
Abstract
Renal colic is a common condition, which will often be seen by GPs throughout their careers. Making up 1% of all emergency admissions to hospital, specialist review and care may be frequently required; however, the responsibilities of initial prompt diagnosis and treatment, followed by patient education and secondary prevention will often lie with the primary care physician. This article aims to provide an overview of renal tract calculi and provide trainees with a general understanding of its aetiology, presentation and acute and long-term treatment.
The GP curriculum and renal stones and renal colic
Describe differential diagnoses for each presenting symptom Decide whether urgent action is necessary, thus protecting patients with non-urgent and self-limiting problems from the potentially detrimental consequences of being over-investigated, over-treated or deprived of their liberty Recognize patients who are likely to need acute care and offer them advice on prevention, effective self-management and when and who to call for help Demonstrate the use of time as a tool and to use iterative review and safety-netting as appropriate
Epidemiology
Urinary tract calculi represent the single most common cause of acute admission to hospital for a urological cause, making up 1% of all emergency hospital admissions. Population prevalence of calculi is in the region of 0.2% and has a lifetime incidence of 12% in men and 3% in women with a positive family history doubling that risk. First presentation can be without warning at any age; however, generally, its peak incidence follows a bimodal distribution of patients in the early twenties and mid-fifties. An attack of renal colic may be an isolated event in a patients' life or become a recurrent problem, which may have a significant impact on their quality of life with attendant physical and psychosocial morbidity.
History and examination
Suffering renal colic is often considered to be one of the most excruciating experiences a person can go through—it has been described as being the closest a man can come to experiencing the pain of childbirth. Patients tend to describe an acute onset of unilateral pain the site of which can vary loosely depending upon the position of the stone. Renal calculi cause loin pain, whereas ureteric stones can cause a pain radiating towards the groin and those in the lower ureter can cause pain in the testicle or labium.
The pain experienced is typically colicky in nature with a fluctuant course that can last from minutes to hours. Patients classically also suffer nausea and potentially vomiting along with their pain. Patients will be physically restless and unable to settle; this behaviour being in marked contrast to a patient with a peritonitic abdomen who will be suffering a pain exacerbated by movement leaving them reluctant to move at all. It is common to suffer a degree of tenderness on palpation of the loin; however, in simple colic, this will not be exquisite. Certainly, on examination, if features of peritonism, such as rigidity, guarding or rebound tenderness, are present, then another diagnosis is more likely.
Calculi in the lower ureter and bladder may cause irritation precipitating frequency and dysuria and occasionally urinary retention. A mechanical intermittent or complete urinary retention can be caused by stones in the bladder or urethra; however, this is very uncommon as the relative diameter of the lower urinary tract is greater than that of the upper.
Patients very frequently develop microscopic haematuria, which is easily tested for on dipstick. Frank haematuria, while possible, is very uncommon. Dipstick proteinuria in isolation is not associated with urolithiasis. Acute, chronic and recurrent urinary tract infections may also be secondary to calculi (with Proteus species the most prevalent causative organisms). Finally, patients may describe the passage of silt or actual calculi in the urine.
Alternative presentations
One of the most dangerous potential complications of urolithiasis is the development of infection in the urinary tract in the presence of an obstructing calculus. An infected obstructed urinary tract represents a true surgical emergency whereby patients must be admitted immediately to hospital for further investigation and intervention. Suspect this complication if a patient with features typical of renal colic is also demonstrating other signs of systemic sepsis, such as fever and rigours. Urine dipstick positive for leucocytes and nitrites must also attract suspicion. On examination, rather than eliciting a slight tenderness on palpation, the patient may experience a severe tenderness resulting from gross inflammation and destruction of the renal parenchyma.
When assessing any patient with potential renal colic, it is vital to give consideration to any other differential diagnoses in their presentation (see Box 1). The classical misdiagnosis is in not considering a possible ruptured abdominal aortic aneurysm in men over the age of 50 years presenting for the first time with ‘renal colic’. Bilateral loin pain is especially suspicious in this regard.
Potential differential diagnoses in spected renal colic
Pyelonephritis Ureteric obstruction*
Renal abscess Appendicitis Diverticulitis Biliary colic/pancreatitis Ectopic pregnancy Pelvic inflammatory disease Tubo-ovarian disease Myocardial infarction Ruptured/symptomatic abdominal aortic aneurysm Musculoskeletal/traumatic pain Radicular pain
Aetiology of stones and risk factors for stone formation
Many cases of recurrent renal colic arise as a result of a specific metabolic derangement. Therefore, GPs should have some appreciation of biochemical aetiologies so as to be able to consider further underlying diagnoses and long-term treatment options.
Calcium stones make up 75% of all calculi. Excess urinary excretion of calcium is associated with hyperparathyroidism, sarcoidosis and increased gut absorption of calcium. Patients with high dietary oxalate intake or those who have undergone jejuno ileal bypass or Crohn's disease-related intestinal resections may have increased gut absorption of oxalate and therefore formation of calcium stones. Low levels of citrate and magnesium are also associated with stone formation as they prevent the crystallization of calcium in the urine.
Struvite (magnesium ammonium phosphate) stones, also known as infection stones, make up 15% of cases and are universally associated with urinary tract infection. Organisms include Proteus, Pseudomonas and Klebsiella species; these split urea into ammonium, which subsequently precipitates as a salt. Infections will not resolve until the stone is removed. Urinary pH is typically greater than 7.0.
Six per cent of calculi are composed of uric acid, with increased urinary uric acid resulting from conditions such as gout, malignancy, insulin resistance, renal insufficiency and excess consumption of alcohol. Diets high in purines (meats, legumes and fish) are also implicated. Urinary pH is normally less than 5.5.
Cystine stones are less common making up only 2% of all calculi. Cystinuria is a rare autosomal recessive condition where there is decreased reabsorption of cystine resulting in increased excretion and therefore crystallization.
Stones can also result from the use of numerous different medications. Those most commonly implicated include calcium supplements, vitamin D supplements, acetazolamide, sulphonamides, triamterene and indinavir.
Other general risk factors for recurrent stone formation include a strong family history and first presentation at less than 25 years of age. Patients with any anatomical abnormality of the kidney or urogenital tract are also at more risk. Such abnormalities most often take the form of medullary sponge kidney, horseshoe kidney, pelvi–ureteric junction obstruction, caliceal diverticulum and cysts, ureteral strictures or vesico ureteric reflux.
Patients with a single functioning kidney should also be considered to be at increased risk from stones. This is not because the rate of formation is increased, but because the potential complications are much more immediate and devastating.
Investigation of patients in primary care
All patients with renal colic must, as a minimum, have a number of baseline investigations. Patients should have urine dip performed to confirm the presence of haematuria and rule out urinary tract infection through the presence of nitrites and leucocytes. It should be noted though that various studies have differed in the demonstrable degree of accuracy of this test with a false-negative rate of between 10 and 25% being reported. One should therefore bear in mind that in the presence of a convincing history, a negative result cannot be seen to exclude the possible diagnosis of stones.
Urinalysis should be performed for pH and microscopy of sediment for pathognomic crystals. Patients should also be encouraged to sieve their urine in an attempt to catch any stone that is passed. All patients should have a calculus sent for chemical analysis on at least one occasion. This will allow the accurate determination of the nature of the stone allowing further treatment and secondary prevention measures to be explored.
Acute renal failure resulting from an obstructing unilateral calculus is unlikely given the presence of a normally functioning contralateral kidney. However, checking serum creatinine levels remains a recommendation in all patients and is of course absolutely vital in a patient with a history of chronic renal insufficiency or a single functioning kidney. It should be borne in mind that acute obstruction will only be followed by a rise in creatinine levels after a lag of several hours, raising the possibility of falsely negative tests. Serum urate levels should be tested especially if no stone has yet been obtained. The presence of a radiolucent stone on x-ray and high serum urate levels indicates a uric acid calculus. Serum calcium levels should be tested—a calcium level of greater than 2.6 is suggestive of hyperparathyroidism with further testing of calcium and parathyroid hormone levels indicated.
Management of acute renal colic
The first priority is to control the patients' pain and vomiting. The appropriate route will depend upon severity of pain and whether vomiting has compromised the oral route (Table 1).
First-line treatment of pain and nausea in the community
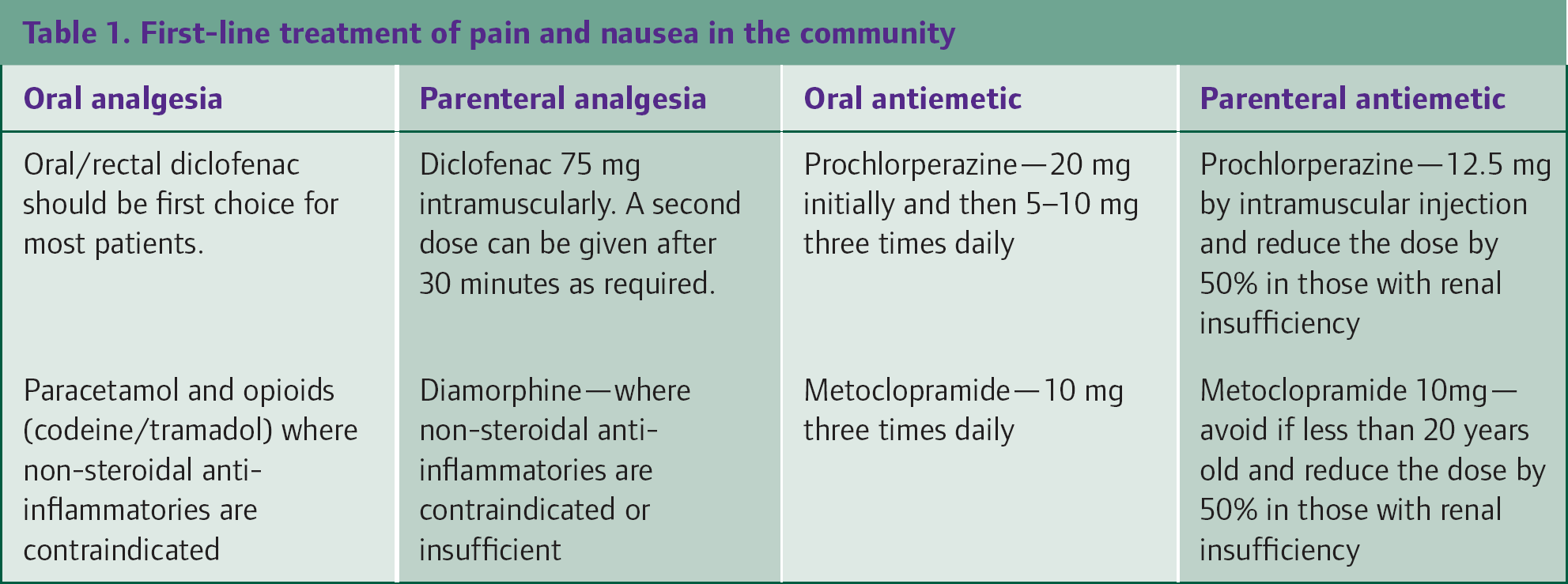
A patient with controllable pain who is systemically well and has no other features of complicated renal colic can be safely managed at home. However, if 1 hour following administration of analgesia pain is worsening or intractable, then admission to hospital should be arranged. Other features indicating that a patient must be admitted urgently to secondary care are listed in Box 2. For those managed at home, they must have a supply of simple analgesics and be given advice on when to seek further medical attention if they have further difficulties.
Indications for admission to hospital in patients with renal colic
Signs of systemic sepsis/fever Worsening or intractable pain Single or transplanted kidney History of chronic renal insufficiency Bilateral obstructing stones are suspected Nausea and vomiting resulting in dehydration Pregnant women—especially in early pregnancy Patients presenting for first time over 60 years of age Where diagnosis is uncertain Patient's wishes or social circumstances necessitating
Where the patient does not require emergency admission, further urological advice should still be sought on an urgent outpatient basis. Any patient who is treated expectantly for renal calculi will require periodic follow-up with imaging to ensure that they are progressively passing their stones.
Investigation of renal tract calculi in secondary care
Depending upon the nature of stone disease, further detailed investigation can be carried out through specialist review to definitely diagnose or exclude underlying conditions. This can take the form of 24 hour urine collections and further blood testing.
Plain abdominal x-ray of the kidney, ureter and bladder (KUB) is a simple, cheap and rapid baseline form of imaging (see Fig. 1) that may provide useful differential information. It has sensitivity in the region of 60%, with calcium-containing stones being radio-opaque. Studies are limited by features such as a patients' body habitus, the presence of prominent bowel gas, calculi elsewhere (for example gallstones), constipation or phleboliths (thrombosed veins in the pelvis that can have the appearance of calculi). In situations where the x-ray is positive, further imaging will still be necessary to characterize the anatomy of the calculi and plan further potential intervention.

Bilateral staghorn calculi
Unenhanced helical computed tomography KUB (CT KUB) is now the accepted gold standard diagnostic investigation according to the British Association of Urological Surgeons (see Fig. 2). It has been shown to have a specificity and sensitivity in the region of 95%, similar or superior to intravenous pyelography (IVP). CT KUB has the advantage that, along with detecting radiolucent stones, it may also detect pathology outside the renal tract. The main disadvantage of CT scanning is the exposure of the patient to high level irradiation and its impracticality as a tool for follow-up in the long term. The European Association of Urology therefore recognizes combining x-ray KUB and ultrasound KUB as a suitable follow-up tool (although not for initial diagnosis).

A CT scan demonstrating a 4 mm calculi in the left mid-ureter (lateral to the superior aspect of the body of the third lumbar vertebrae)
IVP (see Fig. 3), while being accurate, is more limited than CT scanning and will not demonstrate radiolucent stones. Furthermore, IVP carries definite potential risks in terms of possible lactic acidosis in patients treated with metformin and also nephrotoxicity and anaphylaxis to contrast media. For these reasons, IVP will only normally be carried out where CT scanning is unavailable.

A normal IVP
Ultrasonography has a limited but useful role in the diagnosis of urolithiasis. While renal stones and hydronephrosis will be demonstrated, stones in the ureter are poorly visualized. In practice, ultrasound is most often used in the emergency setting of a febrile patient to exclude or guide the drainage of a pyonephrosis. It can also be used safely in pregnant women and children where radiation exposure needs to be avoided. Finally, magnetic resonance imaging (MRI) may also be appropriate on occasions such as in pregnancy to avoid irradiation. It does however have very real drawbacks in terms of scanning times and demands on service from other sources.
Treatment of renal tract calculi in secondary care
Once the size of a stone has been measured, it is possible to predict how likely the stone is to be passed spontaneously. Stones less than 5 mm in size have an 80% chance of spontaneous passage, whereas those greater than 7 mm have a very low chance of being passed.
Medical expulsive therapy
Medical expulsive therapy (MET) is now well established as having an effective role in the expectant management of ureteral (but not renal) calculi. The off-license use of tamsulosin is the most effective drug available. It significantly increases the rates of spontaneous passage and decreases symptoms from stones. Therefore, it should be tried in patients with uncomplicated disease who have no evidence of sepsis and stones less than a centimetre in size.
Indications for stone removal
The European Association of Urology recommends that active stone extraction should be considered if
There is lack of progress in stone passage; in the long term, even relatively asymptomatic stones will cause problems Calculi greater than 7 mm in size (due to lower rates of spontaneous expulsion) Smaller stones that are lodged in a renal calyx Where pain relief cannot be achieved through conservative measures In the presence of a single kidney, especially if there is felt to be any risk of obstruction Bilateral urinary tract obstruction
Certainly, any patient with an infected obstructed urinary tract system will require emergency decompression and draining either percutaneously or through stenting.
Extracorporeal shockwave lithotripsy
Extracorporeal shockwave lithotripsy (ESWL) has a success rate of greater than 90% in smaller renal stones and is the safest form of surgical intervention. Potential complications include hydronephrosis (from obstructing fragments), fever, urinary sepsis and damaging the renal tracts from repeated episodes of ESWL. Contraindications to the procedure include pregnancy, severe obesity, coagulopathy and active urosepsis, which must be resolved in advance of the treatment.
Percutaneous nephrolithotomy
Percutaneous nephrolithotomy tends to be reserved for larger stones. This procedure is guided by either ultrasound or CT imaging whereby a nephroscope is inserted percutaneously into a renal collecting system allowing the stone to be fragmented by lithotripter. Complications include possible sepsis, transurethral resection syndrome, damage to other organs and bleeding following the operation.
Retrograde removal of ureteral and renal stones
Ureteroscopy is most frequently used in the extraction of ureteric calculi. Patients can also have ureteral stenting carried out, which may be desirable if there is the presence of a stricture, a solitary kidney, chronic kidney disease or a large residual stone burden. As stenting can lead to lower urinary tract symptoms and back pain, it should not be carried out in uncomplicated cases. Complications include a 1% risk of ureteral stricture, avulsion or perforation associated with the procedure.
Open or laparoscopic surgery
Formal operative surgery is reported to be necessary in 1–5% of patients, generally in difficult cases. It may be indicated where there is complex stone burden such that other procedures have failed; there is abnormal anatomy or co-morbidities such as morbid obesity. It will usually be the case that laparoscopic approach will be favoured over open.
Special circumstances
Pregnant patients
Renal colic is the most common cause for admission to hospital for non-obstetric causes in pregnant women. It has an incidence of between 0.25 and 0.5% during pregnancy, although rates are not increased in comparison with non-pregnant women. Symptomatic stones will present in the second or third trimester in 80–90% of cases with 70–80% passing spontaneously. Nevertheless, with the possible complications of preterm labour and premature rupture of membranes associated with renal colic, it must still be considered as a potentially serious condition in pregnancy.
Traditionally, management techniques were based around temporizing measures during the course of pregnancy with multiple exchanges of nephrostomy tube or ureteric stent; however, ureteroscopic extraction is being increasingly recognized as a safe definitive treatment. ESWL is generally avoided due to the theoretical risk of damage to the foetus.
Paediatric patients
Only 1% of cases of renal colic will be in children below the age of 18 years. However, those diagnosed with calculi are at high risk of recurrent stones in the future. Spontaneous passage of stones is more common in children than adults; however, there is no evidence for the use of alpha-blockers. Where active intervention is required either ESWL or ureteroscopy can be used safely and effectively.
Secondary prevention of stone recurrence
Any patient who has had a single episode of renal colic is at increased risk of recurrence in the future; therefore, education on potential dietary changes is essential in the long term. All patients should be advised to stay well hydrated as it has been shown that there is an inverse relationship between fluid intake and stone formation. It has been suggested that aiming for a urine output of at least 2 l/day is an effective target for patients.
All patients should have a balanced varied diet; a diet high in vegetables being particularly desirable as it tends to alkalinize the urine. Unfortunately, some fruits and vegetables are high in oxalate and should only be consumed in a limited fashion—these foods include rhubarb, spinach, cocoa, tea leaves and nuts.
Excessive consumption of meat may lead to undesirable metabolic changes and acidification of urine and it is therefore recommended that patients avoid eating more than 1 g/kg bodyweight of protein. Sodium intake should also be controlled as it will lead to increased levels of calcium in the urine and also formation of sodium urate crystals. Borghi et al. have demonstrated that a diet low in sodium and animal proteins will lead to 50% reduction in stone formation in patients with calcium stones.
Due to calcium's role in binding oxalate and preventing its precipitation, patients should not be encouraged to restrict intake of calcium. However, only those with confirmed hyperoxaluria should be started on calcium supplements as excessive intake will lead to calcium stone formation. In patients with confirmed uric acid stone disease, the intake of uric acid should not exceed 500 mg/day. Foods rich in urate include liver, kidneys, poultry skin, herring, sardines and anchovies.
Pharmacological treatments
Any pharmacological treatment should only be considered after a patient has received good advice on fluid intake and potential dietary changes as it is these changes that are more likely to be of benefit to patients rather than any form of medication. Continued compliance with dietary and drinking recommendations must also always be encouraged.
Thiazide diuretics (such a bendroflumethiazide and hydrochlorothiazide) can be commenced in those with hypercalciuria as they have been shown to decrease urinary levels of calcium; however, their efficacy has not been proven in other settings. Potassium citrate can be used in the treatment of patients with hypocitraturia; it is also recommended for patients shown to have renal tubular acidosis and at risk of enteric hyperoxaluria (for example, following bowel resection) Allopurinol has been shown to be of benefit only in patients with hyperuricosuric calcium oxalate stones
Key points
Where immediate admission to hospital is avoided, patients should always have an appropriate referral for further opinion and investigation in a secondary care centre All patients with a potentially infected and obstructed urinary tract must be immediately admitted to hospital Other dangerous differential diagnoses must always be considered in the assessment of a patient with renal colic At first presentation, all patients should have appropriate baseline investigations undertaken, including the chemical analysis of a stone on at least one occasion Long-term patient education on the secondary prevention of stones is vital in the community
Footnotes
*
Ureteric obstruction can also be caused by blood clots, strictures, papillary necrosis, urothelial tumours or pelvi-ureteric junction obstructing bands.