
Abstract
Cardiovascular disease (CVD) is a spectrum of disorders that includes stroke, coronary heart disease (CHD) and peripheral vascular disease (PVD). CVD is the UK's biggest cause of death, with over 191 000 deaths a year. The extent to which CVD affects the health of the population and the financial burden this places on the National Health Service (NHS) makes it an important modifiable disease. Preventing CVD is now a significant role of the general practice team.
The GP curriculum and primary prevention of cardiovascular disease
Manage primary contact with patients who have a cardiovascular problem
Promote cardiovascular well-being by applying health promotion and disease prevention strategies appropriately
Describe strategies for early detection of cardiovascular problems that may already be present but have not yet produced symptoms
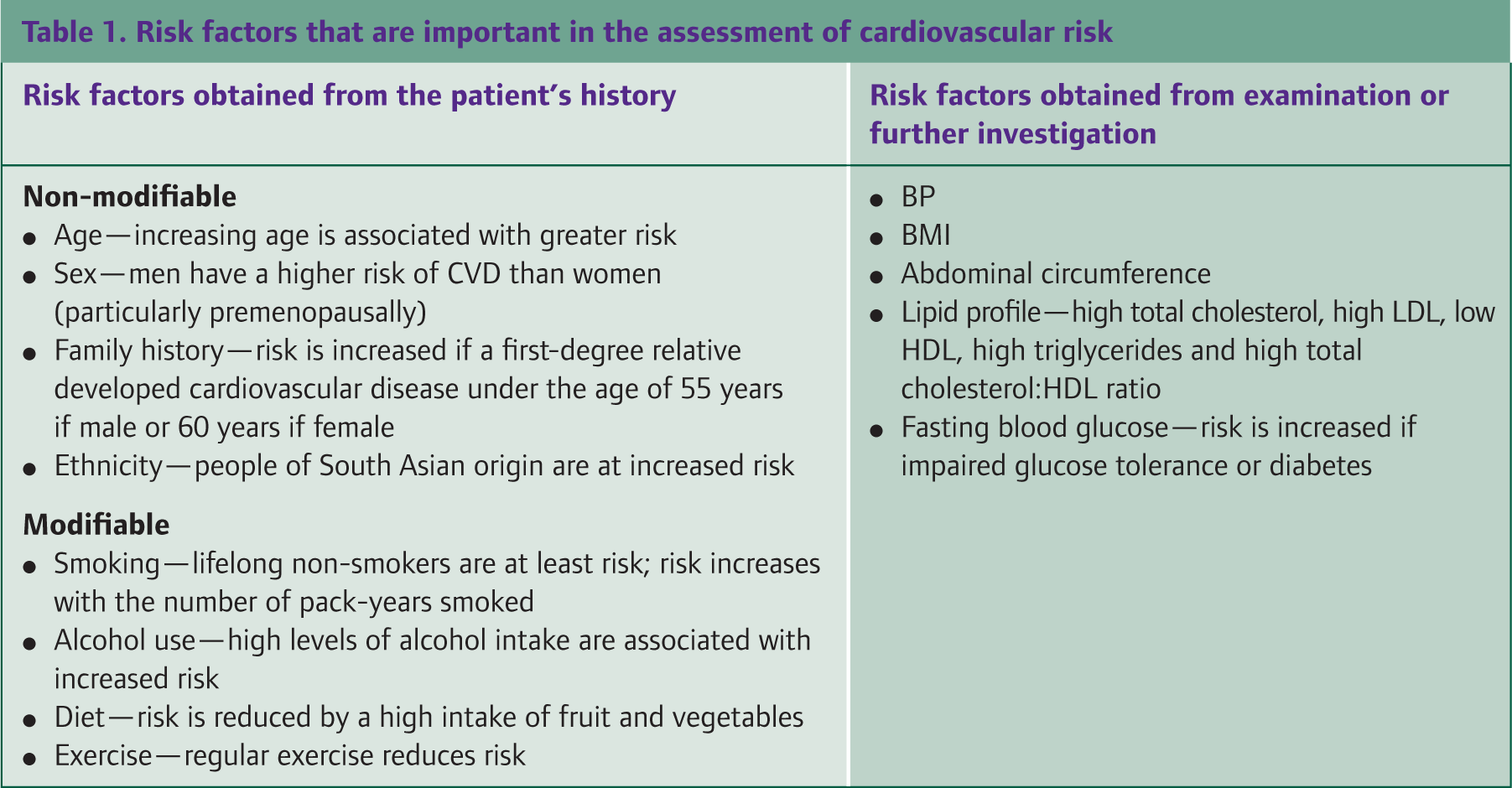
Recognize important modifiable risk factors for CVD which include, blood pressure (BP), diabetes, lipids, smoking, alcohol, exercise, obesity and diet
Recognize important non-modifiable risk factors for CVD which include age, ethnicity, sex and family history
Understand the importance of combining risk factors—risk calculation and communicating risk
Communicate the patient's risk of cardiovascular problems clearly and effectively in a non-biased manner
Describe and be able to implement the key national guidelines that influence health care provision for cardiovascular problems
Describe the key research findings that influence management of cardiovascular problems (e.g. heart protection study)
Calculation of cardiovascular risk
The development of CVD is due to the build up of atherosclerotic plaques within the sub-intimal regions of arteries. These plaques can take many years to develop and remain largely asymptomatic until a critical event. The period before an acute event is an essential time when physicians can intervene to slow down and even reverse this process.
Screening for cardiovascular risk
Many patients in primary care carry risk factors associated with the development of CVD. In the Health Survey for England (2006), it was found that 23% of men and 21% of women aged 16 years or over smoked cigarettes. The same survey also estimated that 24% of both men and women were classified as obese [a body mass index (BMI) of more than 30 kg/m2]. Hypertension (defined as a BP of less than or equal to 140/90 mmHg) was seen in 31% of men and 28% of women, with 57% of men and 61% of women having a total blood cholesterol level of 5.0 mmol/l and over.
These CVD risk factors are usually silent and tend to cluster with synergistic effects. This created the basis for cardiovascular risk surveillance in asymptomatic individuals at the age of 40 years and every 5 years thereafter (Box 1).
It is recommended that routine screening for identification of cardiovascular risk factors starts at the age of 40 years (NICE, 2008). Venues outside GP surgeries, such as pharmacies and community fairs, may also conduct CVD screening. The idea behind such initiatives is to try and increase uptake of the checks and reach people that traditionally might not attend their GP surgery.
Patients considered high risk for CVD
Patients with any form of established atherosclerotic CVD including coronary heart disease (CHD), cerebrovascular disease (such as stroke and transient ischaemic attack) and peripheral vascular disease (PVD)
Patients with a diagnosis of diabetes mellitus
Asymptomatic patients without CVD who have a combination of risk factors that puts them at a 20% or greater risk of a primary cardiovascular event (estimated using a risk calculator) over the next 10 years
Identification of risk factors
Identification of the risk factors as part of cardiovascular surveillance is best done using a brief targeted history in combination with a physical examination and biochemical tests. Important risk factors that should be documented for cardiovascular risk assessment are highlighted in Table 1, with new risk factors are being identified all the time.
Risk factors that are important in the assessment of cardiovascular risk
The INTERHEART study is a large case—control study that looked at risk factors associated with acute myocardial infarction (AMI) across 52 countries (Yusuf et al., 2004). This study highlighted nine risk factors that were strongly associated with incidence of AMI and thus CVD. These were apolipoprotein B (Apo B) to apolipoprotein A-1 (Apo A-1) ratio, smoking, hypertension, diabetes, obesity, diet, physical activity, alcohol consumption and psychosocial factors (Table 2). Many of these factors are easily identified within the primary care setting and can be used in risk stratification. Apo B is a major constituent of low-density lipoprotein (LDL) cholesterol, while Apo A-1 is a major constituent of highdensity lipoprotein (HDL) cholesterol. While levels of Apo B are probably a better indicator of cardiovascular risk than LDL levels, Apo B levels are not routinely tested in the UK.
Data from the INTERHEART study showing risk of AMI associated with risk factors in the overall population

Psychosocial stress was assessed by four simple questions about stress at work and at home, financial stress and major life events in the past year. Additional questions assessed locus of control and presence of depression.
Although long suspected in clinical practice, this study was one of the first to show that psychosocial factors might contribute to AMI. People who had suffered AMI and were still working experienced more work stress than controls [odds ratio (OR) 2.14; 99% confidence interval (CI) 1.73–2.64]. Sustained stress at home similarly increased the chances of having an AMI (OR 2.12, 99% CI: 1.68–2.65). Financial stress, stressful life events in the past year and depression were also more common among those who had sustained AMI than controls (Rosengren et al., 2004).
Cardiovascular risk stratification
The way in which people are stratified with regards to their risk of developing CVD is regularly being revised. In 2000, the Department of Health introduced the National Service Framework (NSF) for the prevention and treatment of CHD in the UK. It recommended the use of the Joint British Societies' (JBS-1) coronary risk prediction charts to estimate total CHD risk in asymptomatic patients without coronary artery disease (CAD).
In 2005, there was a revision of the NSF guidelines and the formation of the new JBS-2 guidelines with new risk prediction charts. Guidelines redefined risk in terms of CVD instead of CHD. In other words, the risk of having a stroke, heart attack or developing PVD as opposed to solely the risk of having a heart attack. High risk for disease was redefined as 20% for a CVD event over the next 10 years. The JBS charts for CVD risk (Figure 1 and Figure 2) are for non-diabetic men and non-diabetic women only and use six variables (gender, age, smoking status, BP and total cholesterol and HDL) to predict CVD risk.

JBS CVD risk prediction chart: non-diabetic men.

JBS CVD risk prediction chart: non-diabetic women
In 2008, the National Institute for Health and Clinical Excellence (NICE) brought out guidance on lipid modification (NICE, 2008). This included a recommendation for the use of the Framingham equation, rather than the JBS-2 chart, to calculate cardiovascular risk. The guidance was subsequently updated in 2010 when that recommendation was amended to include other validated and suitable risk calculators. Table 3 highlights risk prediction programmes now commonly used in UK practices.
Cardiovascular risk prediction tools for specific populations

When to treat
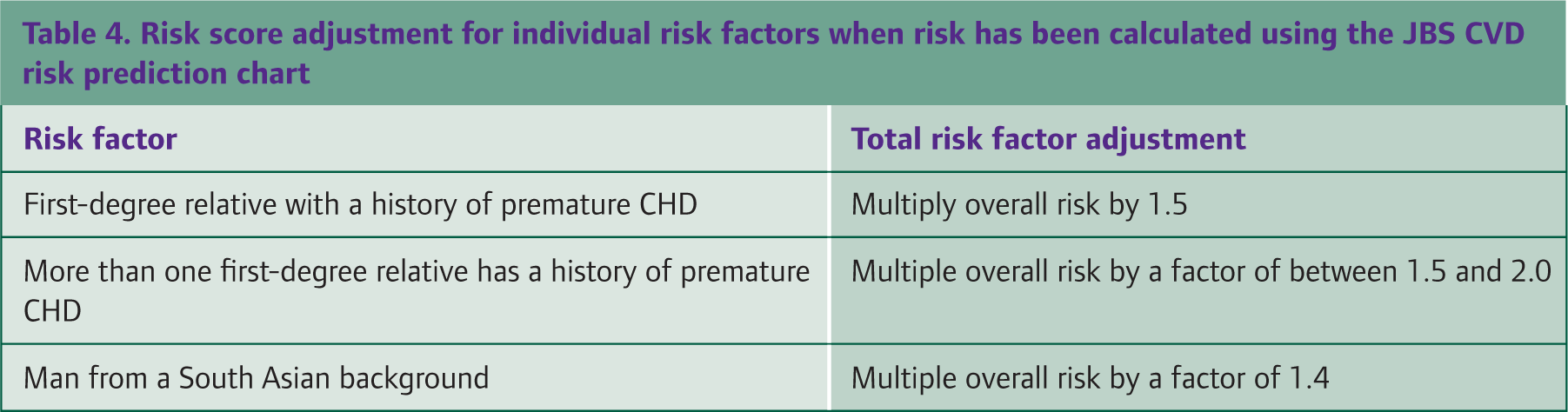
There are some limitations with the use of CVD risk calculators. One disadvantage is that they do not appreciate the full range of contributory factors associated with the development of atherosclerotic disease. Therefore, it is important to refine the CVD risk predicted by a risk calculator according to any additional patient-specific risk factors (Table 4) to create an overall estimate for that individual. Many practices have computer systems that will provide a CVD risk based on the available data but it is important to understand how these figures are obtained: it is very easy to be caught out by a subtle difference between CVD risk and CHD risk. Although the computer will often calculate a risk score for any patient, it is important to remember that CVD risk calculations using standard risk calculators are not applicable for patients already at high risk of CVD, such as those with:
Risk score adjustment for individual risk factors when risk has been calculated using the JBS CVD risk prediction chart
a previous history of CHD, cerebrovascular or peripheral vascular disease and/or
familial hypercholesterolaemia or any other genetic disorder of lipid metabolism
Most people with diabetes are automatically at high risk of CVD, including type 2 diabetics of any age and type 1 diabetics under the age of 35 years with additional risk factors for CVD and all type 1 diabetics over the age of 35 years. Cardiovascular risk for people with type 2 diabetes with no additional risk factors can be estimated using specialized risk calculators such as the ‘UK Prospective Diabetes Study Risk Engine’ (Diabetes Trials Unit, 2001).
For patients for whom risk calculations apply, if a patient is approaching a CVD risk of 20%, it is important to ensure that your data are as accurate as possible. For example, by obtaining an average of three BP readings, ensuring that the fasting lipid profile is recent and the BMI is up to date.
Communication of cardiovascular risk to patients
Discuss the importance of risk identification and stratification with patients, emphasizing in particular its positive health implications. To ensure good communication, afford sufficient time with patients using language that is jargonfree and targeted to their comprehension level. In order to initiate a successful risk reduction plan, an absolute risk value should be given to the patient, with a simple explanation of what it means.
Explain that risks are just estimates and are subject to change with intervention. Follow-up those at risk with regular reviews, documenting their progress, adjusting their CVD risk estimates and revising their goals for the future. Remember that patients may decline to participate in health improvement strategies. In this instance, it is important to use good communication skills to identify factors that could act as a barrier to primary prevention. A patient may not be ready to make lifestyle changes now but may be willing to next year.
Lifestyle modifications
Risk factor modification in all high-risk patients should begin with changes in lifestyle. Alterations in smoking habit, diet, alcohol intake and exercise could greatly reduce the impact of individual risk factors and even negate lifelong pharmacological intervention. Despite the great benefit this may have on a patient's global cardiovascular risk, it is often overlooked. Lifestyle modification can be achieved through a strong doctor—patient relationship, a structured programme that involves all members of the multi-disciplinary team and regular contact between patient and clinician. Consultation techniques such as motivational interviewing should also be considered (Storr, 2011). Attitudes towards healthy living can also be supported nationally through government initiatives, such as the NSF, Food and Health Action Plan and Local Exercise Action Plans (LEAP).
Smoking
There is a plethora of evidence that implicates both active and passive smoking to the development of CVD. The risk is proportional to the number of pack-years smoked, and stopping smoking can derive benefits almost immediately. Irrespective of cardiovascular risk, smoking cessation advice should be given at every opportunity, with the use of the five ‘A's’ of smoking cessation (Box 2).
The five A's of smoking cessation
A number of interventions have been proven to be effective in helping people quit smoking. Through a referral to a local National Health Service (NHS) stop smoking scheme; individual counselling, group behavioural therapy, nicotine replacement therapy (NRT) and oral medications such varenicline or bupropion can be initiated.
Obesity
Obesity in the form of BMI and particularly abdominal obesity has been directly linked with the development of CVD. Certain cardiovascular risk factors such as insulin resistance, dyslipidaemia and hypertension cluster with abdominal obesity to form a disease entity called metabolic syndrome (Box 3). The diagnosis of metabolic syndrome is not a disease entity, but a constellation of signs that does not infer an immediate high risk of CVD, but it does indicate a probable progression and thus a need to intervene with lifestyle modifications aggressively.
Diagnosis of metabolic syndrome
Increased waist circumference (greater than or equal to 102 cm in men and greater than or equal to 88 cm in women; greater than or equal to 90 cm in Asian men and greater than or equal to 80 cm in Asian women)
Elevated triglycerides (greater than or equal to 1.7 mmol/l)
Decreased HDL cholesterol (less than 1.03 mmol/l for men and less than 1.29 mmol/l for women)
BP more than 130/85 mmHg or active treatment for hypertension
Fasting plasma glucose level more than 5.6 mmol/l or active treatment for hyperglycaemia
Saturated fats
One of the most important lifestyle modifications for primary prevention is changing to a healthier diet. Fats, particularly saturated fats, have long been thought to be associated with atherosclerotic plaque formation and the development in cardiovascular risk. Examples of food high in saturated fats include processed meats, lard and whole-milk dairy products. However, recent randomised controlled trials (RCTs) and prospective observational studies have not supported this theory. A meta-analysis looked at 21 studies and concluded that the intake of saturated fat was not associated with an increased risk of CHD, stroke or CVD (Siri-Tarino et al., 2010). Current evidence does however indicate that replacing saturated fats with polyunsaturated fatty acids (omega-three polyunsaturated fatty acids) is associated with a reduction in CVD. Food high in polyunsaturated fats includes: fish, whole grain wheat and sunflower seeds.
Recommendation of plant sterols and stanols as part of a low fat diet is controversial. The food industry heavily promotes these products that are sold as margarines, yoghurts and health drinks, as a means of lowering cholesterol. However, although there is some evidence that shows that they do lower cholesterol, there is currently no evidence that they reduce CVD risk. Therefore NICE (2008) does not endorse their use.
Salt intake
Reducing salt in the diet reduces BP and thus reduces cardiovascular risk. A reduction of salt intake of 6 g/day (2.3 g sodium/day) predicted a fall in BP of 7.11/3.88 mmHg in patients with hypertension and 3.57/1.66 mmHg in normotensive individuals [Scottish Intercollegiate Guidelines Network (SIGN, 2007)]. Currently, the Food Standards Agency (FSA) recommends individuals to consume only 6 g/day (one teaspoon), with individuals with hypertension advised to reduce intake to as little as possible.
Fruit and vegetable intake
Fruit and vegetables are known to contain many nutrients thought to reduce CVD, such as potassium, folate, vitamins, fibre and other anti-oxidants. One meta-analysis which included 12 studies demonstrated increasing fruit and vegetable consumption to more than five servings/day was related to a 17% reduction in CHD risk (He et al., 2007). The Department of Health continues to encourage fruit and vegetable consumption in the UK by its ‘five a day’ campaign that began in 1997. This was further supported by the government's introduction of the schools fruit scheme.
Exercise
All forms of physical exercise are associated with improvements in cardiovascular risk. Data from the INTERHEART (Yusuf et al., 2004) study showed significant reductions in the incidence of myocardial infarction in individuals taking part in moderate exercise (walking, cycling or gardening) or strenuous exercise (jogging, football and vigorous swimming) for 4 hours or more a week. There are multiple ways to encourage exercise in the primary care setting: simple advice during a consultation, referring to specific counselling services, recommending facilities or services such as local walking programmes or referring into a specific ‘exercise referral system’.
Alcohol
Alcohol is known to have both positive and negative associations with CVD. The classic ‘J’ shaped curve, which indicates a lower cardiovascular risk associated with moderate alcohol consumption and higher risk with higher consumption, has been repeated in numerous studies. A meta-analysis in 2002 showed a reduction of 32% in overall cardiovascular risk associated with drinking wine with maximum benefit at 150 ml/day for wine (Di Castelnuovo et al., 2002). The general consensus is that moderate amount of alcohol for a patient is cardioprotective with no more than 2–3 units of alcohol per day for women and no more than 3–4 units for men, with at least two drink-free days per week.
Pharmacological interventions
Initiation of any pharmacological treatment should always be in combination with lifestyle modification. Most pharmacological interventions once started are lifelong and are associated with a number of risks. The guidelines below are recommendations based on best evidence, but this can never replace clinical evaluation of the risk benefit analysis for each individual patient. Issues such as pre-existing diseases, current medications, compliance, stigmata of lifelong medication and side effects need to be weighed against any potential benefit.
Antihypertensive medication
Numerous trials and studies have been conducted that showed that reduction of BP is associated with fewer cardiovascular events and lower cardiovascular mortality, irrespective of the antihypertensive used. One Health Technology Assessment has shown that reduction of diastolic BP by 5 mmHg reduces the risk of stroke by 34% and ischaemic heart disease by 21%. Pharmacological control of hypertension in patients with a CVD risk of 20% should be initiated if BP is above 140/90 mmHg. The British Hypertension Society recommendations (as described in Box 4) help identify an appropriate antihypertensive medication.
Initiation of antihypertensive medication in the primary care setting
If younger than 55 years: start an angiotensin-converting enzyme (ACE) inhibitor (or Angiotensin II receptor antagonist if intolerant)
If older than 55 years or black patients of any age: start a calcium channel blocker or thiazide diuretic
Combine ACE inhibitor (or Angiotensin II receptor antagonist) with a calcium channel blocker or thiazide diuretic
Combine ACE inhibitor (or Angiotensin II receptor antagonist) with a calcium channel blocker and thiazide diuretic
Add to Step 3 either another diuretic or alphablocker or beta-blocker
Also consider specialist referral
Medications should be initiated at the lowest recommended doses and titrated up to keep BP to less than 140/90 (or lower if the patient has diabetes and/or renal disease). The patient should also have a check up to look for end organ damage, such as a check for left ventricular hypertrophy on electrocardiogram (ECG) and urinalysis to look for any microalbuminuria.
Lipid-lowering medication
For asymptomatic patients at high risk for CVD, numerous studies have shown that statin therapy significantly reduces all-cause mortality and primary cardiovascular endpoints. Guidelines recommend high-risk patients be offered simvastatin 40 mg or pravastatin 40 mg once a day as a standard dose, irrespective of baseline lipid levels. This is something that is important to be clear about in communicating to patients as patients may be confused if offered a statin even though their total cholesterol level is low. Such scenarios might be worth rehearsing during communication skills workshops. Anion exchange resins, fibrates and nicotinic acid should not be offered for primary prevention.
Antiplatelet medication
Aspirin is an irreversible inhibitor of cyclo-oxygenase 1 (COX-1) resulting in reduced platelet activation and prevention in the formation of atherosclerotic plaques. The evidence for the use of aspirin in established CVD is overwhelming; however, its use in primary prevention is less convincing. Currently, SIGN, JBS-2 and European guidelines all recommend aspirin 75 mg daily for all people over the age of 50 years who have a total CVD risk less than or equal to 20% once the BP has been controlled to 150/90 mmHg.
However, a recent meta-analysis showed that aspirin use provided an absolute risk reduction in serious vascular events of just 0.06% per year, with an absolute risk increase of 0.03% per year for major bleeds (Baigent et al., 2009). Therefore, it is important to weigh the risks of treatment against the potential benefits for each patient before initiating aspirin for primary prevention of CVD. There is no evidence supporting the use of clopidogrel in primary prevention and it should not be initiated in the primary care setting for this indication.
Final words
The recommendations outlined in this article are based on the current evidence available at the time of writing. There still exists much controversy around best management in many key areas, such as the use of aspirin in primary prevention or the introduction of statins in individuals with a low absolute risk but high single risk factors. The goal of this article is to give clinicians a broad consensus approach to primary prevention of CVD in asymptomatic individuals. As new research comes to light, this should be evaluated, and if valid and applicable to the situation, incorporated into clinical practice.
Key points
Screening for CVD in the asymptomatic population should begin at the age of 40 years
Risk factors for CVD include non-modifiable factors such as age, sex and ethnicity and modifiable factors such as smoking, diet, exercise and hypertension
CVD risk assessment calculators can be used to quantify risk but need to be individualized depending on patient-specific criteria
Lifestyle modification and pharmacological treatment should be considered in asymptomatic individuals with a total risk of a cardiovascular event of greater than or equal to 20% over the next 10 years
Lifestyle modification requires a multi-disciplinary approach and includes modification in diet, exercise and smoking cessation and alcohol consumption
Pharmacological intervention should be discussed with patients and assessed individually and include antihypertensive medication, lipid-lowering drugs and antiplatelet treatment