
Abstract
The term chalazion, from the Greek meaning ‘hailstone’, refers to a lipogranuloma of the meibomian gland. Chalazia are very common and the majority can be managed conservatively in primary care. This review provides an overview of management for GPs.
The GP curriculum and chalazia
Manage primary contact with patients who have an eye problem Perform an external examination of the eye Apply the information gathered during the history-taking and examination to generate a differential diagnosis and formulate a management plan to include assessment of severity and need for referral to secondary care Manage simultaneously both acute and chronic problems in the patient with eye problems
Anatomy
The meibomian glands are sebaceous glands within the tarsal plates of the eyelids (Fig. 1). The meibomian glands produce a lipid layer that lies on the surface of the tear film. This prevents the middle or aqueous layer of the tear film evaporating. The inner layer of the tear film is made from hydrophobic mucin and is produced by globlet cells in the conjunctiva.
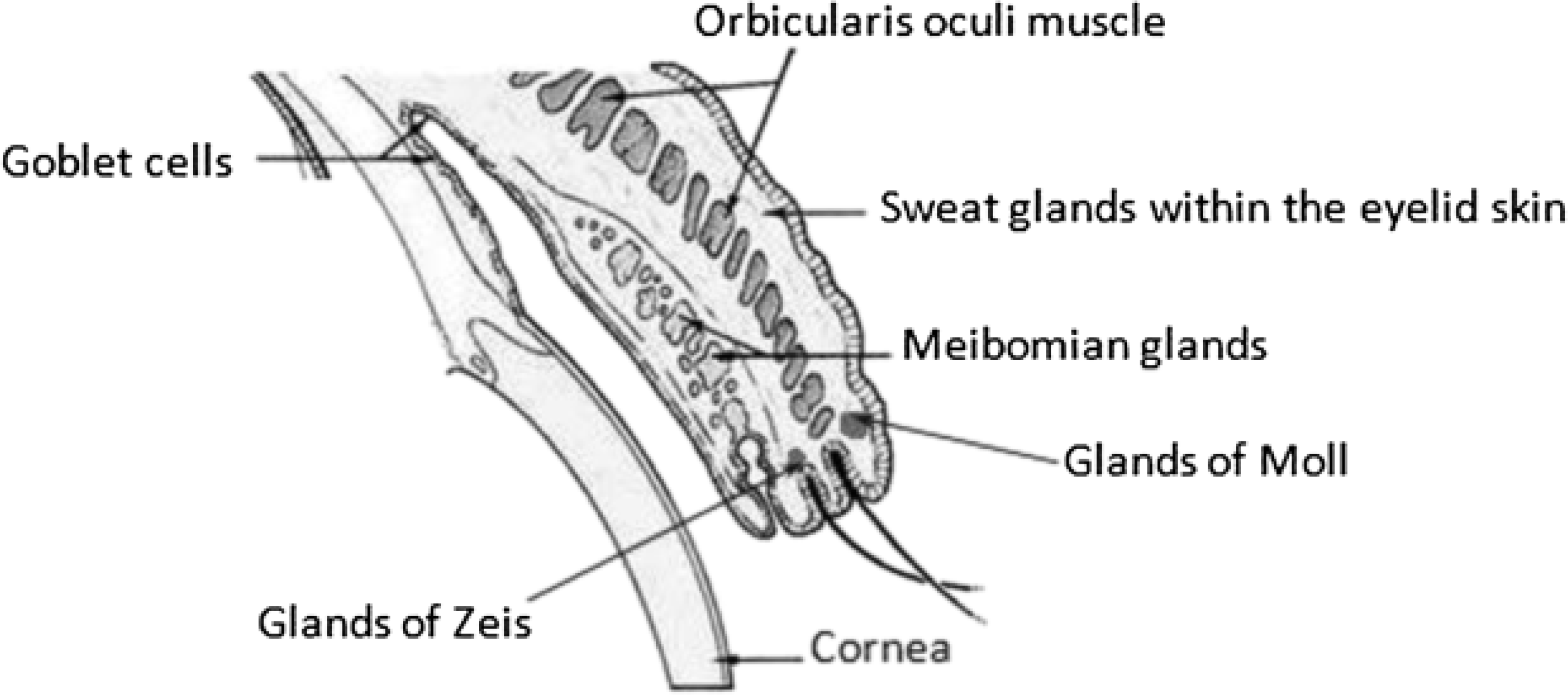
Anatomy of the eyelids.
Aetiology
A chalazion forms following retention of sebaceous secretions in the secretory gland; these become inflamed and infected leading to blepharitis (eyelid inflammation). They can then become blocked, leading to a leakage of lipids into surrounding tissue, inciting a granulomatous reaction and finally resulting in the clinically apparent nodule (Fig. 2).

Secondary infection of a chalazion affecting a meibomian gland by bacteria (usually Stapyhlococcus aureus) can result in a pustular hordeolum internum or internal stye (Fig. 3). A differential diagnosis is of an external stye, resulting from infection of the lash follicle or adjacent glands (Zeis or Moll).

Hordeolum.
Epidemiology
Chalazia are very common; a recent survey by Gaddiee (2010) carried out in the USA suggested that chalazia affect up to 17.8% of the population.
Predisposing factors
Predisposing factors for the development of chalazion are listed in Box 1. It is not uncommon for patients with tear dysfunction to present with chalazion and for chalazion to result in an unstable tear film (Gaddiee, 2010).
Predisposing factors for developing chalazion.
Chronic blepharitis Dry eye Seborrhoeic dermatitis Acne rosacea Diabetes Pregnancy
Blepharitis is inflammation of the eyelids. Broadly two types exist:
Anterior blepharitis affects the lashes and is visible as hard and brittle scales or ‘collarettes’ (dandruff-like flakes) in the eyelashes. Causes include staphylococcal disease (usually in younger age groups) and seborrhoeic dermatitis in older patients. Posterior blepharitis affects the meibomian glands directly. The duct orifice of the glands becomes hyperkeratinized and blocked. Meibomian gland dysfunction can be demonstrated in posterior blepharitis by squeezing the eyelids. A stringy toothpaste like secretion suggests meibomian dysfunction. Stagnation of meibomian secretions may result in infection.
Infestation of the eyelash follicles by the hair follicle mite Dermodex folliculorum can also result in blepharitis. This is suggested by crusting at the base of the eyelashes.
Seborrhoiec dermatitis displays characteristic skin changes of oily skin, flaking of the scalp, brows, nasolabial folds and behind the ears. It is associated with blepharitis and thus also chalazion formation.
Acne rosacea is associated with posterior blepharitis. It is characterized by facial flushing, telangiectasia, erythema and a papulopustular eruption resembling acne. Blepharitis and chalazion in patients with rosacea may also be associated with D. folliculorum infestation.
Presentation
Chalazia usually affect the upper eyelids, which contain more meibomian glands. Presentation varies and may include a history of recent eyelid discomfort, followed by eyelid inflammation and a visible lump (usually round or oval) on the lid (Fig. 2). On inspection, a lesion is usually visible (although it is sometimes only palpable) in the eyelid.
Patients may also present with visual symptoms when chalazia are large enough to depress the cornea and induce astigmatism. Similarly, visual field defects may result following mechanical ptosis of the upper eyelid.
The differential diagnosis includes other causes of eyelid swellings including lid tumours such as basal cell carcinoma and squamous cell carcinoma. A lateral upper lid lesion displacing the eye medially might suggest a lacrimal gland tumour. Features which should raise suspicion of a sinister cause when faced with blepharitis and chalazia are unilateral blepharitis, loss of eyelashes, chronic resistant blepharitis and recurrent chalazion. If a skin tumour or sinister cause of blepharitis and chalazion is suspected, specialist referral should be made.
Management
Non-surgical management of chalazia is often effective and easily carried out in primary care (Gilchrist and Lee, 2009). Figure 4 summarizes a stepwise approach to management.
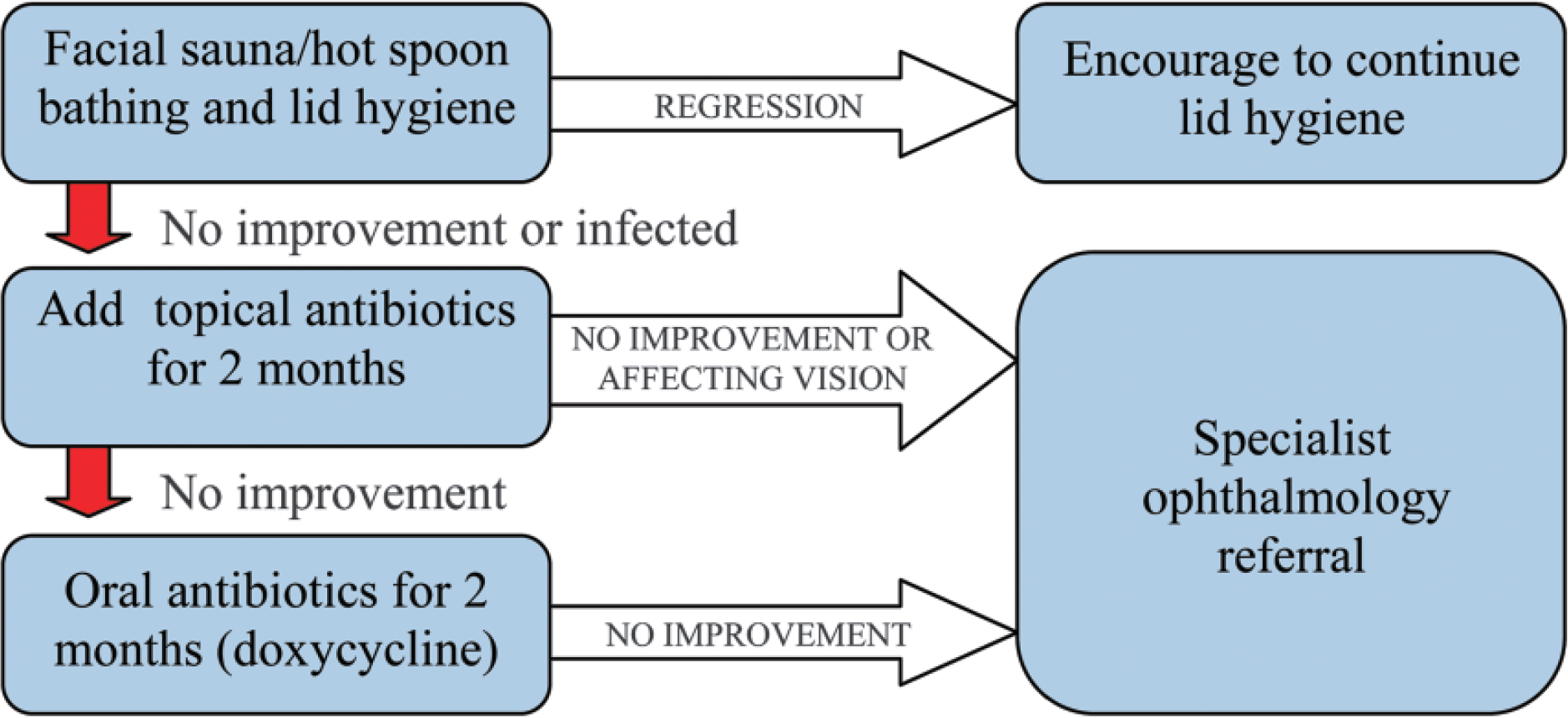
Suggested flow diagram when managing chalazion.
It is thought that up to 80% of patients can achieve complete resolution of chalazion with conservative management (Perry and Serniuk, 1980). An internal audit carried out in our own specialist eye department found that on average, the time between referral of a patient with a diagnosis of chalazion, and review in the clinic was 4 months. All the patients referred by GPs were correctly diagnosed prior to referral. Of the 35 cases reviewed, 26% had been treated in the community prior to referral with antibiotics alone; 20% were encouraged to use hot bathing and lid hygiene. The symptoms and signs of 100% of the patients using hot spoon bathing and lid hygiene resolved spontaneously without additional specialist intervention.
Lid hygiene
Key to the treatment of chalazia is good lid hygiene. The underlying blepharitis must be treated. A facial sauna is probably the most effective way of heating the lids; this should be applied for around 15 minutes, until the face is red and all the skin and lid pores are open. An alternative is ‘hot spoon bathing’ in which a flannel or gauze wrapped around a spoon is dipped in boiling hot water and then held about 10 cm from the face below the eye without touching the skin. The steam rises towards the eye bathing it.
Pressure can then be applied to the edge of the lid or around the chalazion; this helps the glands to release their secretion, which often harbours low grade infection. The lids are then pressed using cotton buds and cleaned with a non-stinging (baby) shampoo, ideally using tea tree oil as a natural antiseptic. It is important to clean well into the base of the lashes removing any crusting that has formed there.
Once the lids are clean, the detergent can be removed with pieces of moist cotton wool wiped across first the upper and then the lower lids. Thorough cleansing only needs to be done twice a week. Blepharitis also responds well to topical antibiotics such as chloramphenicol ointment nocte to the lids and chloramphenicol drops three times during the day; these may need to be prescribed for 2–3 months.
If resolution does not occur, consider oral doxycycline 100 mg daily for 2 months. Other oral tetracyclines are an alternative. Tetracyclines should not be prescribed in pregnancy, to women breastfeeding or to young children.
Specialist options
If a chalazion is not settling, despite primary care management, or is obstructing vision, consider referral for specialist review.
Specialist options include:
Topical steroids, e.g. guttate Lotemax or fluoromethalone (FML) twice daily Surgical incision and curettage
Patients referred to a specialist eye department for further management should be instructed to contact the referral centre to cancel an appointment in advance if they experience involution of their chalazion, to avoid unnecessary waste of outpatient appointments and/or theatre slots due to patients who do not come to their appointment because of resolution or the absence of clinically apparent chalazion at assessment.
Key points
Conservative management of chalazion can be carried out in primary care It is crucial to identify and manage systemic/dermatological conditions A conservative approach with lid heating and lid hygiene is successful in the majority of cases Topical antibiotics alone may not resolve chalazion Features which should raise suspicion of a sinister cause when faced with blepharitis and chalazion are unilateral blepharitis, loss of eyelashes, chronic resistant blepharitis and recurrent chalazion Refer cases with a suspected sinister cause, those cases in which a chalazion is affecting vision and unresolved chalazion for specialist review; instruct patients with chalazion that resolution is possible and they should cancel eye clinic appointments if that occurs
Footnotes
Acknowledgements
We would like to say a special thank you to Mr Richard Newsom, Consultant Ophthalmologist, Southampton University Hospitals Trust for his help reviewing and revising this article.