
Abstract
Traumatic brain injury (TBI) is a physical injury to brain tissue that temporarily or permanently impairs the brain's function. The causes include road traffic accidents (64.1%), falls (19.3%), assaults (5.1%) and sporting activities (2%). Primary injury occurs at the time of impact and is irreversible. During this time, brain function may be immediately impaired by direct damage to brain tissue. Further damage triggered by the primary injury can occur shortly after, leading to secondary injury. The aim of prehospital management is to stabilize and treat the damage from the primary injury and to prevent and manage secondary injury.
The GP curriculum and head injury
Recognize and evaluate acutely ill patients Describe differential diagnoses for each presenting symptom Describe how the presentation may be changed by age and other factors such as gender, ethnicity, pregnancy and previous health Understand indications for emergency referral of people with intracranial haemorrhage and raised intracranial pressure Demonstrate an ability to use telephone triage: to decide to use ambulance where speed of referral to secondary care or paramedic intervention is paramount to make appropriate arrangements to see the patient to give advice where appropriate Demonstrate an ability to use the ‘ABC’ principles in initial management of severe head injuries
Epidemiology
TBI is a leading cause of death worldwide. Every year, around 1.5 million affected people die and several millions receive emergency treatment. In the UK, the annual attendance to the emergency department with a head injury is 6.6%; 70–88% of people who sustain a head injury are male and 10–19% are greater than 65 years of age. Alcohol may be involved in up to 65% of adult head injuries.
Classification
The severity of TBI is categorized by the patient's Glasgow Coma Scale (GCS) score (Table 1). The GCS is used to describe the general level of consciousness. The total score is determined by adding the scores obtained in each of the three categories, with 15 being the maximum and 3 the minimum.
Glasgow Coma Scale

Severe TBI is classified as a GCS score between 3 and 8 and accounts for approximately 10% of cases. A further 10% are classified as moderate TBI with a GCS score of 9–12. The vast majority (80%) are classed as mild TBI with a GCS score of 13–15. It is important to remember that a patient's GCS score should be continually reassessed as it can rapidly deteriorate.
Injuries are usually classified as open or closed. Open injuries involve penetration of the scalp, skull and often the meninges and brain tissue. They are associated with bullets or sharp objects. Closed injuries occur when the head is struck by or strikes an object (for example, the floor following a fall). Good knowledge of the anatomy of the brain and skull is crucial to understanding the pathophysiology of these brain injuries.
Open injuries
Open injuries can be caused by fractures. Depressed fractures and basal skull fractures are relatively common in TBI.
Depressed fractures result from a direct blow to the skull with a blunt object. Most occur over the frontoparietal region due to its decreased bone density. As these fractures are at great risk of damaging the brain tissue underneath, their presentation will vary depending on the presence of associated intracranial injuries. Figure 1 shows a depressed frontal fracture.
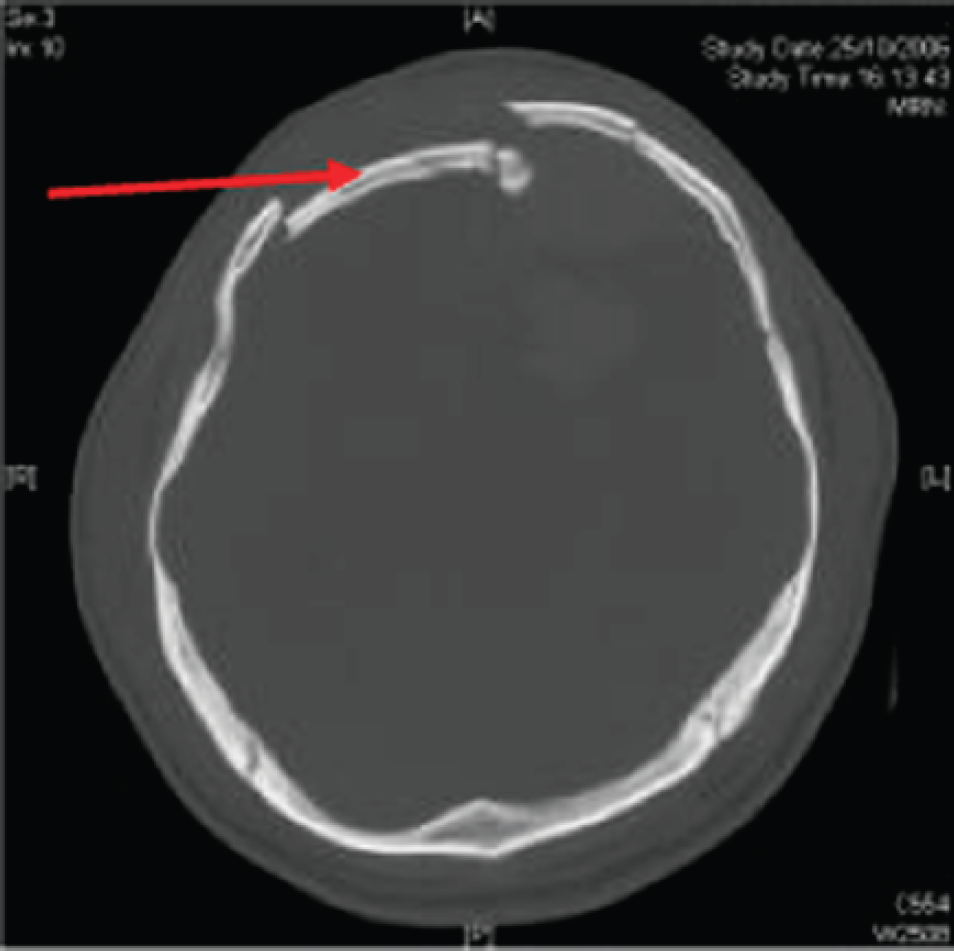
Depressed frontal fracture.
Basal skull fractures usually involve the temporal bone, the occipital bone, the sphenoid bone and the ethmoid bone. These fractures often extend into the sinus cavities tearing the dural membrane causing cerebrospinal fluid (CSF) to leak into the nose and ears. A concern is that the tear in the dura may provide a route for infection. Basal skull fractures will present with symptoms specific to the location of the fracture and include:
Raccoon eyes (periorbital ecchymosis) Battle's sign (mastoid ecchymosis) Rhinorrhea or otorrhea (CSF leaking from the nose or ear, respectively) Haemotympanum (blood in the middle ear) Cranial nerve defects—unilateral hearing loss, vertigo and occulomotor palsy Signs of brainstem compression—hypotension, tachycardia and changes to respiration
Patients that present with either raccoon eyes or Battle's sign should be treated with a high index of suspicion. Raccoon eyes usually occur immediately, while Battle's sign tends to appear within the first 24–48 hours. Fig. 2 depicts a patient with raccoon eyes, while Fig. 3 shows a patient with Battle's sign.

Raccoon eyes.: With kind permission from Springer Science + Business Media: International Ophthalmology, Koray Gumus, A child with raccoon eyes masquerading as trauma (2007) 27: p. 379–81, Fig. 1.

Battle's sign.
Closed injuries
The brain sits inside the skull floating in a bath of approximately 150 ml of CSF. This renders the brain vulnerable to excessive movement within the skull when subjected to significant forces. The skull's numerous ridges mean that the brain is at risk of contusion as it glides over these ridges following impact. For this reason, vascular and axonal shearing can also occur. Sheared vasculature can lead to extradural, subdural and intracerebral haematomas.
Extradural haematoma
Extradural haematomas form between the skull and the dura. They are most commonly associated with blunt trauma to the head; in 85–95% of patients with this type of trauma, there is an overlying skull fracture. Damage to the middle meningeal artery is usually responsible for this type of haemorrhage and for this reason, extradural haematomas tend to occur in the temporoparietal region (specifically the pterion). Patients typically present with a severe headache and an impaired level of consciousness. Only 20% of cases follow the classical presentation of a lucid period between the initial trauma and onset of neurological signs. Subsequent brain herniation (see below) can cause contralateral hemiparesis and ipsilateral pupil dilation.
Subdural haematoma
Subdural haematomas (SDHs) form between the dura and arachnoid. They are often due to damage to veins bridging this space. The subdural space enlarges as the brain atrophies with increasing age (and in alcoholics). This places increased strain over these veins making them more susceptible to damage. For this reason, SDHs are more common in the elderly, especially those on anticoagulants.
SDH can present either acutely or chronically. An acute SDH usually presents within 48 hours of the initial trauma and should be suspected whenever the patient has suffered severe blunt head trauma. Acute SDH carries a high mortality and morbidity rate. Patients can present with nausea and vomiting, drowsiness, blurred vision or slurred speech.
Chronic SDH can be easily missed as half of all cases present without a history of a fall, symptoms and signs often take 2–3 weeks to manifest. Patients may complain of progressive symptoms such as an unexplained headache or personality changes. A SDH should always be considered in a confused elderly patient. Bear in mind that any patient with coagulopathy (haemophiliacs and chronic alcohol users) can develop SDH after seemingly minor trauma. Fig. 4 shows a chronic SDH.

Chronic SDH.
Intracerebral haematoma
Intracerebral haematomas are bleeds that occur within the brain tissue itself. Typically, they occur on the opposite side of the skull to the point of impact (a contrecoup injury). The inferior frontal and anterior temporal lobes are common sites of haematoma following a blow to the back of the head. Symptoms typically begin with a sudden onset headache and loss of consciousness, often within seconds or minutes. The patient may feel nauseous, experience episodes of delirium or develop focal or generalized seizures. Neurologic deficits are usually sudden and progressive and may lead to hemiparesis. If haemorrhage occurs in the posterior fossa, it can cause cerebellar or brainstem deficits.
Brain herniation
Brain herniation is a complication of raised intracranial pressure. The skull is divided into three compartments by the falx cerebri (which divides the two cerebral hemispheres) and the tentorium cerebelli (which divides the cerebellum from the cerebral hemispheres). The openings of these compartments are marked by prominent dural edges. Significant increases in intracranial pressure force the brain out through these openings, rendering it susceptible to injury by the dural edges.
Pathophysiology
In order to manage TBI effectively, it is important to understand the concepts behind the Monro-Kellie doctrine. The brain is housed by the skull, which is essentially an inelastic vault. The Monro-Kellie doctrine states that because the total intracranial volume is fixed, only small increases in volume within the skull can be tolerated before the intracranial pressure (ICP) rises dramatically. The intracranial volume (Vi/c) (1500 ml) is equal to the sum of its components:

The three components must be kept at equilibrium as a rise in the volume of one component must be compensated by a decrease in the volume of the other components.
When a significant TBI occurs, cerebral oedema can occur, causing the volume of the brain to increase. Initially, this is compensated by an increase in CSF being displaced into the spine; however, once the ICP rises to around 25 mmHg, small increases in volume will result in large increases in ICP, which can compromise cerebral perfusion.
Cerebral perfusion pressure (CPP) is defined as the difference between the mean arterial pressure (MAP) and the intracranial pressure (ICP). In other words:

In normal functioning brains, a system is in place to ensure that cerebral blood flow is maintained. This system is known as autoregulation. It is performed by arterioles, which are able to constrict and relax within a specific pressure range (50–150 mmHg) to maintain constant blood flow. Outside these pressure values, the arterioles are unable to autoregulate and blood flow becomes entirely dependent on systemic blood pressure.
Increases in ICP can cause ischaemia and later infarction as they lower CPP. The brain responds by increasing MAP by dilating the blood vessels. An increase in MAP causes cerebral blood flow to increase; however, this also increases ICP again, causing a vicious cycle. Significant increases in ICP can cause midline shifts, which can compress the ventricles resulting in hydrocephalus. Raised ICP can also cause herniation. For these reasons, the maintenance of ICP can significantly improve patient outcome and so is crucial in the management of TBI.
Managing head injuries in general practice
In primary care, there are two types of patient that you are likely to see with head injuries: those with minor head injuries that present in the surgery and elderly people presenting several days after head injury with neurological sequelae. Rarely, you may also be called upon to attend a serious head injury, for example if you stop at a road accident.
Minor head injuries
Minor head injuries are differentiated from severe head injuries by the absence of an extended period of unconsciousness. When presented with a minor head injury, it is important to elicit a history from both the patient and a witness if possible.
Details surrounding the incident are crucial to aid you in forming differentials. You should consider asking how exactly the head injury happened, when it occurred, where the impact was etc. It is important to ascertain whether the patient lost consciousness and whether there were any seizures as these can indicate developing secondary brain injuries. Does the patient recall the whole incident? Retrograde amnesia (before the incident) is more significant than anterograde amnesia (after the incident) and should be taken seriously. Patients should also be asked about any current symptoms that they are experiencing such as visual, hearing or olfactory disturbances and whether their behaviour has changed in any way.
Start the physical examination by looking at the body and limbs and then the head and neck. If a fall is suspected, the hip joint should be examined for potential fractures. As neck injuries often accompany head injuries, examine each cervical spinous process for signs of a fracture. Look for any signs indicative of a basal skull fracture. Check the scalp and head for any obvious injuries (e.g. lacerations).
A neurological examination should then be performed assessing power (looking for signs of unilateral weakness), sensation and reflexes in all limbs. Examine the pupils; a noteworthy sign is discrepancy between the size and reactivity of each pupil, which may signify underlying pathology. Check the fundi for signs of haemorrhage or raised intracranial pressure. Box 1 illustrates when a patient should be referred to the emergency department.
If the examination is normal and the patient displays none of the features listed in Box 1:
Give written discharge advice (Box 2) on the ‘do's and don'ts’ following a head injury and the warning signs that should trigger re-consultation Warn patients (and carers) that they may suffer mild headaches, tiredness, dizziness, tinnitus, poor concentration and poor memory for the next few days Advise rest and paracetamol (not codeine-based analgesics) for headaches
A patient should be referred to the Accident and Emergency Department if any of the following are present.
A GCS score of less than 15 at any time since the injury Any loss of consciousness Focal neurological deficits since the injury—dysarthria, decreased sensation, loss of balance, weakness, visual changes, abnormal reflexes, ataxia, irritability or altered behaviour Any suspicion of a skull fracture—penetrating head injury, blood or CSF from the nose or ear, raccoon eyes, Battle's sign, serious scalp laceration or haematoma Amnesia Persistent headache Vomiting Seizure Any previous cranial neurosurgical interventions High-energy head injury (e.g. road traffic accident, a fall of greater than 1 m, a fall of greater than 5 stairs) History of a bleeding or clotting disorder or on anticoagulant therapy Difficulty in assessing the patient—if very young, elderly, intoxicated or epileptic Suspicion of non-accidental injury Inadequate supervision at home
If a patient has a GCS score of less than 15, neck pain/tenderness, focal neurological deficit or paraesthesia of the extremities his/her neck should be immobilized and he/she should be referred to the Emergency Department.
Elderly patients
The second group of patients with head injuries that you are likely to see in primary care are elderly patients who are behaving ‘unusually’. The patient may not volunteer a history of a head injury; however, when questioned directly about a fall, one will often emerge. It is important to consider the possibility of a potential head injury in elderly patients who present with an unsteady gait and a recent onset of confusion, in conjunction with long-standing headaches. Bear in mind that the elderly are particularly susceptible to subdural haemorrhages, especially those on anticoagulants. These head injuries can take several days/weeks to manifest. In this situation, the key thing to do is to admit the patient to hospital for further investigations if you suspect a SDH.
Severe head injury
Rarely as a GP, you may be placed in a position where you have to deal with a severe head injury. It may be necessary for you to make sure that help in the form of the emergency services is on its way. You may also have to perform basic life support until the ambulance arrives.
Some tips and general advice following a head injury.
If you experience Increasing drowsiness Worsening headache Confusion or strange behaviour Two or more bouts of vomiting Focal neurological problem, e.g. limb weakness, dizziness, loss of balance or convulsions Any visual problems such as blurring of vision or double vision Blood, or clear fluid, leaking from the nose or ear Unusual breathing patterns Show a relative or friend this advice leaflet so that they too know what symptoms to look out for
Stay within easy reach of a telephone and medical help for the next few days
Discuss with your doctor about playing contact sports such as rugby or football. It is often advised that you should not play contact sports for three weeks following a head injury
Firstly, ensure the safety of yourself, the patient and any bystanders and assistants. Do not move the patient unless absolutely essential; if moving the patient, take utmost care to immobilize the cervical spine first.
The Advanced Trauma Life Support (ATLS) protocol is the recommended trauma management guideline designed to be undertaken at the scene of the accident to optimize patient outcome. It involves the following steps:
Airway obstruction is one of the major causes of death in patients with treatable head injuries. If starved of oxygen for just a few minutes, brain tissue cells will undergo irreversible damage. Therefore, it is important to maintain the airway either by using the simple ‘jaw thrust, chin lift’ technique, by creating a nasopharyngeal airway or by endotracheal intubation.
It is important to note that if a cervical spine injury is suspected, the cervical spine should be immobilized before the ‘jaw thrust chin lift’ is performed. If a basal skull fracture is suspected, then the decision to place a nasopharyngeal airway should be considered very carefully, weighing the potential benefits against the risks of intracranial placement.
Once the airway is maintained, 100% oxygen should be given if available. It is recommended that unconscious patients with a GCS score of 8 or under or those unable to maintain adequate airway should be intubated. However, do not attempt this unless you have up-do-date knowledge and skills and suitable equipment to perform this procedure.
Long-term complications of head injury
Most people recover quickly from mild head injury without experiencing any long-term problems. However, people suffering moderate or serious head injury are more likely to require rehabilitation and ongoing treatment.
Post-concussion syndrome is a complication of head injury. It refers to a collection of mental, psychological and cognitive symptoms that patients may experience shortly after their head injury. These can include continual headaches (most common), dizziness, double vision, personality changes and the inability to concentrate. Some patients develop post-concussion syndrome immediately, others after a few weeks or months and in some cases longer. Patients should be warned that they may experience post-concussion syndrome even after minor head injury and advised that they should return to their GP if they experience any of its symptoms.
Although most people's symptoms last a few weeks, they can persist for much longer. While there is no definitive treatment, many patients find just the diagnosis and an explanation of what is happening comforting. Advice about things to avoid (e.g. alcohol, stress etc.) may be useful and painkillers, medication for nausea or antidepressants may also be helpful. The brain injury association, Headway (www.headway.org.uk), produces helpful factsheets for patients, their families and for health professionals. It also has a national helpline to provide advice for patients (telephone 0808 800 2244) and runs local support groups.
Conclusions
The cost of TBI is staggering both from an economic and from an emotional standpoint. In 2008, TBI care in the UK cost £266 million. Almost 100% of people with severe TBI and two-thirds of those with moderate TBI do not return to their premorbid function. Preventing secondary injuries is the cornerstone of good prehospital management. The importance of the GP in recognizing triggers for referral to the emergency department should not be underestimated. A thorough history and examination can detect developing head injuries. Swift detection and referral saves lives.
Key points
GPs may encounter head injuries in primary care and must know how to manage them safely; swift detection and referral of patients with complications saves lives Severe head injuries encountered in the community should be managed by calling for ambulance support and using an ABCDE approach Patients presenting with more minor head injuries to primary care should be assessed for factors that warrant referral to the emergency department, and if not referred, should be given an information sheet providing information about how to manage their head injury and when and how to seek further medical attention Elderly patients and alcoholics are particularly at risk of SDH, which may present without a clear history of head injury; always have a low threshold to refer for specialist assessment Even minor head injuries may have longer term sequelae such as post-concussion syndrome