
Abstract
Bronchiectasis is a term that encompasses the clinical manifestation and pathological findings of patients with chronic bronchial inflammation leading to permanent bronchial architectural distortion. This structural change is the underlying cause for recurrent lower respiratory tract infections (LRTIs) and the condition's characteristic symptoms. The aim of this article is to provide a concise overview of non-cystic fibrosis bronchiectasis (henceforth termed ‘bronchiectasis’ for the purpose of this article) based on the recently published British Thoracic Society (BTS) guidelines and the role of primary care in its management.
The GP curriculum and bronchiectasis
Respiratory problems are among the most common reasons for general practice consultations and emergency medical admission to hospital. The symptoms in the knowledge base of
GPs should:
Be able to manage primary contact with patients who have a respiratory problem Encourage full patient involvement in the management of respiratory conditions Coordinate the patients' care with other primary care health professionals such as practice nurses, district nurses and physiotherapists, to enable chronic disease management and pulmonary rehabilitation Prescribe antibiotics appropriately in order to reduce the development of antimicrobial resistance Be able to describe the indications for urgent referral to specialist respiratory services Demonstrate empathy and compassion towards patients with incurable disabling respiratory conditions. This includes appreciating the importance of the social and psychological impact of respiratory problems on the patient's family, friends, dependants and employers as well as communicating prognosis truthfully and sensitively to patients with incurable disabling respiratory conditions.
Epidemiology
The incidence and prevalence of bronchiectasis are largely unknown. Although it varies between population samples, generally it has been felt that the incidence is decreasing due to a decrease in severe respiratory infections. However, in the context of an ageing population in the western hemisphere and the link between bronchiectasis and increasing age, rates may increase in the future.
Clinical presentation
Bronchiectasis is classically characterized by chronic cough with daily production of mucopurulent sputum. Other less specific symptoms include dyspnoea, wheezing, sinusitis, chest pain and haemoptysis. Clinical examination might reveal coarse bi-basal crackles and wheezing on pulmonary auscultation but extra-pulmonary features such as clubbing are now very rare. Box 1 lists the recommendations of the BTS regarding patients in whom bronchiectasis should be considered as a diagnosis.
One of the key points to elicit when taking a history is to ascertain the presence of recurrent LRTIs. The direction of further history taking should be guided by the need to exclude/confirm the various aetiologies of the condition (see Table 1). For example, patients should be questioned about the presence of arthralgia or be assessed for the risk of TB.
Aetiology of bronchiectasis
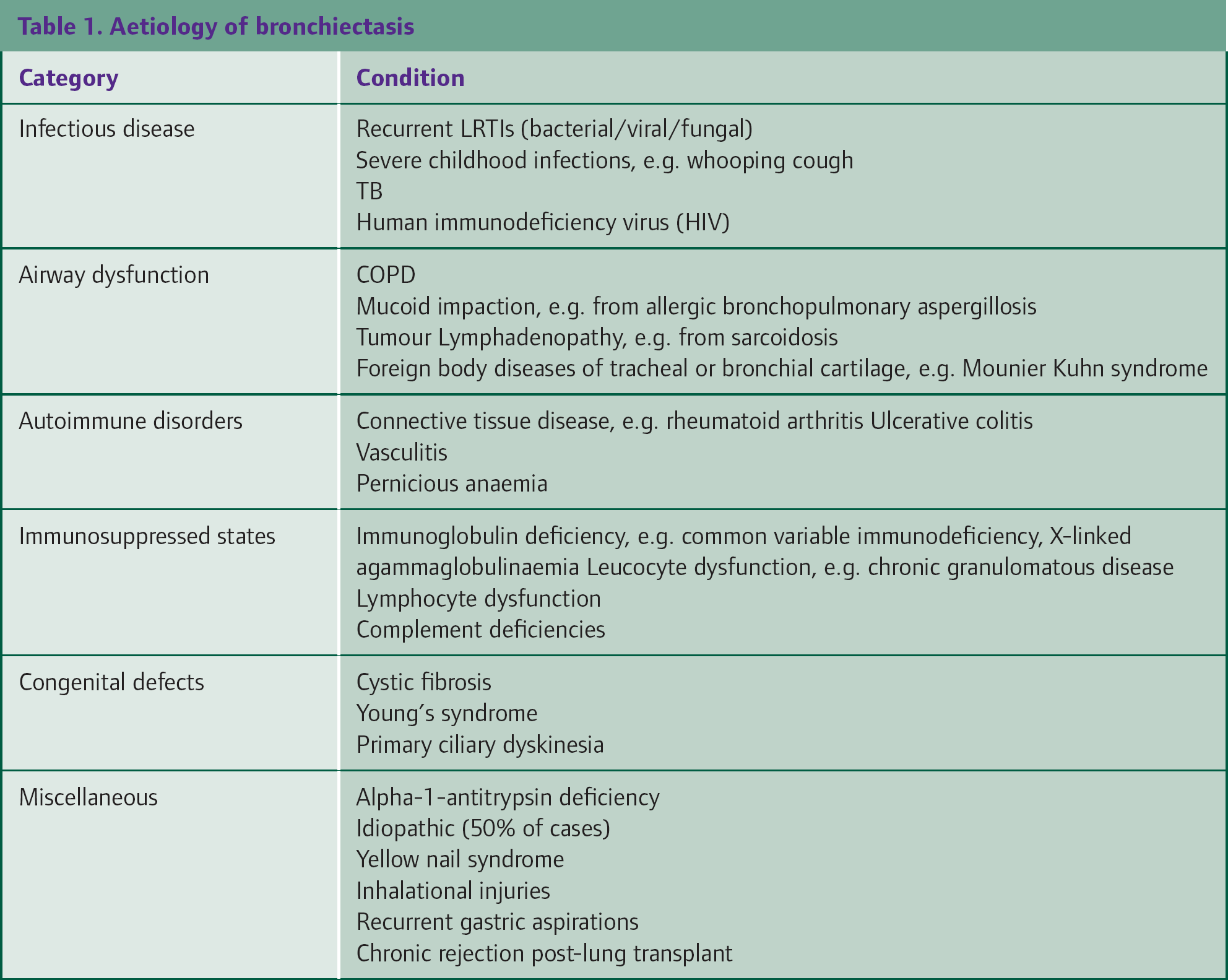
Bronchiectasis is also associated with a number of complications. Some are directly related to the disease, e.g. haemoptysis and a higher rate of influenza and pneumonia. Other less well known complications are sinusitis, arthropathy and urinary incontinence. These should be treated in a similar manner as primary manifestations of these symptoms.
Bronchiectasis should be considered in adults who have:
Persistent productive cough. Any one of the following factors favours further investigation:
Presentation at a young age History of symptoms over many years Absence of smoking history Daily sputum expectoration Haemoptysis Sputum colonization with Pseudomonas aeruginosa, Aspergillus or non-tuberculous mycobacteria (NTM) Unexplained haemoptysis or non-productive cough
Patients thought to have chronic obstructive pulmonary disease (COPD) might have bronchiectasis; referral to secondary care is recommended if:
Management is not straightforward, e.g. recurrent exacerbations Slow recovery from lower respiratory tract infections Absence of smoking history
It should be noted that the term ‘traction bronchiectasis’ is used for bronchial dilatation secondary to pulmonary fibrosis. It is a separate clinical phenomenon from the bronchiectasis described above, with no predisposition to recurrent LRTIs and should therefore be treated as a separate entity.
Investigations
Investigations are aimed at confirming the diagnosis of bronchiectasis as well as identifying its aetiology, specifically targeting any treatable conditions. Investigations also serve to provide a baseline for disease and functional assessment. Naturally, the investigations performed at primary care level would be dependent upon available facilities.
Blood tests
A full blood count can be normal. However, it might reveal mildly elevated white cell count, anaemia, polycythaemia (in the presence of chronic hypoxia), eosinophilia [suggestive of asthma or allergic bronchopulmonary aspergillosis (ABPA)] or neutrophilia (suggestive of chronic inflammation).
An abnormal liver function test might lead one to the diagnosis of alpha-1-antitripsin deficiency. In view of the importance of recognizing immune dysfunction as a possible cause of suspected aetiology, guidelines recommend sending an autoimmune screen and total immunoglobulin levels and functional titres (for vaccine response).
Sputum samples
Sputum samples should be sent for culture for microorganisms and antibiotic sensitivities (bacterial/fungal). A request to look for acid-fast bacilli would be appropriate under suitable clinical circumstances. Culture that is positive for P. aeruginosa is suggestive of bronchiectasis and should prompt patient referral to secondary care.
Radiological imaging
A chest x-ray should be requested. Although images might appear pristine, abnormalities associated with bronchiectasis include linear atelectasis, ‘tram’ lines (dilated, thick-walled bronchi appearing as thin opacified lines), ‘signet rings’ (pulmonary arteries adjacent to dilated bronchi when viewed on end) and thick, peripheral linear opacifications that are suggestive of secretions. On rare occasions, gross abnormalities such as those shown in Fig. 1 are apparent.

Severe cystic bronchiectasis (note: patients usually present with a normal chest x-ray).
It may be sufficient for a diagnosis to be made based on clinical and x-ray findings alone if disease progression has been severe, but referring a patient for a high-resolution computed tomography (HRCT) scan enables the detection of mild and moderate disease and provides a baseline for future reference.
Spirometry
Spirometry usually reveals an obstructive picture, although it can occasionally reveal a mixed or even restrictive pattern. Patients should be referred for full pulmonary function tests to measure peak expiratory flow, lung volumes, diffusion capacity as well as to test for reversibility.
Non-medical management
Lifestyle changes
As with all chronic respiratory conditions, patients should be encouraged to stop smoking. While this may not have an impact on bronchiectasis per se, it does have an effect on underlying lung function.
Chest physiotherapy
Patients with bronchiectasis should be referred to an experienced physiotherapist to be trained to use appropriate techniques to help clear respiratory secretions or as part of pulmonary rehabilitation. Physiotherapy plays an important role in the management of bronchiectasis by loosening and improving sputum clearance. This is particularly important for those who have evidence of mucus plugging. Airway clearance techniques (e.g. postural drainage) and the use of positive expiratory pressure devices (e.g. Flutter and Acapella) have been shown to improve sputum clearance and this is a worthwhile form of therapy in patients who are sufficiently motivated. The most appropriate form of physiotherapy will be dictated by patient preference and lifestyle.
Psychological care
Patients with bronchiectasis have increased depression and anxiety levels with subsequent lower quality of life. Levels of depression have been correlated with increasing dyspnoea and the presence of the haemoptysis and high-volume sputum production is usually a cause for concern with patients.
With this in mind, it is essential to identify the patient's ideas of the disease and to deal with his/her concerns and expectations appropriately. This enables patients to be actively involved in their management plan and thereby empowers them. Our experience is that patients feel more confident after seeing a specialist.
Medical management
The aim of treatment is to improve the patients' quality of life by decreasing the number of exacerbations and controlling symptoms.
Bronchodilators
Bronchodilators are used to treat bronchial hyper-reactivity and are particularly useful in patients with underlying asthma or COPD who demonstrate reversibility and symptomatic improvement. Although bronchiectatic patients without asthma or COPD are routinely given bronchodilators, there is a lack of evidence to support this. There is also no role for the use of long-term steroids in these patients, although short courses of oral steroids can be helpful in acute exacerbations and should be prescribed as appropriate.
Expectorants
Some patients may describe difficulty expectorating due to increased sputum viscosity. While the mainstay of management would be chest physiotherapy, these patients may benefit from the addition of a mucolytic, e.g. carbocisteine. This should be started at a dose of 750 mg three times a day and reduced to 375 mg three times a day as condition improves. It should be stopped after 4 weeks if the patient does not display any clinical benefit.
There is also evidence that normal and hypertonic saline nebulizers aid sputum clearance. The feasibility and suitability of these forms of treatment are considered at secondary care level.
Antibiotics for acute exacerbations
Antibiotics should be given during acute infective exacerbations. These are characterized by progressive symptoms (cough, increased sputum volume/change in viscosity, increased sputum purulence, increase wheeze, dyspnoea and haemoptysis) or systemic symptoms.
Culture and sensitivity of sputum samples form the basis of anti microbial management. In the management of acute exacerbations, it is imperative that sputum samples are sent to microbiology labs within 3 hours, as some microorganisms such as Haemophilus influenzae and Streptococcus pneumoniae might die within this time period. The 3 hour time limit may not be practical in certain circumstances. In these situations, it would be necessary to tamper negative findings with the patient's clinical presentation. Care should be given to differentiate microorganisms that are causing infective exacerbations and those that are colonizing the patient, e.g. at least two isolates of an organism 3 months apart over 1 year.
The need for hospital admission during an acute exacerbation is guided by a mixture of disease severity as well as local resources (see Box 2). Empirical antibiotics should be started while awaiting results from the microbiology laboratory but choice should be guided by previous cultures and sensitivities where available. Recommended first-line empirical treatment is either amoxicillin 500 mg three times a day or clarithromycin 500 mg twice a day for a total of 14 days. Ciprofloxacin 500 mg twice daily is recommended in patients who have had previous growth of P. aeruginosa. Antibiotics should then be adjusted in light of subsequent sputum sensitivities.
Criteria for inpatient treatment
Unable to cope at home Cyanosed Delirium Dyspnoea with respiratory rate of 25 breaths per minute or more Circulatory or respiratory failure Temperature of 38°C or greater Unable to take oral therapy or prior history of infection with a multi-resistant organism Intravenous therapy required in patients with clinical failure after oral antibiotics
Management of haemoptysis
Small amounts of haemoptysis are typical of infective exacerbations and can be managed conservatively. Occasionally, the use of procoagulant agents such as tranexamic acid are warranted. In massive haemoptysis (100 −600 ml over 24 hours), the patient should be referred urgently to a hospital for computed tomography (CT) scan with a view to performing bronchial artery embolization.
Long-term antimicrobial therapy
Macrolide antibiotics such as azithromycin have been shown to have an immunomodulatory effect on the body's inflammatory responses to bacteria. These have been shown to improve symptoms and are prescribed for patients with three or more exacerbations per year requiring antibiotic therapy. The prescription of macrolides should be tempered by the realization that they are not without side effects.
A similar cohort of patients could benefit from the use of long-term nebulized antibiotics, e.g. colomycin or tobramycin that act as anti-pseudomonal agents. Long-term antibiotics should be prescribed on a case-by-case basis at secondary or tertiary levels of care.
Important pathogens
In adult bronchiectasis, the most common microorganism grown is H. influenzae. This is followed by other pathogens that cause LRTIs, e.g. S. pneumoniae, Moraxella catarrhalis and Staphylococcus aureus.
However, the most significant pathogen in patients with bronchiectasis is P. aeruginosa. This microorganism behaves in a virulent manner in patients with bronchiectasis and leads to a poorer quality of life, faster rates of decline in fixed expiratory volume in one second (FEV1) and increased number of hospitalizations. Patients with evidence of P. aeruginosa growth should be followed up in secondary care, where aggressive attempts will be made to eradicate it.
Surgery
In a small cohort of patients, surgery might be a management option. However, this is only suitable for patients with focal bronchiectasis who do not show clinical improvement despite maximal medical therapy. In a further highly selected group of patients with end-stage respiratory disease, lung transplantation can be considered.
Vaccination
As with all patients with chronic respiratory disease, seasonal influenza and pneumococcal vaccines should be offered to patients with bronchiectasis. Immunization can lead to decreased frequency of exacerbations, although data are admittedly limited in this group of patients.
Monitoring progress
Regular monitoring would help ensure that therapeutic aims are achieved. The BTS recommends that the following data should be recorded for disease monitoring:
Annual spirometry Number of exacerbations and which antibiotics were taken in the follow-up period Estimated sputum volume per day and sputum character Result of sputum culture Daily symptoms and the degree of disturbance of activities of daily life Concordance with treatment Specific concerns from the patient
Routine repetition of chest x-rays to monitor progression is not recommended. Chest x-ray should only be requested when there is a clinical need. Box 3 lists patients who are at a higher risk of poorer outcomes or need easier access to inpatient facilities and should be referred to secondary care as an outpatient.
Prognosis
There is no conclusive evidence that bronchiectasis leads to increased mortality. However, it is worth noting that the mean annual decline of FEV1 in patients with bronchiectasis is 50–55 ml/year, which is similar to those who have COPD. This decline is more marked in patients with frequent exacerbations, P. aeruginosa colonization and increased inflammatory markers.
Patients who should have follow-up in secondary care
Patients with advanced disease or those being considered for lung transplantation Patients with chronic P. aeruginosa, opportunist mycobacteria or methicillin-resistant Staphylococcus aureus (MRSA) colonization Deteriorating bronchiectasis with declining lung function More than three exacerbations per year Patients receiving prophylactic antibiotic therapy Patients with the bronchiectasis and the following conditions:
Rheumatoid arthritis Immune deficiency inflammatory bowel disease Primary ciliary dyskinesia ABPA
Key points
Bronchiectasis is often underdiagnosed and should be considered in patients with a copious amount of sputum production on a background of recurrent LRTIs Basic investigations include blood tests, radiological imaging and sputum microbiology. If these investigations are suggestive of bronchiectasis, the patient should be referred to a respiratory physician for secondary care review. Antibiotic use should be guided by sputum culture and sensitivity Chest physiotherapy is highly effective Patients with P. aeruginosa colonization have poorer outcomes. These patients will need continued follow-up at secondary care level.