
Abstract
Rheumatoid arthritis (RA) is a destructive polyarthropathy characterized by synovial inflammation. It is often a debilitating illness with significant and irreversible joint damage occurring within the first few years, and around 40% of RA patients are registered disabled within 3 years. Recent developments in treatment, in particular with early use of disease-modifying antirheumatic drugs (DMARDs), have dramatically improved prognosis. This article overviews the presentation and subsequent management of RA in primary care.
The GP curriculum and rheumatoid arthritis
Describe the epidemiology of musculoskeletal disorders at all ages and apply this when developing a differential diagnosis
Explain the aetiology and natural history of common and important musculoskeletal conditions
Distinguish inflammatory from non-inflammatory joint conditions
Describe when blood tests and imaging methods are required for diagnosis, how to interpret them and how they influence management
Describe the indications for referral within a suitable time frame to the most appropriate health care practitioner [e.g. GP with special interest (GPwSI), physiotherapist, podiatrist, osteopath, chiropractor, orthopaedic surgeon or rheumatologist]
Epidemiology
Prevalence of RA varies between ethnic groups and is lowest among people of black African and Chinese descent. In the UK, around 12 000 new cases of RA are reported every year; prevalence of RA is 1.0%. RA is three times more common in women than men and usually presents between the fourth and sixth decades of life. It is more common among people who have another autoimmune disease and smokers.
People are often concerned when members of their family are diagnosed with RA that they too will be at risk. The inheritance of this condition is not straightforward but having a family member diagnosed does seem to increase the risk of developing RA. Estimates for the degree of risk vary widely, but most studies suggest that first-degree relatives have between a two to four times increased risk of developing RA compared with the general population.
Causes and pathophysiology
Twin studies show that 4% of dizygotic twins are concordant for RA as compared with 15% of monozygotic twins. Although there is a clear genetic component in development of RA, other environmental factors also play a part.
RA seems to have been brought from the ‘New World’ (the Americas) to the ‘Old World’ (Europe) sometime after 1800. There is no evidence of its existence in Europe prior to that time either in contemporary art and literature or in skeletal remains. Because of this, the idea of an infective agent brought from the New World to the Old that caused RA became popular.
RA often starts within a few weeks of an acute viral infection or even sometimes following immunization. However, despite extensive research, no single infective organism that triggers RA has been isolated. Therefore, it has been postulated that RA may be an abnormal immune reaction to an infection in a genetically susceptible individual.
RA is an autoimmune inflammatory arthritis with marked inflammation of the synovial membrane. Lymphocytes, macrophages and CD4+ T cells infiltrate the synovium and play a central role in the disease process. Stimulated B cells produce immunoglobulins, including rheumatoid factor (RF), and macrophages produce inflammatory cytokines.
These cytokines and immunoglobulins lead to the destruction of the joint. Of particular importance in this inflammatory cascade is tumour necrosis factor alpha (TNF-α), a pro-inflammatory cytokine which is targeted by some of the newer disease-modifying agents.
Clinical features
The main clinical features pointing to a diagnosis of RA include:
Joint swelling: predominantly affecting proximal metacarpophalangeal (MCP) and interphalangeal joints as well as the wrists and metatarsophalangeal (MTP) joints. Figure 1 shows late changes affecting the hands
Morning stiffness: typically lasting more than 30 minutes
Extra-articular features: fever, malaise, weight loss and fatigue

Deformities of hands associated with RA. Reproduced from Davidson's Principles and Practice of Medicine, Colledge N, Walker B, Ralston S. Copyright Elsevier (2010).
Synovitis is the prominent feature in RA, characterized by joint warmth, stiffness, effusion and pain on stressing of the joint.
Unfortunately, these features, although pointing to an inflammatory arthropathy, are not specific to RA and can also occur in osteoarthritis (OA). OA is far more common than RA. The pattern of joint involvement and the evolution of symptoms over time can often be more helpful.
Most cases of RA initially present with small joint disease of the hands and feet. Occasionally, presentation is with a monoarthritis or with mainly systemic features, such as fever and malaise. However, whatever the initial presentation inflammation tends to spread leading to a polyarthritis (i.e. disease affecting more than four joints).
Extra-articular features
Extra-articular features usually present after joint features and include:
Nodules: firm non-tender nodules over the elbow, forearm and MCP joints
Dry eyes and dry mouth
Pleurisy and pericarditis
Interstitial lung disease
Differential diagnosis
Table 1 lists the major features of commonly encountered conditions presenting with polyarthralgia including RA. Seronegative arthritis is a varied group of disorders incorporating anklyosing spondylitis, reactive arthritis, psoriatic arthritis and arthritis related to inflammatory bowel disease. Of these, ankylosing spondylitis is markedly different in its presentation, mainly affecting the axial skeleton and presenting with insidious low back pain and stiffness. Reactive arthritis (including Reiter's syndrome) is linked to genitourinary infection, in particular Chlamydia infection.
Features of common causes of polyarthritis
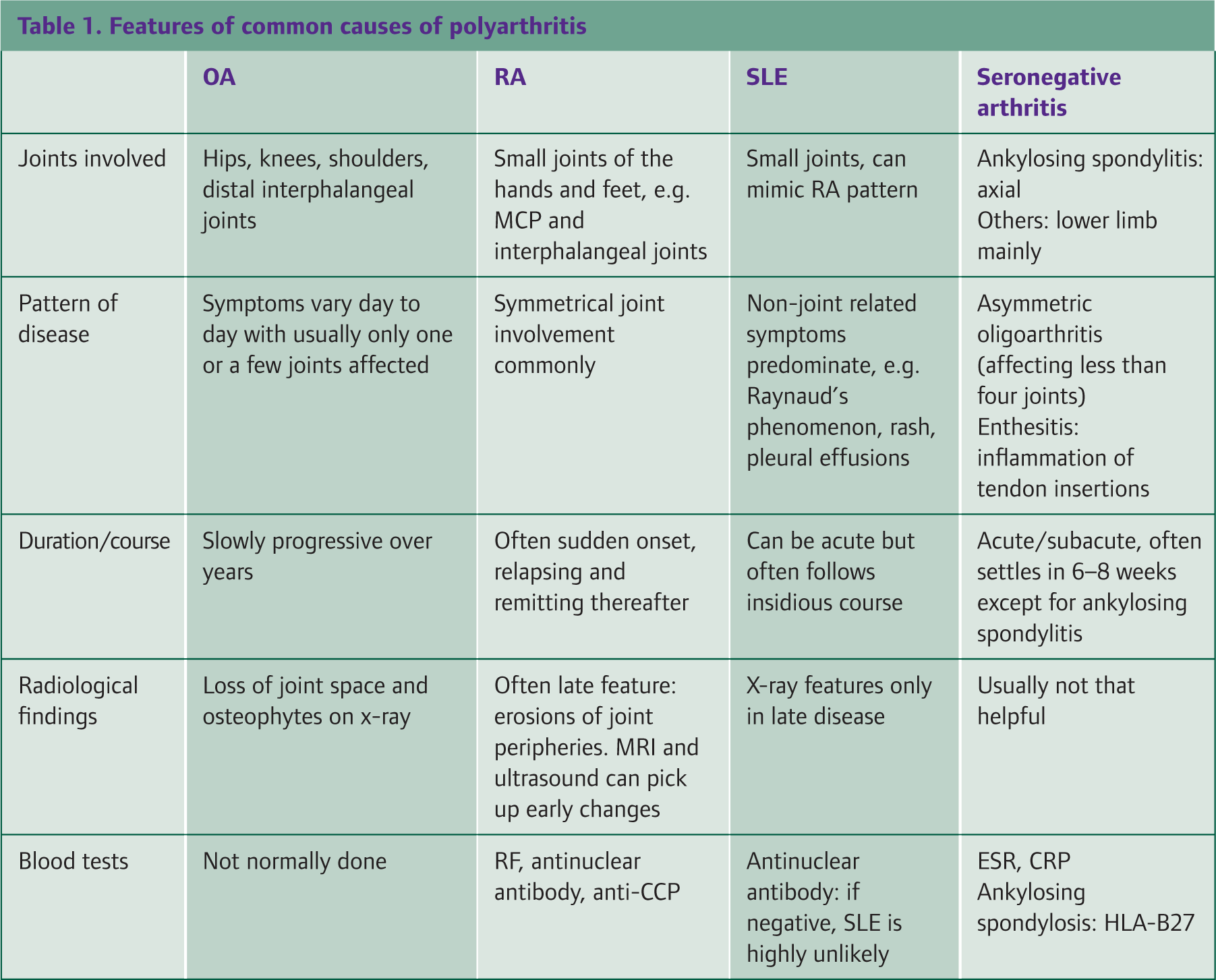
Gout is also important to consider in any differential diagnosis. It is due to deposition of monosodium urate crystals in joints and usually produces an acutely inflamed and very painful joint. The first MTP joint of the great toe is most commonly affected. Subsequent attacks usually only affect one joint at a time but can present as a polyarthritis. Gout is much more common in males and subsides in 10–14 days in most cases.
Laboratory investigations
RA remains a largely clinical diagnosis. Although laboratory investigations are useful in helping to formulate a more complete clinical picture, they are unreliable when used alone. Recent guidance from the National Institute for Health and Clinical Excellence (NICE, 2010) stresses that all investigations including blood markers can be normal in the early stages of the disease.
Inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are useful to include in initial investigations. However, they are non-specific and simply indicate the presence of an inflammatory process.
RF is positive in many patients with established RA and indicates a poorer prognosis. However, RF is negative in many patients with early RA. It is also not specific for RA, and may be positive in a small proportion of healthy individuals, and patients with tuberculosis, systemic lupus erythematosus (SLE) or hepatitis C. Therefore, a negative RF in patients with persistent synovitis does not exclude RA and should not delay onward referral to secondary care.
Newer tests such as anti-cyclic citrullinated peptide antibody (anti-CCP) have greater specificity for RA than RF while having a similar sensitivity. However, these tests are not directly accessible for GPs in many areas.
Radiological investigations
X-rays are often normal early on in RA. Ultrasound is becoming increasingly popular with rheumatologists. It often picks up early synovitis and joint inflammation and is relatively cheap and easily accessible.
When to refer?
For GPs, when to refer is a crucial question. Treatment with DMARDs is initiated in secondary care and reduces the risk of long-term permanent joint damage as well as reducing the high cardiovascular risk associated with RA. The first 12 weeks after initial onset of symptoms are thought to be particularly important and treatment with DMARDs during this period may well be more effective in prevention of long-term joint deformity and disability.
Current guidance (NICE, 2010; SIGN, 2011) suggests urgent referral to rheumatology for patients with any of the following features:
Persistent swelling (6–8 weeks) in more than one joint
Involvement of the MCP or MTP joints
Early morning stiffness lasting more than 30 minutes
‘Persistent swelling’ is defined as lasting between 6 and 8 weeks as other causes of polyarthritis, such as reactive arthritis and arthritis associated with inflammatory bowel disease, usually subside within this time, whereas RA does not.
While awaiting a specialist opinion, symptom control with non-steroidal anti-inflammatory drugs (NSAIDs) and other agents will be necessary. If pain is severe, an intramuscular injection of steroid or course of oral steroids may relieve symptoms but seek advice from the specialist to whom the patient has been referred before administering steroids as steroids alter the clinical picture.
Treatment
Treatment falls into two broad categories: symptom control and DMARDs.
NSAIDs and simple analgesia
The most commonly used drugs for symptom control are regular paracetamol and the NSAIDs. There is not much evidence to suggest any difference between the NSAIDs in effectiveness. Start with the least gastric toxic, for example ibuprofen 200–400 mg three times daily. Given the risk of upper gastrointestinal complications, it is always wise to consider adding a proton pump inhibitor such as omeprazole to any course of NSAID treatment. If the patient is already taking aspirin for cardiovascular prophylaxis, other agents for pain relief and symptom control should be considered, but NSAIDs are not absolutely contraindicated.
Corticosteroids
Oral or intramuscular steroids are used in conjunction with DMARDS to provide quicker resolution of symptoms when treatment is started for the first time. Intra-articular injections of steroids can settle localized flares (for example of the knee or shoulder) and can be used up to three times a year in any particular joint. Depot intramuscular injections or intravenous infusions (pulses) can also help settle an acute flare but offer short-term benefits with the risk of systemic side effects. Daily low-dose oral steroids help symptoms and there is some evidence that they can modify disease progression but concerns about adverse side effects have limited use.
Disease-modifying antirheumatic drugs
DMARDs fall into two broad categories:
Traditional agents—most commonly methotrexate but also sulfasalazine and hydroxychloroquinine
Newer biological agents, e.g. infliximab (antibody against TNF-α), tocilizumab (antibody against interleukin-6) and rituximab (antibody against B cells)
DMARDs should be used only under consultant supervision. They reduce disease progression by modifying the immune response and inflammation and may be used individually or in combination. DMARDs are now started very early in the disease process (within the first 3–6 months), hence the need for early referral. DMARDs can take several months to show any effect.
NICE (2009) and SIGN (2011) recommend initial treatment with methotrexate or sulfasalazine as there is greatest evidence for safety and efficacy with these agents. Newer biological agents are reserved for unresponsive cases and incomplete resolution of symptoms. There is emerging evidence that the most effective option for achieving resolution of symptoms during a first presentation is a combination of methotrexate with TNF-α; however, at present, cost is prohibitive.
Traditional agents must always be started in secondary care but ongoing prescription and monitoring may be done by GP practices under local shared-care arrangements. Before starting traditional DMARDs, patients should have baseline renal and liver function, full blood count (FBC) and urinalysis checked. Monitoring frequency is consultant led, but for methotrexate, blood and urine, tests are weekly until the disease and dose are stable and then monthly for at least the first year. After that time, frequency of monitoring may be reduced under consultant direction. All patients on methotrexate should have a chest x-ray within a year of starting the drug, and those with pre-existing lung disease should have baseline lung function tests prior to initiation. Patients should be asked to report symptoms or signs of infection (when a FBC should be checked) or respiratory symptoms.
Results requiring action include:
Total white cell count of less than 3.5 × 109/l
Neutrophil count of less than 2 × 109/l
Platelet count of less than 150 × 109/l
Alanine transaminase/aspartate aminotransferase (ALT/AST) increased to greater than twice the baseline level
Persistent proteinuria (more than 1+ on two occasions) or haematuria
If any of these abnormalities are detected, discuss the result with the patient's rheumatologist. In addition, if mean cell volume of red cells is greater than 105 fl, check serum B12 and folate levels.
The biological agents also carry potentially serious complications. They have been linked with an increased risk of cancer, infection, reactivation of dormant tuberculosis, congestive heart failure and multiple sclerosis. These agents have been in widespread use for less than 10 years and hence their long-term health implications are still being evaluated. They are usually prescribed and monitored in secondary care.
Physical therapies
Aside from drug therapy, other approaches to maintaining joint function remain very important. Physiotherapy can be beneficial not only in maintaining joint function but also helping to alleviate symptoms.
Surgery
Surgery aims to relieve pain and improve function. Consideration of the risks, benefits and the most appropriate timing of surgery are vital. Common procedures include joint fusion, replacement and excision; tendon transfer and repair and nerve decompression.
The role of the GP
Work
RA can be a debilitating illness resulting in long-term disability that may affect ability to work. GPs have a role in sickness certification. This includes making recommendations, using the new style Med3 certificate, about adaptations to work that might enable the patient to remain at work. The Equality Act (2010) provides protection for those with RA, whether they are in employment when the disease strikes or looking for work. It places the onus on employers to make reasonable adjustments such that the affected individual can continue to carry out their duties in the workplace. The Equality Act also covers discrimination during the initial hiring of staff.
Financial assistance
Patients with disability resulting from RA who would benefit from help with everyday activities may be eligible for Disability Living Allowance (if under the age of 65 years) or Attendance Allowance (if 65 years or older). These benefits are not means tested. Application forms can be downloaded from the government website www.direct.gov.uk/disability.
Patients with RA unable to work may be eligible, after assessment, for Employment Support Allowance. In addition, patients may be eligible for low income benefits.
Support around the home
Both occupational therapy and social services have important roles to play in providing support and assistance at home when joint deformity and disability restrict activities.
Mobility
The Blue Badge Scheme can also be a useful aid for patients struggling with transport when out of the home. It is administered by local councils. In addition, patients who have difficulty driving because of their disability may seek assessment for adaptations to their vehicles via local mobility assessment centres. Financial assistance for adapted cars may be available via the Motability Scheme.
Information and support
Valuable advice and support can be obtained from Arthritis Research UK, whose website (www.arthritisresearchuk.org) not only contains downloadable advice sheets for patients and their families but also provides details of events around the country where affected patients can meet and share experiences. The National Rheumatoid Arthritis Society (www.nras.org.uk; telephone: 0800 298 7650) also provides information and support for patients.
Monitoring for complications
Even when a patient is being monitored by a specialist unit, the GP still has an essential role in checking for complications. Patients with RA are prone to:
Physical disability
Side effects of treatment
Depression—consider routine depression screening at least annually
Osteoporosis—resulting from steroid use, immobility and the RA disease process itself
Increased infections
Lymphoma
Cardiovascular disease (CVD)—patients with RA are at increased risk of CVD due to an accelerated rate of atherosclerosis; although DMARDs reduce this risk, GPs have a vital role in reducing other risk factors.
Amyloidosis (up to 10%)
Conclusions
RA is a multisystem autoimmune disease that tends to present with persistent synovitis and polyarthropathy. Early recognition in primary care and specialist referral for definitive diagnosis are important as early treatment with DMARDs reduces the likelihood of long-term disability and also decreases cardiovascular risk. Specialist treatment focuses on symptom relief and disease modification. Primary care management focuses on supporting the family through signposting to sources of information and support and monitoring for side effects of treatment and complications.
Key points
RA affects 1% of the UK population
RA is a multisystem autoimmune disease probably caused by an environmental trigger acting in a genetically susceptible individual
Early diagnosis and referral to secondary care for treatment with DMARDs are essential to reduce disability and cardiovascular risk
Secondary care treatment involves measures for symptom control coupled with drug treatment to modify disease progression
DMARDs should not be initiated in primary care but may be prescribed on an ongoing basis and monitored in primary care under local shared-care arrangements
GP management involves provision of information and support for the whole family, as well as monitoring for disease complications
Footnotes
Acknowledgements
We would like to thank Dr Shane O'Hanlon for his help with the writing of this article under the InnovAiT ‘buddy’ scheme.