
Abstract
The prevalence of dyspepsia is 25–40% and it is a common presenting symptom in general practice consultations. Only a small percentage of patients have any organic pathology; the remainder have functional (idiopathic) dyspepsia, which can result in significant morbidity as well as significant costs to the health service when not managed appropriately. As most patients with dyspepsia are managed in the community, GPs should have a framework from which they can manage dyspepsia and understand when it is appropriate to refer for further investigations, such as upper gastrointestinal (GI) endoscopy.
The GP curriculum and dyspepsia
Summarize the debate about the role of upper GI endoscopy in the management of dyspepsia Demonstrate a consistent evidence-based approach to prescribing for dyspepsia Recognize the effects psychological stress can have upon the GI tract, especially with functional disorders Demonstrate a non-judgemental caring and professional consulting style to minimize embarrassment of patients with digestive problems.
Definition of dyspepsia
Dyspepsia is defined as having epigastric pain or discomfort, which can encompass postprandial fullness and early satiety (Rome Foundation, 2006). Patients often use the term ‘indi gestion’ to describe their symptoms. Heartburn is excluded from the criteria as this suggests gastro-oesophageal reflux disease (GORD), although dyspepsia and GORD can occur concomitantly.
Functional dyspepsia is defined as dyspepsia symptoms of greater than 3 months duration, with onset at least 6 months prior to diagnosis and without any anatomical, systemic and metabolic abnormality. It often has a relapsing remitting course. There is a large overlap between functional dyspepsia and irritable bowel syndrome (IBS).
There is often much confusion between dyspepsia and GORD. However, dyspepsia is a symptom whereas GORD represents a collection of diseases caused by gastro-oesophageal reflux. Retrosternal heartburn and acid reflux are the principal presenting complaints in patients with GORD.
Epidemiology
The prevalence of dyspepsia is around 40% and it is a common presenting symptom in general practice. It is thought to be the main presenting complaint in 5% of all consultations every year. Annually, approximately 1% of patients will undergo upper GI endoscopy [National Institute for Health and Clinical Excellence (NICE, 2005a)]
Causes
The five main causes of dyspepsia are
Functional dyspepsia Medication-induced dyspepsia Gastro-oesophageal reflux (erosive and non-erosive) Peptic ulcer disease and Malignancy.
The most common cause is functional dyspepsia (50%). In those that do undergo endoscopy, approximately 40% have functional dyspepsia, 40 % have GORD, 13% have some form of ulceration and only around 3% have oesophageal or gastric malignancy (NICE, 2005a).
Other less common causes of dyspepsia include hepatobiliary disease, acute and chronic pancreatitis, metabolic disorders such as hypercalcaemia and systemic disease such as connective tissue diseases. It is important to keep in mind cardiac causes as part of the differential diagnosis in patients presenting with dyspeptia-like symptoms.
Referral criteria for endoscopy
Universal investigation of all patients with dyspepsia is neither affordable nor desirable. There is no indication for routine endoscopic investigation in dyspeptic patients under the age of 55 years who do not have any red flag features. Alarm symptoms that require urgent referral for endoscopy are listed in Box 1. For patients over the age of 55 years, in addition to urgent referral for upper GI endoscopy for patients with red flag features, NICE (2005a) recommends urgent referral for any patient with unexplained and persistent recent-onset dyspepsia alone.
Symptoms that require urgent referral for endoscopy for patients of any age
Chronic gastrointestinal bleeding Progressive unintentional weight loss Progressive difficulty swallowing (dysphagia) Persistent vomiting Iron deficiency anaemia Epigastric mass or suspicious barium meal
Management of uninvestigated dyspepsia
Lifestyle advice
Offer all patients with dyspepsia lifestyle advice including weight reduction and recognizing precipitants, such as stress, alcohol, caffeine and smoking. Other measures can include propping up the head of the bed, introducing smaller, more frequent meals and avoiding precipitants such as fatty foods.
Antacids
Educating patients about the role of antacids and/or alginates in the self-management of dyspepsia is important. Antacids are usually magnesium based, aluminium based and less commonly calcium based and are best used when symptoms are present or expected. This is usually after meals and at bedtime. Bismuth-containing antacids are no longer recommended (unless chelates) due to the risk of neurotoxicity, which can precipitate encephalopathy. Alginates can be used in combination with antacids. They work by increasing the viscosity of gastric contents and protect the oesophagus from reflux.
Medication review
A medication review is very important but frequently overlooked. Review all the drugs that the patients are taking both on prescription and on over-the-counter in the initial consultation. The most common medications causing dyspepsia are listed in Box 2.
Medications causing dyspepsia
Non-steroidal anti-inflammatory drugs (NSAID) and aspirin Bisphosphonates Corticosteroids Selective serotonin reuptake inhibitors (SSRIs) Serotonin and noradrenaline reuptake inhibitors (SNRIs) Iron preparations Antibiotics e.g. tetracycline Calcium antagonists Nitrates Theophyllines
Dyspeptic symptoms can sometimes also be avoided or reduced if patients are adequately counselled prior to commencing a medication. For example, bisphosphonates should be taken 30 minutes before food or other medication, while sitting upright, and washed down with plenty of water. The patient should remain upright for at least 30 minutes after taking the drug. In addition, when prescribing or recommending a drug known to cause dyspepsia such as a non-steroidal anti-inflammatory or steroid tablets, consider offering patients at high risk a concomitant prescription of a stomach protector such as a proton-pump inhibitor (PPI). High-risk patients include the elderly, those already on other drugs that might irritate the stomach and those with a past history of indigestion or peptic ulceration.
Helicobacter pylori
The role of Helicobacter pylori in functional dyspepsia is a controversial one. Several studies have shown only a modest improvement in dyspeptic symptoms in patients managed in the community once H. pylori has been eradicated.
However, studies have shown that the ‘test and treat’ approach does lead to a reduction in the number of endoscopies with resultant savings to the health service and avoidance of unnecessary investigation for the patient. The NICE (2005a) has no clear preference for whether or not test and treat for H. pylori should be done prior to or as a result of failure of empirical PPI treatment. Either way, in patients being tested for H. pylori, it is essential that they are not on PPI's for at least a 2 week period in order to reduce the likelihood of a false negative result.
Helicobacter pylori testing is done using a Carbon 13 (C-13) urea breath test (CUBT), stool antigen test or serology. Both CUBT and stool antigen test are accurate in detecting H. pylori with a sensitivity and specificity of 92–95%.
Serological testing is inferior (sensitivity 92% and specificity 83%) and antibodies can persist for H. pylori even after eradication [Scottish Intercollegiate Guidelines Network (SIGN, 2003; NICE, 2005a)].
The eradication treatments recommended for adults are summarized in Fig. 1. NICE (2005a) states that eradication is successful in approximately 80–85% of patients. However, this does mean that treatment fails to eradicate H. pylori in approximately one in five patients treated.

H. pylori eradication treatment regimes for adults
Eradication is equally effective in those patients prescribed PAC500 (PPI, amoxicillin and clarithromycin 500 mg) and PMC250 (PPI, metronidazole and clarithromycin 250 mg) regimens. However, PMC250 when used as first-line therapy appears to increase subsequent resistance to both clarithromycin and metronidazole. Amoxicillin resistance appears not to increase after use of PAC500.
NICE (2005a) does not recommend routinely retesting for H. pylori in dyspeptic patients following eradication therapy unless clinically indicated i.e. for those patients that do not respond or relapse after eradication therapy. In patients whom retesting for H. pylori is indicated the choice of test is CUBT. This should not be performed within 2 weeks of PPI therapy or within 4 weeks of antibiotic therapy, to reduce the likelihood of false negatives.
Pharmacological treatment
The NICE recommendations for patients with uninvestigated symptoms are summarized in Fig. 2 (NICE, 2005a). All patients with dyspeptic symptoms should be offered an empirical trial of full-dose PPI therapy for 1 month. PPI therapy should be used in preference to H2 receptor antagonists (H2RA) as trials have shown them to be superior in the control of symptoms, with an average response rate to PPIs of 58% as compared to 36% for H2RAs (NICE, 2005a).
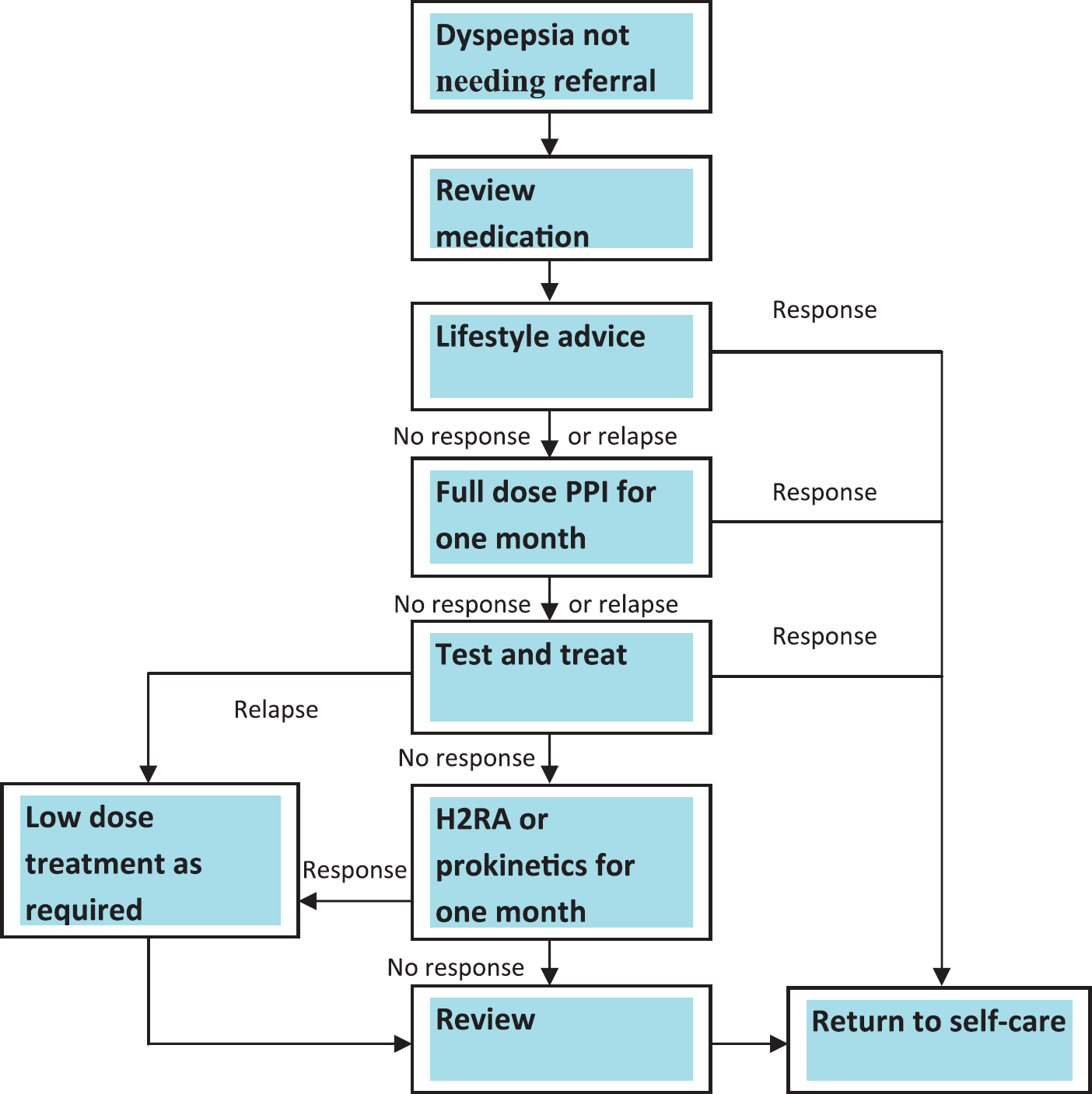
Management of uninvestigated dyspepsia.
For those patients responding to PPI and whose symptoms return after stopping, prescribe the lowest dose needed to control symptoms. Alternatively, advise patients to use their medication as required as part of the self-management of their symptoms.
If there is no response to PPI therapy, alternatives include H2RAs and prokinetics, such as metoclopramide and domperidone. Prokinetics can be used in combination with PPIs when PPI alone has not been effective. Metoclopramide and domperidone work similarly but domperidone has a better side effect profile as it does not cross the blood-brain barrier. The evidence for the effectiveness of prokinetics in the management of functional dyspepsia is limited. If considered, they should be used on a short-term basis only.
Psychosocial aspects
The majority of patients that present to their GP with dyspeptic symptoms have functional dyspepsia. It is important for GPs to address the psychosocial aspect of the condition as part of their overall management strategy. Reassure patients that although the symptoms of functional dyspepsia can be distressing or bothersome, the condition itself is not serious. Encourage patients to take a proactive role in the management of their symptoms.
Cognitive behavioural therapy (CBT) and psychotherapy have been shown to reduce dyspeptic symptoms although they are not currently recommended by NICE (2005a). Unlike for other functional bowel disorders, there is no clear evidence for any beneficial effect of antidepressants, such as tricyclics in the management of dyspepsia.
Follow-up
All patients should be reviewed on annual basis to address their ongoing management, with scaling down of prescription medications if appropriate. Consider seeking a specialist opinion in those patients whose symptoms are not controlled despite the measures detailed in this article.
Key points
Dyspepsia is a common presenting symptom in general practice; only a small proportion of patients will have any significant pathology. Routine endoscopic investigation as part of the management of patients with dyspepsia is not recommended. Any patient with alarm symptoms and patients over the age of 55 years with persistent and recent-onset dyspepsia alone should be referred for urgent endoscopy. Management of dyspepsia should include lifestyle modifications, over-the-counter antacids/alginates, medication review, test and treat for H. pylori and prescription medication. It is important to recognize the large psychosocial aspect of functional dyspepsia and address this as appropriate.