
Abstract
Basic or advanced adult life support is a common scenario in a hospital environment. However, adult resuscitation scenarios are an infrequent occurrence in the surgery or the community at large. The key role of the GP is to provide initial resuscitation prior to potential transfer to a secondary care centre for on going assessment and management.
The GP curriculum and adult resuscitation
requires GPs to:
Be able to recognize death Be able to recognize and evaluate acutely ill patients Keep cardiopulmonary resuscitation (CPR) skills up to date, including use of a defibrillator, with an annual certified resuscitation course Describe how presentation may be changed by age and other factors such as gender, ethnicity, pregnancy and previous health Demonstrate an ability to make complex ethical decisions demonstrating sensitivity to a patient's wishes in the planning of care Provide clear leadership, demonstrating an understanding of the team approach to care of the acutely ill and the roles of the practice staff in managing patients and relatives
To complete their training, the RCGP requires all GP trainees to show competence in adult basic life support (ABLS), correct use of a pocket mask, and safe and competent use of a modern external automated defibrillator in a patient with a shockable rhythm. Trainees will not be expected to use advanced airway techniques (such as endotracheal intubation) or administer drugs. A certificate to prove this competency must be completed by a Resuscitation Council (UK) advanced life support (ALS) instructor or equivalent. Certificates obtained during foundation training are not transferable to GP speciality training.
Even for trained GPs, resuscitation guidelines are continually reviewed. They take into consideration years of international reviews and discussions on ways to improve and manage the adult resuscitation scenario. It is therefore imperative to keep up to date. This article provides a brief overview of the current Resuscitation Council (UK) guidelines and highlights recent changes.
Basic life support
Figure 1 summarizes the steps for ABLS. This sequence may have already been commenced by bystanders, family, friends, staff or other GP colleagues before you arrive. ABLS is carried out to maintain the circulation and oxygen intake of the patient. It is essentially a holding operation in order to sustain life until help arrives. It should be started as soon as cardiopulmonary arrest is detected — the outcome is less good the longer the delay.

ABLS algorithm.
It is vital for rescuers to get assistance as quickly as possible. If you are the only rescuer, go for assistance before starting CPR. If more than one rescuer is available, one should start resuscitation, while another goes for assistance. Another should take over CPR every 2 minutes to prevent fatigue. Ensure the minimum of delay during changeover of rescuers.
In any resuscitation situation, it is important that the rescuers act as a team. One person only should take the lead and direct the process, ensuring that instructions are clear and can be heard. All members of the team should be used effectively with tasks delegated according to skills. For example, if a patient collapses in a GP surgery:
One or two people (depending on the number of people available) could start basic life support One person could be tasked with calling for an emergency ambulance (stating location and that a resuscitation is currently in progress) One person could be asked to fetch the practice resuscitation trolley and automated external defibrillator (AED) One person could look after any relatives or friends that accompanied the patient to the surgery
Danger, response, airway, breathing and circulation
The mnemonic ‘danger, response, airway, breathing and circulation (DR ABC)’ is a useful way to remember the key steps in any resuscitation attempt. ‘D’ stands for danger. In any resuscitation situation, it is important to secure the safety of yourself, your patient and any other bystanders or staff involved. This is particularly important in the community when you may be conducting a resuscitation attempt in a less than ideal location, for example by the roadside.
Next, it is important to assess the patient's response (‘R’). Check for any response (
Is the patient Does he or she respond to Does he or she respond to a Is the patient
If the patient responds by answering or moving, do not move the patient unless he or she is in danger. Get help urgently and reassess regularly. If the patient does not respond, shout for help. Turn the patient onto his or her back and, if possible, move the patient onto a firm surface if not already on one.
‘A’ stands for airway. Open the airway by placing one hand on the patient's forehead and tilting his or her head back. Using the fingertips under the point of the patient's chin, lift the chin to open the airway.
If spinal cord injury is suspected (for example, if the victim has sustained a fall, been struck on the head or neck or has been rescued after diving into shallow water), take particular care during handling and resuscitation to maintain alignment of the head, neck and chest in the neutral position. Try to avoid head tilt if trauma to the neck is suspected. A spinal board and/or cervical collar should be used if available in this situation.
Once the airway is open, the next step is to assess breathing (‘B’). In the first few minutes after cardiac arrest, a victim may be barely breathing or taking infrequent noisy gasps. This is often termed agonal breathing and must not be confused with normal breathing. Look, listen and feel for no more than 10 seconds to determine if the victim is spontaneously breathing with a normal rate and depth. If you have any doubt whether breathing is normal, act as if it is abnormal.
If the patient is breathing normally, turn the patient into the recovery position (Fig. 2), make sure help is coming and reassess regularly for continued breathing If the patient is not breathing or only making occasional gasps or weak attempts at breathing, get help then start chest compressions

The recovery position diagram.
‘C’ is for circulation. If the patient is not breathing, start chest compressions.
Kneel by the side of the victim and place the heel of one hand in the centre of the victim's chest. Place the heel of your other hand on top of the first hand. Interlock the fingers of your hands and ensure that pressure is not applied over the victim's ribs. Do not apply any pressure over the upper abdomen or the bottom end of the bony sternum Position yourself vertically above the victim's chest and, with arms straight, press down on the sternum 5–6 cm After each compression, release all the pressure on the chest without losing contact between your hands and the sternum. Compression and release should take an equal amount of time Repeat at a rate of about 100–120 compressions / minute
Combining chest compressions with rescue breaths
After 30 chest compressions, open the airway again using head tilt and chin lift. Pinch the soft part of the victim's nose closed, using the index finger and thumb of your hand already on his or her forehead. Allow the victim's mouth to open but maintain chin lift.
To give a rescue breath, take a normal breath and place your lips around the victim's mouth (mouth-to-nose technique is an alternative) making sure that you have a good seal. Blow steadily into the victim's mouth for about a second while watching for the chest to rise. Maintaining head tilt and chin lift, take your mouth away from the victim and watch for the chest to fall as air comes out. Take another normal breath and blow into the victim's mouth again to give a total of two effective rescue breaths. Then return your hands without delay to the correct position on the sternum and give a further 30 chest compressions. Continue chest compressions and rescue breaths in a ratio of 30:2.
Stop to recheck the victim if the patient makes a movement or takes a spontaneous breath. Otherwise, resuscitation should not be interrupted.
If rescue breaths do not make the chest rise, check the victim's mouth and remove any visible obstruction (blind finger sweeps are not advised). Recheck that there is adequate head tilt and chin lift. Do not attempt more than two breaths in each 30:2 cycle, before returning to chest compressions.
Resuscitation and infection risk
During resuscitation, precautions should be taken if possible to prevent spread of infection from victim to rescuer or vice versa. There have been isolated reports of transmission of tuberculosis and severe acute respiratory distress syndrome (SARS). Transmission of human immunodeficiency virus (HIV) during CPR has not been reported. Methods to minimize the spread of potential infection risk include the use of gloves, one-way valve masks for giving rescue breaths and single use resuscitation equipment. In cases where equipment is not available to minimize spread of infection, if you are unwilling to give rescue breaths, the Resuscitation Council (UK) recommends giving continuous chest compressions only at a rate of 100 compressions / minute.
Regurgitation during CPR
Some patients regurgitate gastric contents during resuscitation. If this occurs, the patient should be turned away from the rescuer, ensuring that the head is turned towards the floor, the mouth is open with any obstructions removed and that gastric contents can drain out freely. Once gastric contents have drained, the patient should be repositioned to open the airway and recommence CPR with the minimum interruption that is possible.
What has changed in basic life support?
The 2010 Resuscitation (UK) guidelines on ABLS updated the following points as compared to the previous version:
When getting help, ask for an AED Compress the chest to a depth of 5–6 cm and at a rate of 100–120 / minute Do not stop to check the victim or discontinue CPR unless the victim starts to show signs of regaining consciousness, such as coughing, opening his eyes, speaking or moving purposefully and starts to breathe normally Teach CPR to lay people with an emphasis on chest compressions but include ventilation, particularly for those with a duty of care
Automatic external defibrillators
AEDs can now be found in most large shops, airports, offices, factories and sporting venues. In the UK, approximately 30 000 people sustain cardiac arrest outside hospital and are treated by the emergency services each year (Pell et al., 2003). Basic life support will help to maintain a shockable rhythm but is not a definitive treatment. Electrical defibrillation is the only effective therapy for cardiac arrest caused by ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). The scientific evidence to support early defibrillation is overwhelming: the delay from collapse to delivery of the first shock is the single most important determinant of survival. If defibrillation is delivered promptly, survival rates as high as 75% have been reported. The chances of successful defibrillation decline at a rate of about 10% with each minute of delay (Resuscitation Council UK, 2010).
Modern AEDs are suitable for use by lay people and by health care professionals. Some semi-automatic AEDs enable the operator (if CPR trained) to over ride the computer assessment and deliver a shock manually without computer prompting. The National Defibrillator Programme recommends that AEDs in public places or GP practices are not kept in a locked cabinet as this could delay the resuscitation attempt and therefore delay effective cardioversion.
As a GP, you may wish to consider taking the AED from your practice when attending visits to high-risk calls or potential resuscitation scenarios. If you are just starting your general practice placement, it is worth asking your trainer about practice policy. Your practice may have a protocol about this.
How to use an AED
AEDs should be programmed to deliver a single shock followed by a pause of 2 minutes for the immediate resumption of CPR as summarized in Fig. 3. If a patient arrests, start CPR according to the guidelines for basic life support. As soon as the AED arrives:
Switch on the AED and attach the electrode pads. If more than one rescuer is present, continue CPR while this is done. Some AEDs automatically switch on when the AED lid is opened Place one AED pad to the right of the sternum below the clavicle and place the other pad in the mid-axillary line (V5/V6 position) with its long axis vertical. There is often a diagrammatic picture to help with positioning on the pads themselves Follow the voice and/or visual prompts. Ensure nobody touches the victim while the AED is analysing the rhythm If a shock is indicated, ensure that nobody is touching the victim. Push the shock button as directed. Fully automatic AEDs deliver the shock automatically. Immediately resume CPR and continue to follow the prompts If no shock is indicated, immediately resume CPR and continue to follow the prompts
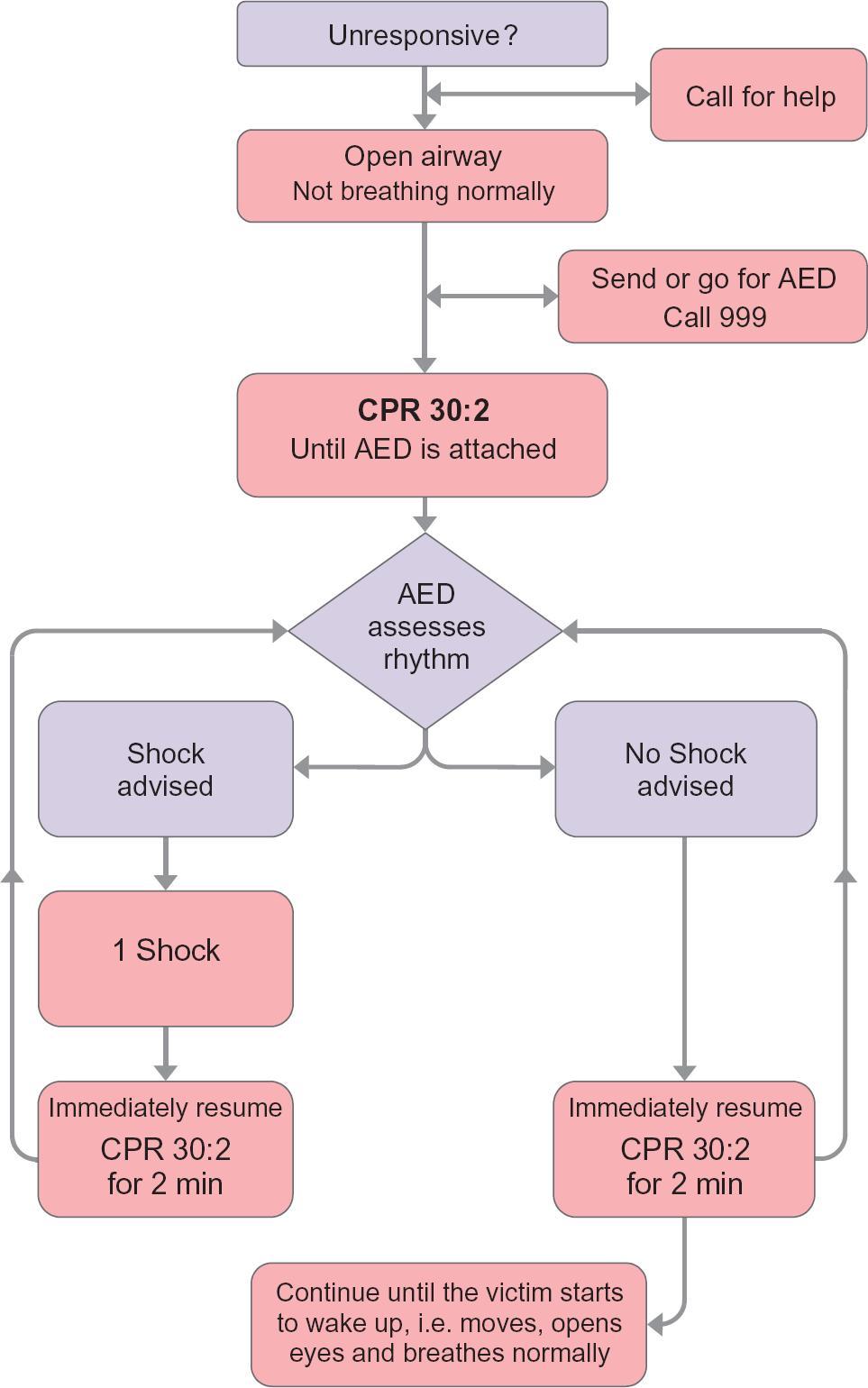
Adult AED algorithm.
If the patient has significant chest hair, then this should be removed if possible to aid efficient conduction. A razor for this purpose may be included in the AED kit. If a razor is not present, then the use of scissors could be considered. However, removal of chest hair should not delay a resuscitation attempt if equipment to do this is not at hand. If the patient is wet, dry the chest quickly before delivering a shock. If oxygen is in use, remove the oxygen supply and attached face mask to at least a metre away from the patient before delivering the shock.
AEDs: what has changed?
Since the previous 2005 guidelines, there has been little change with regards to the use of AEDs. However, the 2010 guidelines highlight that AEDs can and should be used by people with no previous training in resuscitation situations.
Adult ALS
Awareness and ability to use and administer adequate advanced adult life support (ALS) techniques are essential to a GP. The current Resuscitation Council (UK) ALS algorithm is reproduced in Fig. 4. There are three main stages:
Revive the patient using ABLS. Basic life support should be started if there is any delay in obtaining a defibrillator but must not delay shock delivery. In adults, CPR should be performed at a ratio of 30 chest compressions to two rescue breaths. If the airway has been secured and there is more than one rescuer, chest compression should be continued without pausing during ventilation Restore spontaneous cardiac output using a manual or automatic defibrillator Review possible causes for cardiac arrest and take further action as needed
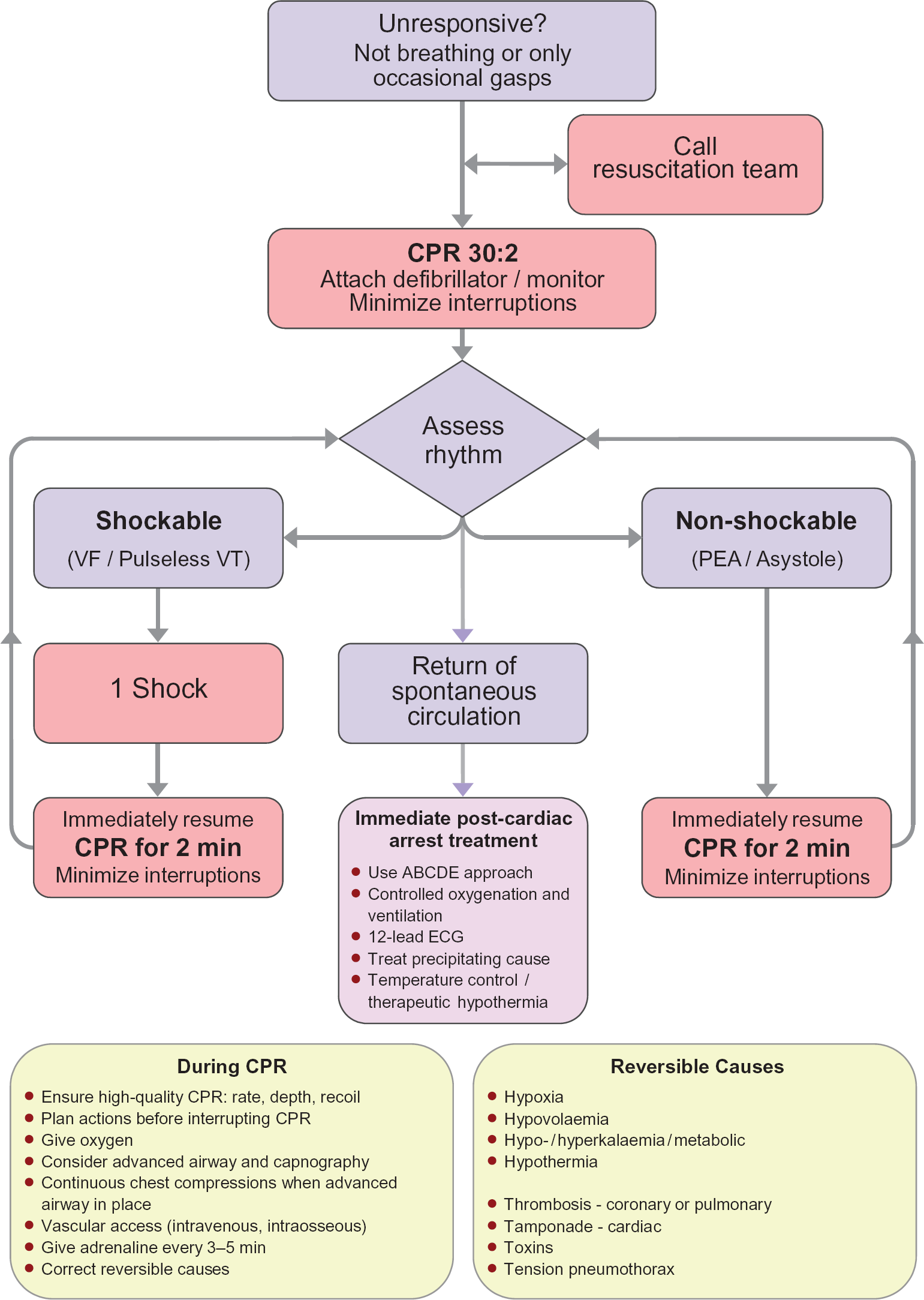
Adult ALS algorithm.
ALS: what has changed?
The overall role of the pre-cordial thump has been de-emphasized (although this can still be performed if the arrest is witnessed and no defibrillator is at hand, as long as it does not delay the initiation of CPR) and the previously recommended period of out of hospital CPR prior to defibrillation has been removed.
The 2010 Resuscitation Council guidance emphasizes the importance of good quality chest compressions without interruptions except to carry out essential tasks, such as rhythm assessment or shock. Compressions should be continued up until the defibrillator is fully charged to enable only a short pause in CPR.
Endotracheal administration of medications is now not advised. If an intravenous route is unavailable, then the intraosseous route should be used.
When treating VF or pulseless VT, 1 mg of adrenaline (epinephrine) is given once chest compressions have restarted after the third shock and then every 3–5 minutes (i.e. during alternate cycles of CPR). In the 2005 Guidelines, adrenaline was given just before the third shock. This subtle change in the timing of adrenaline administration is to separate the timing of drug delivery from attempted defibrillation. It is hoped that this will result in more efficient shock delivery and less interruption in chest compressions. Amiodarone 300 mg is also given after the third shock.
Atropine is no longer routinely advised for use in pulseless electrical activity or asystole.
There is now reduced emphasis on endotracheal tube (ET) intubation. This is to reduce the interruption to adequate CPR while intubation is attempted. ET placement should not be attempted unless the operator is experienced and competent.
Once return of spontaneous circulation (i.e. spontaneous pulse, blood pressure and improvement in general perfusion) has been established, there has been a new emphasis on preventing hypoxaemia. If oxygen saturation can be monitored reliably by pulse oximetry, inspired oxygen should be titrated to achieve oxygen saturations of 94–98% (Resuscitation Council UK 2010).
When to stop resuscitation?
As a GP, usual guidance is to continue resuscitation until further help such as paramedics/ambulance transfer arrives and takes over, the victim starts breathing normally and/or you become exhausted. If the patient starts to breathe spontaneously and normally, turn the patient into the recovery position (Fig. 2) and monitor frequently.
Advanced directives and do not resuscitate orders
Patients within your practice or in the out of hours setting may have an advanced directive declining CPR or a ‘do not attempt to resuscitate’ (DNAR) order in place. Advanced directives must be specific for the situation, written if the person is declining life-sustaining treatment such as CPR and signed by the person declining treatment and a witness.
In some situations, attempting resuscitation of a patient might be inappropriate. This should be discussed in advance by all health professionals likely to be involved with the care of the patient and, where possible, the patient or patient's representative before a DNAR form is completed.
Any decision about whether or not to attempt CPR must be readily accessible to all health professionals who may need to know it (for example, a copy should be kept in the patient's home, the decision should be communicated to local out of hours and emergency ambulance providers and secondary care professionals in the event of hospital admission). The patient's GP record should contain clear documentation of the decision and how it was made, the date of the decision and the reasons for it and the name and position of the person responsible for making the decision. All decisions not to attempt resuscitation should be reviewed regularly in light of the patient's condition. If no explicit decision has been made in advance about CPR and the wishes of the patient are unknown, there should be a presumption that health professionals will make all reasonable efforts to attempt to revive the patient in the event of cardiac or respiratory arrest.
Being prepared
What is your practice protocol for an acute emergency situation such as cardiac arrest? Where is the protocol kept and are you aware of how to implement this protocol in the event of a cardiac arrest in the practice? Where is the emergency equipment kept in the surgery? How does the AED/defibrillator work? Who is responsible for maintaining it? It is essential to find out the answers to all these questions, ideally before you need that information in an emergency situation.
Emergency drugs
Most practices have an emergency drugs kit kept on their resuscitation trolley. GPs usually carry additional emergency drugs in their bags for use outside the surgery. It is important to know where the emergency drugs are kept in your surgery and which drugs/doses are available. There should be a robust system in place for monitoring these drugs and ensuring that they are replaced before they go out of date.
In my own doctor's bag, I tend to group drugs together, i.e. cardiac, respiratory, infection or emergency drugs. I find that this is useful as it prevents me fumbling to find the right drug in acute situations. I also keep a table of the appropriate doses of emergency drugs for different age groups in my bag, for quick reference to ensure that I give the right dose of adrenaline in the emergency situation.
Recording and debriefing
Accurate records of all resuscitation attempts and electronic data stored by most AEDs during a resuscitation attempt should be kept for audit, training and medico-legal reasons. The responsibility for this rests with the most senior member of the practice team involved. Process and outcome of all resuscitation attempts should be audited to allow deficiencies to be addressed and examples of good practice to be shared.
Key points
All doctors, whether working in a hospital or the community, should be trained in resuscitation techniques; these skills should be refreshed at least annually Basic life support is a holding process designed to sustain life until further help arrives. It involves assessment of danger, response, airway, breathing and circulation All GP practices should have an AED and all GPs should be able to use one ALS aims to sustain life using basic life support techniques but also to restore normal rhythm and cardiac output with the use of a defibrillator and/or to use drug treatment to restore cardiac output All resuscitation attempts should be documented and audited as significant events