
Abstract
Assessing patients clinically through taking the history and performing a physical examination provides the basis for safe and effective clinical practice. Doctors new to general practice can find it difficult to undertake an effective clinical assessment in under 10 minutes, while not missing serious illness. This article outlines strategies for assessing patients in a focused yet patient-centred way and discusses areas that can be particularly difficult.
The GP curriculum and focused clinical assessment
Demonstrate understanding of the context in which the consultation happens Use time and resources effectively Understand the structure of the consultation Use techniques to limit consultation length when appropriate Be able to formulate appropriate diagnoses, rule out serious illness and manage clinical uncertainty Demonstrate in the consultation an ability to adapt communication skills to meet patient needs
Consultation length
Compared to doctors working in secondary care, GPs frequently see unselected and undifferentiated clinical problems. Therefore, they need to be able to perform a focused clinical assessment using organizational and clinical skills at a high level—and often under time constraints—to manage their patients safely and appropriately (Sackett and Rennie, 1992). It can be difficult to assess and manage more complex patients in anything under 15 minutes (Freeman et al., 2002). Howie et al. (1991) state that longer consultations allow GPs to identify and manage psychological problems better, and there is evidence that they may also reduce prescribing and increase health promotion activities (Howie et al., 1999). In part, because of the demand on appointments, many GP surgeries book patients in at 10 minute intervals or even less, which may at times lead to premature closure of consultations or allowing less time for the next patient. Therefore, GPs must make best use of the time that is available to them.
Applying focus
GPs need to be able to integrate clinical and communication skills to understand their patients' symptoms and physical signs as well as other important factors, such as the impact of a medical problem on their lives, health beliefs, worries and expectations about treatment. Freeman et al. (2002) suggest that doctors who directly acknowledge and respond to patient's problems and concerns are those who provide the most effective consultations. A structured and holistic approach in gathering information during clinical assessment therefore helps doctors to apply their understanding of diseases while still being person centred —a process that facilitates evidence-based decisions and effective communication with patients and other professionals. Table 1 gives an example of a possible structure for a focused clinical assessment of a common clinical problem (these are only suggestions for possible points to consider—it may not be possible to cover them all within a single 10 minute appointment).
Case study

Data gathering
The history in the GP consultation is a powerful tool to deal with the majority of problems that we face in everyday general practice. If a patient presents with various undifferentiated symptoms and little in terms of clinical signs, taking a well-organized history and gathering data systematically will give you a solid basis for guiding your physical examination and making clinical judgements.
Being patient centred
Adopting a non-interrogative and non-threatening approach to history taking allows patients to come forward with their own ideas, worries and thoughts about their problem and possible management options, which not only increases patient satisfaction and adherence to treatment but will also give you more valuable information (Roter and Hall, 1987). Box 1 suggests ways to make your consultations more patient centred.
Becoming more patient centred
Stand up and greet your patient and make eye contact Provide a calm and relaxed ambience, even if you feel rushed Through your body language signal to your patient that you are interested and committed (e.g. use eye contact, initially face your patient and not the computer, put your pen down and give undivided attention) Address the person's ideas, concerns, expectations, preferences, feelings and needs and find out about the impact of the problem on day-to-day life Show that you care and that you want to find out what's really going on Share your thoughts and ideas about diagnosis and management Be aware and show respect to issues of diversity, equality and ethnicity
Using communication skills
Various communication techniques are available to find out about the reason for patients' attendance, gain an understanding of their illness experience, gather data effectively and take a shared approach to managing problems (Thistlethwaite and Morris, 2006). Open questions (see Box 2 for some useful examples) can be particularly helpful to find out the reason for a person's attendance and to spot a hidden agenda or a potential ethical dilemma. Open questions can help to identify psychological or social issues, which will often be useful for putting the presenting problem in context. We have to acknowledge, however, that it can be difficult to be patient centred and ask open questions when time is limited—but a focused clinical assessment does certainly not preclude you from being patient centred.
Examples of useful open questions
What can I do for you? What prompted you to make the appointment today? How do you feel in general terms? Tell me how it all started Tell me (more) about … And then …? What did you do …? Can you explain this to me in a bit more detail? Have you had any thoughts as to what I might be able to do for you today?
Try to achieve a good balance between open and closed questions. Open questions are useful for identifying issues important and relevant to the patient, which you can then illuminate further with the use of more closed questions. Closed questions can help obtaining further details about a problem but have the potential to make the consultation less patient centred. Box 3 contains some tips for asking closed questions.
Tips for asking closed questions
Avoid too many direct questions, particularly at the beginning of the consultation Warn patients that you will be asking a set of brief and quick closed questions, which can help them focus Use closed questions mainly to explore your diagnostic hypotheses, to clarify the person's answers and to establish the time course of any events
Using a patient-centred approach not only provides you with higher quality information but may also save you time because you increase the chances of identifying relevant problems early in the consultation. This also creates the foundations for sharing the management plan.
When gathering data, use terms and explanations that are unambiguous and easy to understand. Also be aware of the importance of non-verbal messages that you receive from the patient—and the ones that you may project (Silverman and Kinnersley, 2010), like showing lack of interest by looking out of the window or frequently looking at your watch. You can enhance the consultation in a patient-centred way by providing relevant patient information leaflets (PILs) containing important diagnostic, prognostic and safety netting advice as well as evidence with regard to pharmacological and non-pharmacological treatments that you have recommended. Generally speaking, each consultation has its own momentum and requires a different approach tailored to the individual as well as an awareness of how to avoid common questioning errors (Box 4).
Avoiding questioning errors
Try not to use ‘leading questions’ (e.g. ‘You haven't passed black tarry stools, have you?’) Listen actively to what the patient is saying and respond appropriately Don't ignore patient cues (Patient: ‘Yesterday I bled so much that I stained a car seat, which was very embarrassing’. Doctor: ‘So, tell me: have you lost any weight?’
Symptoms in general practice
Summerton (2007) reminds us that the impact of symptoms depends on the disease prevalence. To use the example from the case history described earlier (see Table 1), the prevalence of colorectal cancer in patients presenting with rectal bleeding is lower in patients presenting in general practice compared to preselected patients in secondary care. Therefore, it makes sense to gather clinical data bearing in mind the probabilities of underlying disease. Incorrectly estimating the prior probabilities for specific clinical conditions is a common heuristic diagnostic error.
Symptoms encountered in general practice are also special in other ways. GPs often face diseases in their early stages when symptoms may change over time. The duration of the illness and individual patient characteristics may also affect the way in which we need to interpret a particular symptom (Summerton, 2004). Patients commonly present with multiple problems, and it can be tricky to find out if these are separate entities or related to an overarching problem, which may include both physical as well as psychological features.
Excluding serious pathology
An important aspect of the initial data gathering is to exclude serious organic pathology, particularly when faced with non-specific symptoms, such as weight loss, being tired all the time or feeling generally unwell for no apparent reason. Systematically searching for important symptoms and being aware of their implications can help identify diagnoses that you should try not to miss and increases the chances of diagnosing serious disease, such as cancer earlier (Jones et al., 2007). Alarm symptoms (or ‘red flags’) can help to ‘rule in’ potentially serious disease, so by eliciting other features in addition to the presenting complaint you can increase or decrease the probability of an underlying condition. ‘Rule out’ questions would relate to questions where a negative answer would help to rule out a certain underlying condition (e.g. the absence of radiation in low back pain helps to rule out disc protrusion).
Building up a mental picture
Taking the history and gathering information as part of the focused clinical assessment is a highly active process, during which you need to be able to think on different levels simultaneously. It helps to be flexible, systematic and holistic to try and build up a mental picture of what is really going on with the patient in front of you. While taking the history, use the information that you gather to plan your physical examination and think of which signs you want to look out for.
Physical examination
Compared to the ‘full’ top-to-toe physical examination traditionally taught at many medical schools, GPs need to be able to adopt a focused and selective examination that is tailored to the findings from the history. The main aim of the physical examination is to rule in your working diagnosis and to rule out other and potentially serious conditions that have entered your differential diagnosis. Make sure that you maintain your skills in using standard medical instruments that you are likely to need frequently (see Box 5).
Standard clinical instruments for the GP consultation
Tape measure Thermometer Sphygmomanometer (aneroid or electric) Stethoscope Ophthalmoscope Auroscope Patella hammer Peak flow meter with disposable mouthpieces
Apart from helping with making a diagnosis, the physical examination has other functions too (Summerton, 2007). Be aware that your patient may expect a physical examination, even if this is unlikely to show up any abnormality or change your management. A normal examination together with an explanation of your findings (or lack thereof) can be very reassuring, like, for example, a chest auscultation in respiratory infections or checking the ears in babies. By performing an appropriate examination, you also show that you take the person seriously and that you care, which can help with establishing rapport. Opportunistic checks may show up unexpected underlying disease (such as hypertension or asymptomatic atrial fibrillation in older people). But remember that by performing a physical examination, you may ‘justify’ and reinforce a patient's help-seeking behaviour, such as consulting for minor colds.
A general inspection can help with pattern recognition, particularly in dermatological problems and multisystem conditions. As a general rule, measure and record the vital signs in every patient who appears unwell. Abnormal vital signs can be an indicator for more serious underlying disease (e.g. asthma or pulmonary embolus), whereas normal vital signs on the whole mean that a serious cause is less likely. At all times during the physical examination stay sensitive to the patient's feelings and be alert to non-verbal cues.
Diagnostic strategies
Heneghan et al. (2009) formally recognized and described three stages of the diagnostic process that GPs use in routine consultations (see Table 2). These strategies may be used interchangeably, depending on the clinical situation. More than one strategy may be used during each stage.
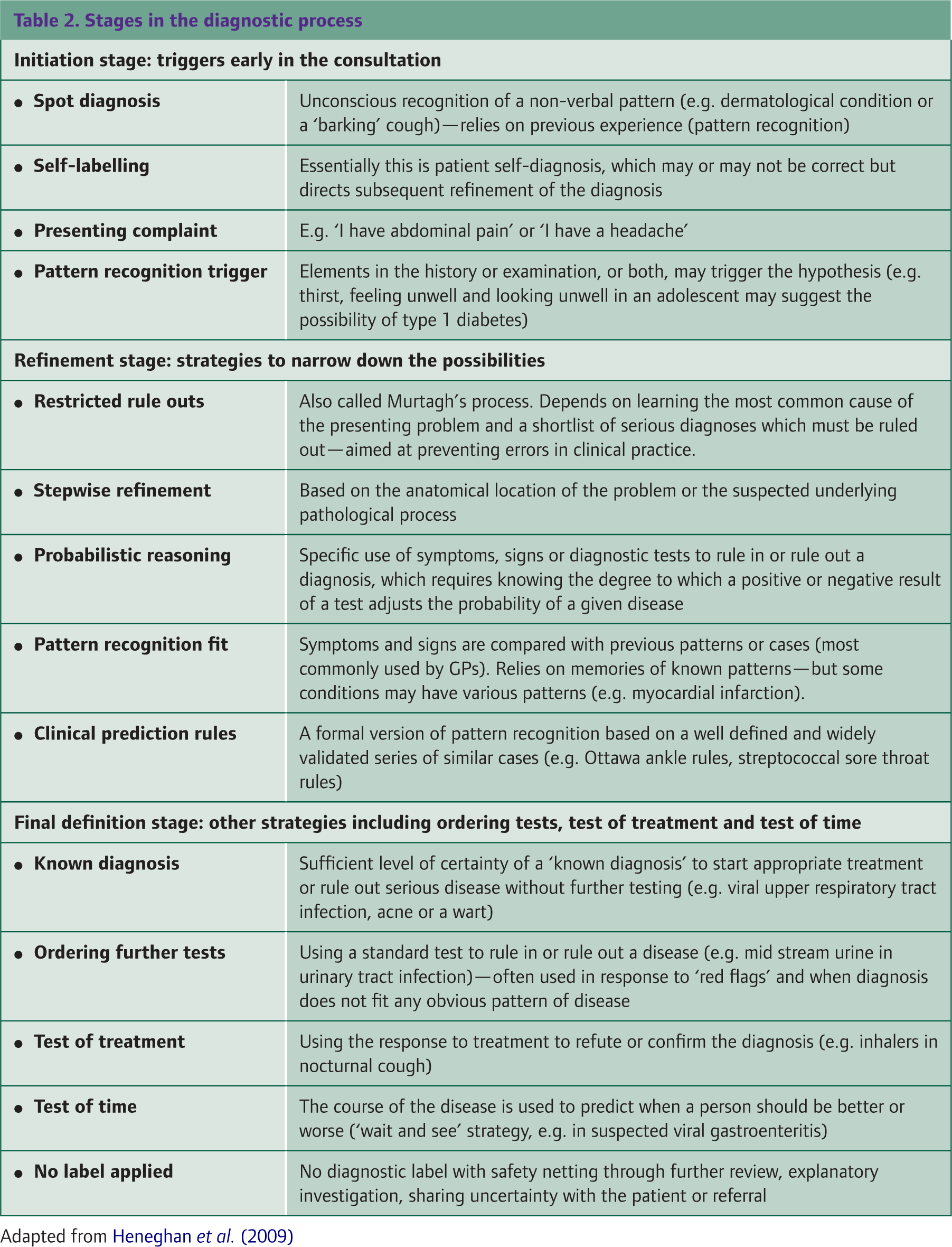
Remember that physical signs are not always reliable. Adapt your choice of diagnostic strategy to the clinical presentation and always consider the context in which a person presents. Take into account any co-morbid conditions as well as the availability of diagnostic tests and other contextual information.
Clinical prediction rules
Clinical prediction rules (CPRs) may be used to try and identify patients with underlying pathology (e.g. bacterial versus viral) or to distinguish between mild and serious illness. They provide a structured approach to individualizing care by calculating a probability estimate from key variables that predict the risk of a future event—typically a diagnosis or prognosis. CPRs have the potential to reduce clinical uncertainty as to which patients are least or most likely to experience complications and which patients are least or most likely to benefit from certain treatments. Table 3 summarizes some important diagnostic terms from what is called the ‘Bayesian’ approach.
Common Bayesian terms

Diagnostic testing
Near patient testing (such as urine dipstick and blood glucose) can be useful for diagnosis and management of clinical conditions. Make sure that you use diagnostic testing judiciously and think about how a test will affect your management. To make this decision, consider the pretest probability of your diagnosis and estimate how the test may or may not alter disease probabilities.
Clinical management
A focused yet with regard to the presenting complaint comprehensive clinical assessment is the cornerstone for recognizing and managing symptoms and medical conditions in general practice. Try to maintain a flexible approach when making decisions and use the strategies mentioned earlier to deal with multiple complaints and co-morbidity effectively. By adopting a focused and patient-centred approach, you will create the foundations for your management plan, which should take into account best practice. While you assess a person clinically, always consider collecting information that will be relevant for follow-up and safety netting, e.g. whether she or he lives alone. And remember that you do not have to achieve everything in a single consultation—you have the option to use time and review the patient at a later stage as appropriate.
Integrating information technology
Using computers have become part of the ‘modern’ GP consultation. Information technology can help provide almost instant access to medical information via the Internet (see Box 6) or through mobile telephone-mediated applications (e.g. ‘Differential Diagnosis iPhone App from the BMJ Group’), which can be downloaded and is not limited to use in the consulting room only.
Helpful websites for use in the consultation
Clinical Knowledge Summaries, www.cks.nhs.uk
GP Notebook, www.gpnotebook.co.uk
National Institute for Health and Clinical Excellence (NICE), www.nice.org.uk
Patient UK, www.patient.co.uk
Scottish Intercollegiate Guidelines Network (SIGN), www.sign.ac.uk
The Internet also allows you to search for up-to-date diagnostic guidelines (e.g. from the National Institute for Health and Clinical Excellence, www.nice.org.uk) as well as CPRs via electronic medical journals or preprogrammed on the computer (e.g. the QRisk2 score, www.qrisk.org.uk). There is evidence that computers have the potential to improve clinical performance (Montgomery and Fahey, 1998). Using computers effectively may save you time and may help to avoid errors (Chan and McGlade, 2003). Although computers may change the flow of the GP consultation (Silverman and Kinnersley, 2010), research suggests that GPs appropriately reduce computer use in consultations that focus on psychological problems (Chan et al., 2008).
Many GPs use information technology to provide their patients with additional and often more detailed information through PILs, which can be downloaded from sites, such as Patient UK (www.patient.co.uk). This can also be useful for safety netting (e.g. head injury advice).
Avoiding errors
We are much more likely to make errors in clinical reasoning because of the way that we think in complex situations rather than due to incompetence or lack of knowledge (Scott, 2009). Cultivating self-awareness (e.g. feeling tired, lack of clinical skills, lack of motivation or urgency to finish) may help prevent errors in clinical practice (Borrell-Carrió and Epstein, 2004). Common errors include wrongly estimating the pretest probability of a condition or failure to review the original hypothesis, which may be affected by clinicians' prior experience and the setting in which they have worked (Fahey and van der Lei, 2008). A good rule of thumb is to become sceptical and review your initial diagnosis when a patient presents more than twice for the same problem. Good communication skills, identifying red flags, checking the vital signs and careful record keeping are all important to avoid being sued (Panting, 2004).
Try and keep up-to-date with medical developments, which can help with remembering to ask patients the critical and discriminating questions that are helpful when making a diagnosis. In addition, ensure you scan the medical notes and correspondence for information that may be useful (e.g. drug history, allergies, previous medical and social problems, previous investigations or hospital attendances). Be even more cautious in consultations that for various reasons are particularly challenging (see Box 7).
Challenging clinical presentations
Long-standing symptoms Multiple attendances for the same problem Mismatch between symptoms and the patient's distress Unexplained aggression Difficulty making sense of the clinical presentation Long list of problems
Note keeping
An essential part of the focused clinical assessment is to keep contemporary and concise yet comprehensive case notes. In addition to providing clinical details, good notes also give a ‘feel’ for how the consultation went and provide insight into your thought processes. A good and simple framework is to use the ‘SOAP’ acronym, which is an acronym for the headings for ‘subjective’ (i.e. what the patient told you) and ‘objective’ findings (results from your clinical examination), your ‘assessment’ (diagnosis and possible differential diagnoses as well as your impression of progress or prognosis) and your management plan (including investigations and therapy). Box 8 summarizes features important for good record keeping, which is an integral part of your clinical care and essential for medico-legal reasons (MPS, 2010).
Items to include in your case notes
Key points
Focused clinical assessment is a highly active process that works on various levels Being able to make good clinical decisions depends on gathering and making best use of high quality information from a focused history and clinical examination Integrate findings from your assessment with additional information from clinical records and other resources (e.g. CPRs, decision aids), which may be available electronically during the consultation Be patient centred in your approach and keep asking yourself the right questions Always document your findings and write contemporaneous, comprehensive yet concise case notes