
Abstract
Hcyperhidrosis is a condition in which individuals suffer from excessive and uncontrollable sweating. While its prevalence within the UK is unknown, it is a relatively common dermatological complaint encountered by GPs. It can cause a great deal of embarrassment for many sufferers as well as interference with daily activities. A holistic approach is therefore essential in the assessment and management of this condition. Clinicians should be aware of the treatment options available in both primary and secondary care.
The GP curriculum and hyperhidrosis
Manage primary contact with patients who have a skin problem Be aware of the treatments commonly used in primary care and how to apply them Appreciate the importance of the social and psychological impact of skin problems on the patient's quality of life Ensure that skin problems are not dismissed as trivial or unimportant
The physiology of perspiration
There are three glands responsible for the production of sweat.
Eccrine glands form the vast majority of sweat glands in the human body and are found in large numbers on the forehead, palms, soles of the feet and axillae Apocrine glands are found mainly within axillae and urogenital areas Appoeccrine glands are found within axillae and perianally
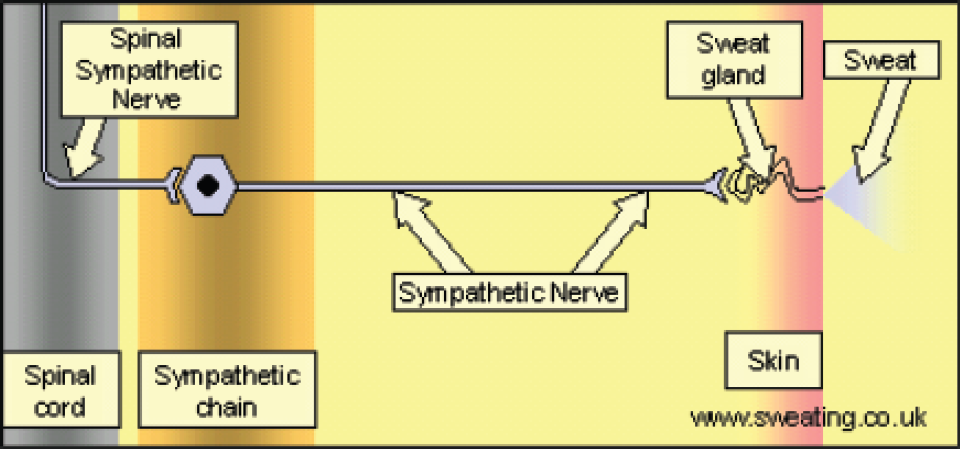
Both eccrine and apocrine glands are innervated by postganglionic fibres from the thoracolumbar sympathetic nervous system (Fig. 1).
Role of the sympathetic nervous system in perspiration
Sweating can occur as part of a thermoregulatory response. If there is a rise in the core or surface body temperature, the thermoregulatory centres within the anterior hypothalamus send signals to eccrine glands via the sympathetic nervous system. This triggers sweat production and its evaporation promotes cooling. The evaporation of 1 g of water is thought to use 2.4 kJ of heat.
Sweating may also occur as a result of emotion, such as anxiety or fear. Here, it is thought that centres of higher functioning within the cerebral cortex act on hypothalamic regulatory centres to induce sweating in a manner similar to that described above. The palms and axillae are primarily affected by emotional sweating.
Gustatory sweating is defined as perspiration that occurs on eating hot or spicy foods. It tends to affect the face, scalp and neck and can be a normal physiological response but may be related to an underlying disease. Pathological causes of gustatory sweating will be mentioned later in the article.
Complications of excessive perspiration
The amount of sweat produced can vary greatly from person to person. Excessive perspiration only becomes an ailment if it begins to have a negative impact on an individual's quality of life. Common effects may include:
damp clothing that requires regular changing damaged garments odours irritant dermatitis secondary skin infections (e.g. tinea) and avoidance of social norms that may lead to embarrassment (e.g. shaking hands).
Types of hyperhidrosis
Primary focal hyperhidrosis
Primary focal hyperhidrosis has no identifiable cause. It affects specific areas such as the forehead, palms (Fig. 2), soles of the feet (Fig. 3) or axillae (Fig. 4). It usually presents in childhood or adolescence but can occur at any age. Its diagnosis can be made if sufferers satisfy a set of criteria (Box 1).

Palmar hyperhidrosis.

Plantar hyperhidrosis.

Axillary hyperhidrosis.
Diagnostic criteria for primary focal hyperhidrosis
There is localized sweating that is excessive and visible
There is no underlying cause
Symptoms have been present for at least 6 months
At least one of the following sites are involved: forehead, axillae, palms and soles At least two of the following features are present:
Areas of sweating are bilateral and symmetrical Daily activities are impaired Excessive sweating occurs at least once in a week The onset of symptoms occurred before the age of 25 years There is a family history of hyperhidrosis There is no focal sweating during sleep
Secondary focal hyperhidrosis
Secondary focal hyperhidrosis affects specific areas of the body and is due to an underlying condition (Box 2). Causes can be broadly categorized into:
neurological disorders (e.g. cerebrovascular disease) thoracic lesions (e.g. mesothelioma) disorders that induce gustatory sweating (e.g. diabetic neuropathy) iatrogenic causes (e.g. sympathetic trunk injury during endoscopic sympathectomy) and other causes (e.g. rheumatoid arthritis)
Generalized hyperhidrosis
Generalized hyperhidrosis affects the entire surface area of the skin. It may be idiopathic or secondary to underlying disease or medication (Box 2). It may also be present in patients who are undergoing normal physiological change such as in menopause or pregnancy.
Assessment in primary care
History
Hyperhidrosis can have a profound effect on a sufferer's self-esteem and ability to engage in social norms. It is, therefore, essential that GPs are both empathic and nondismissive during a consultation. This is particularly important when previous treatments have failed or investigation results have returned as normal. Box 3 lists examples of questions that may be asked in a hyperhidrosis history.
It is important to determine whether or not a patient is suffering from hyperhidrosis, its type and whether further investigation is necessary. This can be verified by enquiring about the age of onset, duration of symptoms, sites affected, whether sweating occurs at night, medications being taken, a family history of hyperhidrosis, features of systemic disease, features of conditions that are known to cause excessive sweating and a menstrual history in female patients. Discussing the complications of excessive sweating, its effect on daily activities and treatments tried so far can help gauge the severity of symptoms and allow the clinician to decide on what treatment options to offer the patient.
Causes of secondary focal and generalized hyperhidrosis
Alcohol abuse and withdrawal Anxiety Cardiovascular disease, e.g. cardiac failure, ischaemic heart disease, shock Disorders that induce gustatory sweating, e.g. periauricular herpes zoster, parotid gland injury, tumour invasion of the cervical sympathetic trunk Drugs, e.g. selective serotonin reuptake inhibitors, tricyclic antidepressants, venlafaxine, trazodone, mirtazapine, pyridostigmine, neostigmine, bethanecol, pilocarpine, propanolol Endocrine conditions, e.g. thyrotoxicosis, phaeochromocytoma, hypoglycaemia, acromegaly and hyperpituitarism Infection, e.g. tuberculosis, HIV, malaria, brucellosis, abscesses Intrathoracic lesions, e.g. mesothelioma, cervical rib Malignancy, e.g. Hodgkin's lymphoma, myeloproliferative disorders, spinal tumours Menopause Neurological conditions, e.g. cerebrovascular disease, diabetic autonomic neuropathy, peripheral neuropathies, spinal cord lesions, Parkinson's disease and diencephalic epilepsy Obesity Pregnancy Respiratory failure Rheumatoid arthritis
Questions to consider in a hyperhidrosis history
How long the sweating has lasted for and at what age it first started? Why the patient feels it is excessive, e.g. regular changing, garment damage? Whether the sweating is localized or generalized and the sites affected? Whether the sweating is symmetrical or unilateral? Whether sweating occurs during sleep? Whether anxiety exacerbates sweating? Whether the patient is on any medications that are known to cause sweating? Family history of hyperhidrosis • Features of systemic disease, e.g. malaise, weight loss, pyrexia Features of conditions that may lead to a secondary focal or generalized hyperhidrosis Female patients should be asked about menstruation, e.g. last period, regularity How sweating has stopped the patient from partaking in activities or adhering to social norms that he or she would want to do, e.g. shaking hands, dating, attending the gym? Treatments the patient may have tried so far, e.g. antiperspirant sprays or roll-ons
Examination
Unless you are convinced the patient meets all the criteria for primary focal hyperhidrosis, a thorough physical assessment should be performed. This might include cardiovascular, respiratory, neurological and thyroid examinations depending on the history.
Investigations
If a diagnosis of primary focal hyperhidrosis is made, no further investigation is necessary. Diagnostic tests should be considered in patients in whom an underlying cause is suspected. A good history and examination will help a GP to decide what blood tests or imaging to request, especially if other features of a condition are present. For example, a chest x-ray may be helpful in excluding a mesothelioma or cervical rib. Thyroid function tests may be performed in suspected thyrotoxicosis. A fasting glucose can help confirm an underlying diabetic neuropathy. A full blood count can be useful to look for infective causes, Hodgkin's lymphoma and myeloproliferative disease.
Management of generalized or secondary focal hyperhidrosis
The management of generalized or secondary focal hyperhidrosis involves investigating and treating the underlying cause. This may entail specialist referral, especially if there are other features present that are indicative of a serious underlying pathology.
Some patients with generalized hyperhidrosis will have no identifiable cause. For this unique group, the International Hyperhidrosis Society has suggested treating the worst affected areas as one would for primary focal hyperhidrosis.
An alternative would be to consider a trial of systemic agents. These medications include anticholinergics (e.g. glycopyrronium), clonidine, diltiazem or a short course of benzodiazepines. There is little published data, however, that demonstrates the efficacy of these treatments in this particular situation. It may, therefore, be sensible to consider seeking an opinion from a dermatologist before commencing these drugs in primary care.
Management of primary focal hyperhidrosis
Lifestyle advice
General measures include avoiding drinks that contain caffeine, avoiding spicy foods, wearing loose-fitting garments that do not show stains readily (such as black and white), avoiding fabrics that are man made (e.g. nylon) and using soap substitutes during bathing as well as talcum powder afterwards. Patients who suffer primarily fromaxillary hyperhidrosis should use a commercial antiperspirant frequently and consider using armpit or sweat shields to protect clothing. Those who suffer primarily from plantar hyperhidrosis should consider avoidance of occlusive footwear (e.g. boots), wearing a different pair of shoes on alternate days, changing socks twice daily and using absorbent soles and foot powder.
Aluminium salts
These work by temporarily closing the pores of sweat glands. They should be applied at night because this is the time when sweat glands are inactive so allowing an opportunity for active ingredients to penetrate the skin. In the UK, 20% aluminium chloride hexahydrate is manufactured as either Driclor (a roll-on stick) or Anhydrol Forte (a solution). Both are licensed and can also be purchased over the counter. Both should be applied to the dry skin of affected areas before sleep and washed off the following morning. They should be used every 1–2 days until the condition improves and then as required thereafter. If successful, they can be continued indefinitely. A dusting powder (Zeasorb) can be used as an alternative for plantar hyperhidrosis. The main side effect of aluminium salts is skin irritation which limits their use in some patients.
Cognitive behavioural therapy
For some hyperhidrosis, sufferers anxiety may be an exacerbating factor. These patients may benefit from cognitive behavioural therapy.
Treatment options available in secondary care
Refer to a dermatologist if lifestyle changes or aluminium salts prove to be unsuccessful or unacceptable. If a patient is keen on surgical treatment, refer directly to a vascular surgeon.
Ionotophoresis involves passing a weak current through warm water while an affected area is immersed in it. It is thought to work by disrupting the ion channels that run through secretory glomeruli within sweat glands. Patients will undergo 2–4 sessions/week and some improvement is usually seen after 4–10 sessions. Maintenance treatment is required at 1–4 weekly intervals. Resistant cases many benefit from the addition of glycopyrronium bromide to the water.
Unfortunately, many National Health Services (NHS) centres do not offer ionotophoresis and it can cost around £250 to purchase an ionotophoresis bath for personal use. There is also little evidence demonstrating its efficacy in axillary hyperhidrosis. Response rates of 90–100% have been noted in several observational studies when used in the treatment of plantar hyperhidrosis. A similar response rate has been noted when ionotophoresis has been used for palmar hyperhidrosis.
Botulinum A toxin can be delivered to affected areas by intradermal injections. It is thought to inhibit acetylcholine release near sweat glands and subsequently limit sweat production. It is generally safe, but side effects have been reported and these include compensatory sweating (5–10% of patients), pain at the site of injection and local reactions (9–12% of patients). Most NHS centres do not offer this treatment and privately it can cost £300–£600 per session.
Several large, randomized, placebo controlled trials have demonstrated significant improvement in axillary hyperhidrosis symptoms with Botulinum toxin A administration. Response rates were noted to be between 75 and 95%. Some studies have also demonstrated response rates of 90% in palmar hyperhidrosis sufferers. There is little evidence supporting the use of Botulinum A toxin administration in plantar hyperhidrosis.
Surgery can be considered as a last resort in patients in whom other treatment options have failed. Resection of sweat glands can be performed under local anaesthesic but has a relapse rate of 10–20% and can result in scar formation. Another procedure is endoscopic thoracic sympathectomy. This is the removal of part of the sympathetic trunk endoscopically. It is performed in patients who suffer from severe axillary, palmar and craniofacial hyperhidrosis. Unfortunately, it can be associated with complications that can be just as disabling as the original complaint. These include gustatory sweating (50% of patients), compensatory sweating (almost 100% of patients), phantom sweating, pneumothorax (up to 75% of patients), haemothorax and Horner's syndrome.
Prognosis
A few sufferers spontaneously improve after 25 years of age. In the majority, however, the disease runs a chronic course.
Support groups
There are several support groups available for patients who are interested in learning more about hyperhidrosis and the treatment options available. These are listed in Box 4.
Hyperhidrosis support groups
Key points
Hyperhidrosis is a condition in which individuals suffer from excessive and uncontrollable sweating Sweating may be primary focal, secondary focal or generalized Management of secondary focal or generalized hyperhidrosis involves investigating and treating the underlying cause Treatment options for primary focal hyperhidrosis include lifestyle changes, aluminium salt application, ionothophoresis, botulinum toxin injection and surgery