
Abstract
Atransient ischaemic attack (TIA) is defined as an acute neurological event causing loss of focal cerebral or ocular function lasting less than 24 hours and thought to be due to inadequate cerebral or ocular blood supply. More than 46 000 people suffer a TIA in the UK each year. Of these, approximately 10% will go on to suffer a stroke within the next 5 days and 20% within the next 4 weeks. The importance of this diagnosis both to the individual and to the National Health Service (NHS) is therefore huge. This article will discuss the diagnosis and management of TIA in general practice including primary and secondary preventative strategies.
The GP curriculum and transient ischaemic attacks.
Manage primary contact with patients who have a cardiovascular problem Coordinate care with other primary care health professionals, cardiologists and other appropriate specialists, leading to effective and appropriate acute and chronic disease management Make timely appropriate referrals on behalf of patients to specialist services including TIA clinics Promote cardiovascular well-being by applying health promotion and disease prevention strategies appropriately Demonstrate a reasoned approach to the diagnosis of cardiovascular symptoms using history, examination, incremental investigations and referral Advise patients appropriately regarding driving according to the Driver and Vehicle Licensing Agency (DVLA) guidelines Describe and be able to implement the key national guidelines that influence health care provision for cardiovascular problems
Background
Early identification, assessment, investigation and treatment of TIA is vital to reduce risk of recurrent stroke. Up to 23% of strokes are preceded by a TIA and the risk of stroke in the week after TIA is up to 10% (Coull et al., 2004; Rothwell and Warlow, 2005). Stroke costs the NHS £7 billion/year (National Stroke Strategy, 2007) through a combination of direct costs, informal care costs and income lost. Therefore, aggressive management of TIA in order to prevent recurrent stroke not only benefits patients but also the economy as a whole.
It is therefore important that as GPs we are alert to the diagnosis of TIA and know how to risk stratify patients to guide appropriate referral in addition to understanding ongoing management strategies. The importance of the topic as a whole has been recognized nationally within the National Stroke Strategy (2007) and also the National Clinical Guideline for Stroke [2008—incorporating the National Institute for Health and Clinical Excellence (NICE) guidance on diagnosis and initial management of acute stroke and TIA]. These documents set out the importance of appropriate urgent referral for suspected TIA. The recommendations in this article are based on these two documents, in addition to the NHS Clinical Knowledge Summary (CKS) on the topic of stroke and TIA (2011) and the recently released NICE Technology Appraisal on antiplatelet medication (2010).
Risk factors and primary prevention
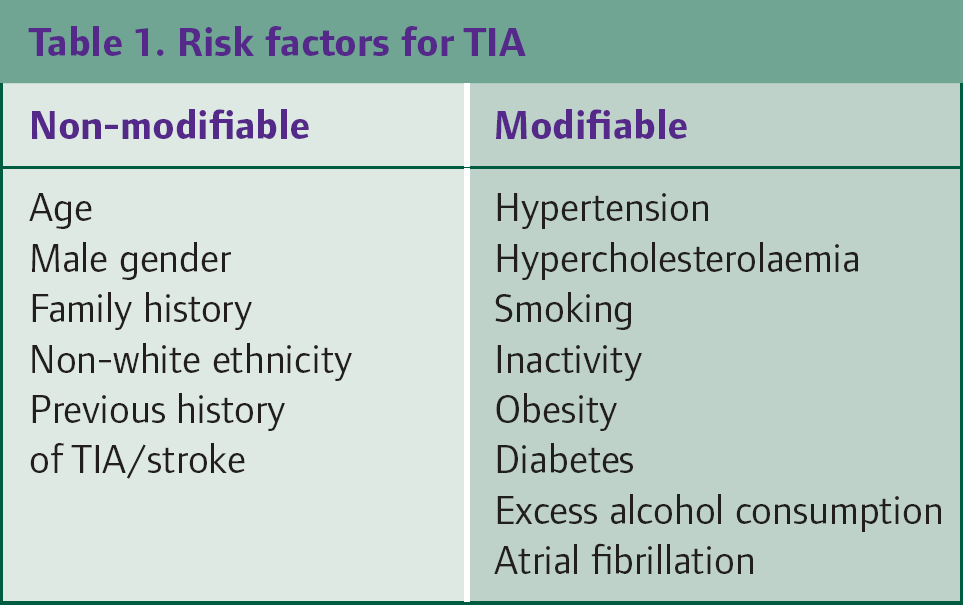
Appropriate management of TIA should begin prior to an event happening by aggressively targeting risk factors. Risk factors for TIA include both non-modifiable and modifiable factors and are shown in Table 1. The majority of factors are common to all cardiovascular disease and hence appropriate and aggressive management of these factors in line with national guidelines can help to reduce the risk of a TIA.
Risk factors for TIA
Diagnosis
Recognition of the symptoms of TIA is vital. This is to facilitate appropriate diagnosis, referral management and the prevention of future strokes. Most TIAs only last several minutes. Therefore, presentation to primary care after the event is common. By definition, however, a diagnosis of TIA can only be made if symptoms have resolved fully within 24 hours. Any patient seen within this time who has ongoing neurological symptoms should be assumed to have a stroke and be referred to hospital immediately.
Diagnosis of TIA can sometimes be difficult because a variety of differentials can exist (see Table 2). A suspected TIA should be diagnosed in any patient with transient focal neurological symptoms that suggest a focal neurological event and are otherwise unexplained (CKS, 2011). Potential symptoms are listed in Box 1. Note that these are usually unilateral and of sudden onset but importantly can also include symptoms such as visual field defects. Up to 50% of suspected TIAs turn out to be due to an alternative cause (such as in Table 2). However, all patients presenting with symptoms suggestive of TIA should be managed as such until review by specialist services to help confirm diagnosis has taken place.
Conditions that may present with symptoms similar to TIA

Possible symptoms of TIA
Facial weakness Unilateral weakness of upper and/or lower limb Unilateral sensory loss of upper and/or lower limb Speech problems Visual defects Disorders of perception Disorders of balance Coordination disorders
Over recent years, there has been a public campaign to educate patients about the importance of stroke and TIA and also to alert patients about the presenting symptoms of these conditions. The FAST tool was designed with this in mind (see Fig. 1). It is a useful out-of-hospital guide to help the general public (as well as paramedics and doctors) detect symptoms, not only of stroke but also of TIA, and encourage them to present to medical services. While the FAST tool is helpful in its simplicity, it will not detect less common symptoms of TIA such as visual field deficit. A negative result using the FAST tool should prompt a more thorough assessment if TIA is suspected.

FAST campaign to aid symptom recognition in members of the public.
Management at first presentation in general practice
Rapid treatment after TIA improves outcome including prevention of subsequent stroke with associated morbidity and mortality. Prior to the 2007 National Stroke Strategy, only 35% of patients were seen in secondary care within 7 days of suspected TIA as many GPs at that time did not refer all patients (Department of Health, 2007). Rapid treatment and referral of patients with possible TIA were therefore a key component of the National Stroke Strategy.
The EXPRESS study (Rothwell et al., 2007) showed that early initiation of antiplatelet, statin and antihypertensive treatment resulted in an 80% relative risk reduction of early recurrent stroke. Aspirin (300 mg daily for the first 2 weeks, then 75 mg daily indefinitely) should be started immediately at first assessment in primary care. Raised blood pressure should not prevent this treatment but gastro-protection should be considered in those at risk of side effects. Patients already taking aspirin should continue their current dose (unless non-compliance is suspected when the dose should be increased to 300 mg). True intolerance or allergy is rare but in these cases, an alternative should be considered. Patients with active gastrointestinal bleeding or a known ulcer should not receive any antiplatelet therapy nor should those who are currently taking warfarin (but these patients should be admitted to exclude haemorrhage).
In addition, all patients should have their risk of early stroke assessed in order to guide the speed at which referral to secondary care is made. There have been several risk assessment tools suggested in the literature; however, the best validated tool recommended by all UK parties is the ABCD2 score where points are given on simple clinical features easily obtained at first assessment (see Table 3).
ABCD2 score (maximum 7 points)

The scoring tool should be applied to patients at presentation with referrals made as following.
Greater than or equal to four points on ABCD2 score—high risk of recurrent stroke. Referral should be made urgently to secondary care for review and investigation within 24 hours Three points or fewer on ABCD2 score—slightly lower risk of recurrent stroke. Referral should still be made urgently to secondary care but for review and investigation within 1 week
The pathways by which these referrals are made vary locally. There are exceptions to these rules as follows:
Recurrent TIA-like symptoms within a week (irrespective of ABCD2 score)—assumed to be at high risk of recurrent stroke. Referral should be made urgently to secondary care for review within 24 hours. Patients with suspected TIA taking warfarin—should always be admitted for brain imaging to exclude haemorrhage Patients in atrial fibrillation (AF)—should be considered for admission as potentially higher risk of stroke Late presenters (i.e. more than a week after symptoms occurred)—should be managed as lower risk. Referral should be made to secondary care with target for review within 1 week
The only time referral is not necessary is if a patient has previously suffered with stroke or TIA and been fully investigated (including carotid artery assessment). In this case, referral can be avoided if the diagnosis is certain, the patient is already on optimal treatment, new AF has been excluded and the TIA does not involve any new vascular territory.
For those patients at lower risk who may not be seen in secondary care for a week, depending on local protocols, consider doing baseline tests in primary care. These are likely to include an electrocardiogram (ECG), a full blood count, renal function tests, a fasting glucose and lipid profile, liver and thyroid function tests.
During the initial consultation in primary care, the referral procedures should be discussed with patients. It is also important to explain what the patient should expect to occur in secondary care and to have an initial discussion of secondary risk prevention. Advise patients not to drive until assessment in secondary care has taken place when definitive advice should be sought. Driving is not permitted for 1 month following TIA for Group 1 (e.g. car) licence holders and for 1 year for Group 2 (e.g. heavy goods vehicle) licence holders (DVLA, 2011).
Management in secondary care
Secondary care assessment aims to confirm the diagnosis of TIA and exclude preventable causes. Brain imaging may be performed (magnetic resonance imaging or computed tomography) if diagnosis is uncertain or to confirm the vascular territory involved. If initial investigations have not been done in primary care, ECG to exclude AF, chest x-ray and a routine blood screen are carried out in secondary care. Echocardiogram may be indicated if the patient has had a recent myocardial infarction or has heart failure or a heart murmur.
Carotid imaging, within 1 week of symptom onset, is arranged for patients with symptoms stemming from the carotid artery territory if the patient would be a candidate for carotid surgery. Carotid imaging is important to detect patients with carotid stenosis who have the highest risk of stroke recurrence. Good evidence from both European and North American randomized control trials has shown that the early operation of severe symptomatic carotid stenosis (greater than 70%) significantly reduces the risk of recurrent stroke (Rothwell et al., 2003). The number needed to treat to prevent one recurrent stroke is five if carotid endarterectomy is performed within 2 weeks but this rises to 125 if performed after 12 weeks (Rothwell et al., 2004). NICE (2008) recommends patients with greater than 70% stenosis (or greater than 50% depending on which measurement criteria are used) should be assessed for endarterectomy within 1 week of symptom onset and undergo surgery within 2 weeks.
Other treatment usually started in secondary care includes:
Antiplatelet medication—ideally aspirin 300 mg daily for 2 weeks and then 75 mg daily thereafter and dipyridamole 200 mg three times daily indefinitely (NICE, 2010) Anticoagulation if AF is diagnosed Blood pressure control Statin treatment—regardless of baseline cholesterol levels aiming to reduce total cholesterol by 25% or to less than 4 mmol/l, whichever is the lower value, and to reduce low-density lipoprotein (LDL) cholesterol by 30% or to less than 2.0 mmol/l, whichever is the lower value Advice on driving, exercise, diet and smoking cessation
Modified-release dipyridamole should be given alone to patients who are allergic to or intolerant of aspirin and aspirin given alone to those who are allergic to or intolerant of dipyridamole. If both of these drugs are not tolerated, or there is allergy, then clopidogrel can be given alone as a final option but this is an off-licence use.
Follow-up and ongoing management in primary care
Following confirmatory diagnosis and management in secondary care, GPs are best placed to ensure appropriate ongoing management of patients who have suffered a TIA. This involves ensuring that medical management and lifestyle changes are optimized, as well as providing ongoing support to patients. A summary of optimal management is shown in Box 2.
The National Stroke Strategy (2007) recommends that patients are reviewed 1 month following a TIA to ensure that all interventions (including appropriate medication and risk factor reduction) are correctly in place. It is also recommends that patients are reviewed at least annually in primary care to ensure that they are taking the correct medication and that their risk factors are being appropriately managed including the annual recording of blood pressure and lipid profile. Patients who have suffered a TIA are also eligible for annual influenza vaccination and this should be actively encouraged. Quality and Outcomes Framework points are available to practices for annual review of patients who have suffered a TIA (BMA/NHS Employers, 2011). Patients should also be provided with contact details of organizations such as The Stroke Association (www.stroke.org.uk) to access further information and support.
Summary of ongoing management post-TIA.
Five portions of fruit and vegetables per day Two portions of oily fish per week Replace saturated fats with polyunsaturated or monounsaturated fats Reduce amount of salt intake Overweight patients should be offered help and support to lower their body mass index
Key points
TIA is an important clinical condition as it is associated with a 10% risk of subsequent stroke in the following week Patients should be risk assessed on presentation in primary care in order to guide the urgency of assessment in secondary care Most patients should be started on aspirin in primary care prior to referral Patients with Group 1 licences should be advised not to drive for 1 month following TIA Following secondary care review, most patients should take aspirin and dipyridamole indefinitely and be regularly reviewed (at least annually) for risk factor modification
Footnotes
Acknowledgements
Many thanks to Arvind Chandratheva for his helpful suggestions regarding an early draft of this article.