
Abstract
Reducing health inequalities and improving access to primary care for the socially excluded is a Royal College of General Practitioners (RCGP) area of clinical priority for 2011–13. Asylum seekers are a key socially excluded group but primary health care professionals are under-resourced and lack confidence in managing this population because the UK asylum process is complex, asylum seekers present with an uncommon set of health care needs and cultural and communication barriers may exist. This article provides an overview of providing primary care for asylum seekers, an introduction to the legal process that asylum seekers must travel through and aims to equip readers with knowledge, skills and attitudes that may be helpful when providing care for this group.
The GP curriculum
This article directly relates to the
The learning outcomes with particular relevance include:
Treat colleagues, patients, carers and others equitably and with respect Act in ways that recognize that people are different and do not discriminate against people because of those differences Provide information in ways that help people to exercise their rights Recognize and take action to address discrimination and oppression in self and others Develop communication skills including working with interpreters to deal with patients from diverse backgrounds Recognize the importance of individual differences and social context to health, illness and health care when dealing with patients from ethnically diverse backgrounds Recognize the concepts of ethnicity and culture Recognize the concepts of diversity and equality and, in context, perspectives on migration, demography of cultural groups, experience of socio-economic disadvantage and patterns of illness and disease
Definitions
Asylum seekers are one of the most vulnerable groups in UK society. While they may suffer from many of the same health problems as the rest of the UK population, they come from diverse cultural, religious and social backgrounds and have some needs more specific to their experiences, past and present.
Health care workers should become familiar with the following definitions to aid understanding of the different stages of the asylum process (they will be used throughout this article).
In the UK, a person is officially given ‘refugee’ status when his or her claim for asylum has been accepted by the UK Border Agency (UKBA) An ‘asylum seeker’ is a person who has left his or her country of origin, has formally applied for asylum with the UKBA and is awaiting a decision on his or her application A ‘refused asylum seeker’ is a person whose asylum application has been unsuccessful A ‘destitute asylum seeker’ is a person whose asylum application has been refused and, due to lack of entitlement to any welfare support or the right to work, is unable to meet the basics of food and shelter
Global context
Claiming asylum is a universal Human Right as stated in Article 14 of the United Nations (UN) Declaration of Human Rights. Article 14 states that ‘everyone has the right to seek and to enjoy in other countries asylum from persecution’. This article was the pivotal point for the UN Convention relating to the Status of Refugees of 1951, which came to its 60th Anniversary in 2011. Curriculum statement 3.4 maintains GPs must understand ‘in context, perspectives on migration’.
Numbers of asylum applicants in the UK may be decreasing but globally, the number of refugees, internally displaced people (IDP) and asylum seekers are increasing. This global trend is primarily due to people moving to safety from a number of world conflict situations, basic resource shortages and climate catastrophes. Refugees, IDP and asylum seekers are distinct from economic migrants, who move countries solely to improve their financial position or prospect of employment.
The 2009 UN High Commission for Refugees (UNHCR) report documents 43.3 million forcibly displaced people around the world, the highest number since the mid 1990s. To make a comparison, the entire population of Spain is approximately 46.1 million (ine.es/) and Argentina, 40.0 million (censo2010.indec.gov.ar). With 1.7 million refugees, Pakistan at the time of writing hosts the largest number in the world (mainly Afghani refugees), Iran closely follows with 1.1 million and Syria with 1.05 million—the majority of these being Iraqi.
Asylum trends are determined by a host of rapidly changing factors in both the region of origin and the potential destinations. At the start of this millennium, the older European Union (EU) countries were receiving far fewer asylum applications than before and newer EU countries showed a steady small increase (Norredam, 2005). The provision of health care for asylum seekers across Europe was heterogeneous, often based on minimum EU standards, with almost half of the countries restricting access to emergency care only. Figure 1 summarises the number of asylum applicants in Europe in 2009 and shows the UK (in red) equalling the EU average.
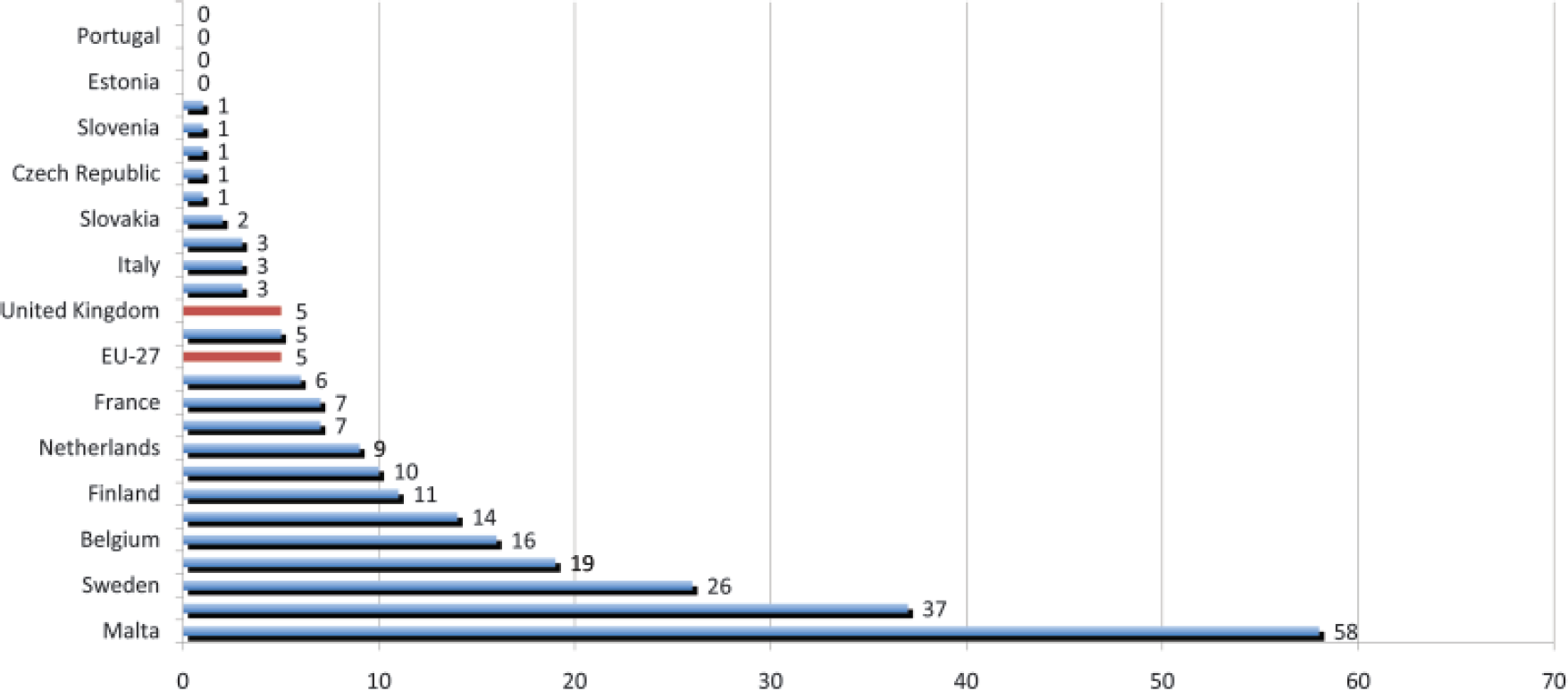
Asylum applications in 2009 per 10 000 population of receiving country.
UK situation
A number of barriers limit the engagement of frontline health care workers with the health care needs of asylum seekers in the UK. These include a lack of understanding of the UK and Global asylum legislation, the reasons for people seeking asylum, the impact the process can have on individuals and their families and the availability and entitlement asylum seekers have to various health care services. This disassociation can partly be explained by rapid and prohibitive legislative changes, inaccurate and inappropriate media reporting and lack of sustained funding to develop local or voluntary services, which may manifest as prejudice by frontline workers.
Longstanding tradition
The UK has been host to refugees for over 450 years, who often bring a wealth of knowledge and skills. For example, in the 17th century, Jews fled from Spain and Portugal introducing the now traditional ‘fish and chips’ to the UK, while the highly skilled French Protestant ‘Huguenots’ took sanctuary from Louis XIV bringing silk weaving, copper engraving and reintroducing market gardening. Every conflict of the 20th century has resulted in displaced people coming to the UK, no more so than after the Second World War. The Observer newspaper estimates 30 000 UK jobs have been created in Leicester by Ugandan Asian refugees since they immigrated in 1972. Many established communities in the UK came originally as refugees. Today, the number of asylum applications is steadily decreasing having peaked in 2002 at 84 130. Consequently, the number of refugees resident in the UK is on the decline (Fig. 2).
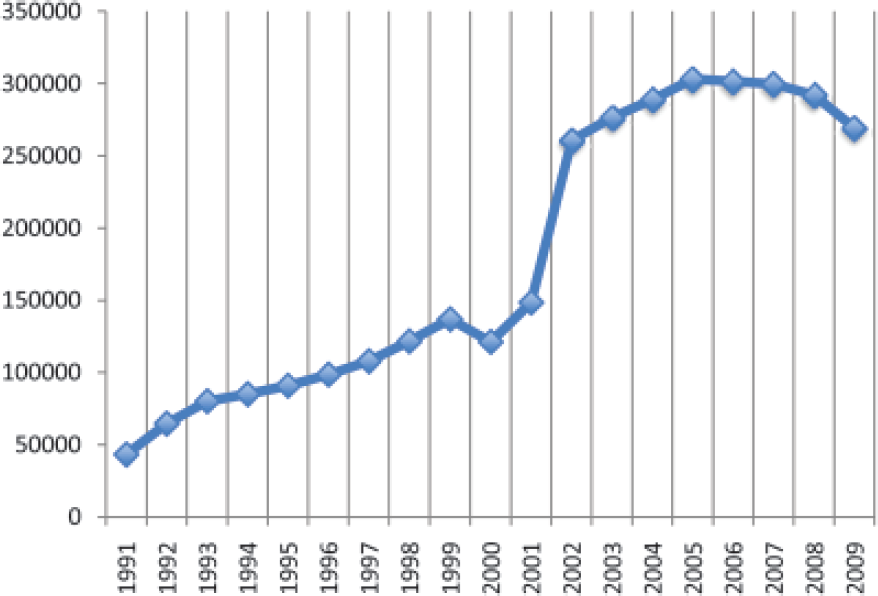
Total number of refugees resident in Britain (1991–2009).
However, UNHCR statistics show that there was not a significant drop in asylum applications worldwide and that UK trends are not mirrored internationally.
As with the asylum debate in general, the cause of this decline is much debated, highly political, multifactorial and without definitive answers. Contributing factors could be the 2002/2003 changes to the immigration rules making it more complex to get into the UK, the UK's collaboration with France to ‘protect’ the borders and manage migration across Europe. This was symbolized by closure of the Sangatte refugee camp in Calais in 2002 and subsequent destruction of its temporary replacement known as the Jungle in 2009.
The top 10 countries of origin for people claiming asylum in the UK also differs slightly from the international list. The most significant change between 2009 and 2010 was the 60% drop in applications from Afghanistan and the increase by 209% in applicants from Sudan fleeing the Darfur conflict (Table 1).
Top 10 countries seeking asylum in the UK quarter 3, 2010 compared with quarter 3, 2009

UK policy context
The UK asylum process (summarized in Fig. 3) has been subject to numerous changes since 1999. There have been new immigration bills practically every year, making the legal and administrative process of claiming asylum in the UK a complicated and dynamic process.

Summary of the UK asylum process.
In keeping with statement 3.4, it is essential for primary care staff to maintain a basic and clear understanding of the asylum process. The following sections illustrate the process that an asylum seeker will have to follow prior to presenting in primary care and so the context from which they seek care.
Arrival
In the UK, people in fear of persecution in their own country can approach the authorities to seek protection from the state and hence exercise their right under Article 14 of the UN Declaration of Human Rights. This can be done at the port of entry on arrival in the UK or alternatively ‘in country’ by approaching the UKBA (UKBR) offices in Lunar House in Croydon. According to UK law, this must be done as soon as practically possible and failing to do so may result in detention of the person or the refusal of asylum support (accommodation and support provided by the UKBA).
Screening interview
A screening interview is conducted at the time of claiming asylum in order to establish the background of applicants, their country of origin, their route of entry into the UK and a broad explanation of why they fear returning to their home country. Asylum seekers may then be given temporary admission into the UK and the option of obtaining financial support and accommodation (‘Section 98’ support), usually in hostels dispersed around the UK for a period of 2–6 weeks. During this time, all applicants are required to submit an application for asylum support (Section 95) and will also be allocated a ‘case owner’ who will conduct a substantive interview and be responsible for making a decision on their asylum application and following the case to ‘conclusion’ (either until leave is granted or the applicant is removed from the UK).
Those not granted temporary admission will be detained and entered into the ‘fast-track’ system, which aims to conclude applications quickly (this is usually people from a country deemed ‘safe’ by the UK and should not include vulnerable groups such as pregnant women and victims of torture). Interpreters must always be used if required, but in the majority of cases access to a legal representation is not provided.
Dispersal
Once the asylum support application is processed, the applicant is dispersed and settled in temporary hostel accommodation. Asylum support accommodation is provided on a no-choice basis. Accommodation and financial support is provided during the time that the asylum claim is being processed. Applicants who have children at the point of claiming asylum, or while the asylum claim is pending, continue to receive financial support and accommodation even if their claims are refused. This support should continue until the family either leaves the country or is granted ‘leave’ to remain in the UK for a specified time period.
The case owner makes the asylum application decision generally within days of the substantive interview. If the claim is accepted, the applicant is then granted ‘Refugee Status’ (5 years limited leave), ‘Humanitarian Protection’ (5 years limited leave) or ‘Discretionary Leave’ (time scales may vary). If the claim is refused, the applicant will have the right of appeal at the First Tier Tribunal (formerly known as the Asylum and Immigration Tribunal). Applicants are financially supported through this process under ‘Section 95’ unless one of these appeals was made out of time.
End of process
At the point of refusal, the UKBA has developed a ‘hard case’ alternative which is known as Section 4 support. Section 4 support provides accommodation and £35 worth of vouchers to be used in different shops around the UK. In order to qualify for Section 4 support, applicants must firstly prove that they are ‘destitute’ and secondly that they fall into one of the following categories:
The applicant is taking all reasonable steps to leave the UK voluntarily or placing him or herself in a position to do so. The applicant is unable to leave the UK by reason of physical impediment to travel or for some other medical reason The applicant is unable to leave the UK because in the opinion of the Secretary of State, there is currently no viable route of return available The applicant has made an application for Judicial Review of a decision in relation to his or her asylum claim The applicant requires support in order to avoid a breach of a person's rights under the European Convention on Human Rights (ECHR).
Destitution
This type of support is by nature meant to be a temporary measure, although in reality, many applicants are supported via the voucher system for periods of longer than 18 months. If Section 4 support is refused, asylum seekers rely on handouts from friends, family, churches and charities or survive by working illegally and hence are at risk of exploitation. In this scenario, they become defined as a ‘destitute asylum seeker’. Different refugee support agencies around the country provide independent advice on asylum support and offer other types of advice to asylum seekers in need. They can submit the asylum support forms and can direct people to their entitlements and advocate on their behalf.
Health screening
The UK provides health screening for all those who claim asylum and are willing to take part. Screening consists of a general medical consultation that is usually carried out by a specialist nurse in the Initial Accommodation Centre. A health record is then opened and routine checks such as the tuberculosis (TB) Mantoux test are carried out. Access to GPs and other doctors should be made available and a certificate (HC2) should be issued by the UKBA.
The HC2 entitles asylum seekers to free prescriptions, eye-care, dental care and other health-related costs for 6 months and needs to be renewed thereafter.
Entitlements to health care
As shown in Table 2, current entitlement to National Health Service (NHS) health care is dependent upon the stage of the Asylum process. In January 2010, failed asylum seekers, denied access to health care or charged £1000 for care already received, legally challenged the existing legislation. They argued that it was a breach of human rights not to provide health care to people in need who did not have the means to support themselves while in the UK. In March 2011, responding to the subsequent ‘Review of Access to the NHS by Foreign Nationals’, the Department for Health made significant changes to the entitlements system for implementation by June 2011. Destitute asylum seekers (on Section 4 support) are now exempt from secondary care charges, whereas refused asylum seekers are charged for secondary care and charged for immediate care after the fact.
Entitlements to NHS primary and secondary care

Health needs of asylum seekers
The GP curriculum emphasizes ‘the importance of individual differences and social context to health, illness and health care when dealing with patients from ethnically diverse backgrounds’. Health needs of asylum seekers are summarized in Box 1.
Health needs of asylum seekers
TB Hepatitis Human immunodeficiency virus (HIV)
Direct trauma Secondary effects of torture Post-traumatic stress disorder (PTSD) Malnutrition Rape and sexual assault
Anxiety Depression Grief and loss Disorientation Suicidal thoughts
Physical health
There are likely to be higher levels of communicable disease among asylum seekers, which will vary according to country of origin [for example high rates of exposure to human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) in Sub-Saharan Africa]. This may be exacerbated by coming from a country where the health system is poorly organized, lacks funding or has even collapsed, with patients less likely to have been immunized, diagnosed or to have received treatment for common conditions.
Correspondingly, many chronic diseases such as hypertension and diabetes may not have been diagnosed or treated, leading to late presentation of complications related to advanced disease and consequently to poorer health outcomes. People who have come from long stays in overcrowded refugee camps where sanitation is poor are also more likely to have picked up communicable diseases, such as TB, and are made more vulnerable through malnutrition. Malnutrition, poor sanitation, overcrowding and extremes of temperature are also likely to occur on long and dangerous journeys to reach the UK often exacerbating existing health problems and making injury and spread of disease more likely.
Many will have sustained injury as a result of torture, sexual violence, war or imprisonment in their country of origin, may not have received any treatment for these injuries and will have little to no access to disability support services. Such injuries include fractures, scars from burns/beatings, head injuries, dental problems and loss of hearing or vision. Sexual violence and rape are also used as a tool of war and torture with the resulting mental and physical health problems including HIV and other sexually transmitted disease and unwanted pregnancy and its complications.
Mental health
The majority of asylum seekers experience mental health difficulties as they are going through the asylum process in the UK and this features prominently in the literature as an unmet health need. There are many reasons why asylum seekers have high levels of stress, anxiety, poor sleep patterns and other mental health problems:
Stress of leaving their country of origin, family, friends and community Associated loss of status, personal identity and employment Difficult conditions on their lengthy journey to the UK Horrific events (either directly experienced or witnessed) as a result of war or oppressive regimes. It is estimated that the prevalence of torture amongst asylum seekers is 5-30% depending on their country of origin.
It follows that mental health features in asylum seekers often present differently, more severely and with high levels of somatization when compared to the general population. This may be due to different notions of what constitutes mental illness in the country of origin, through the cultural stigma of mental illness, or by not having knowledge of the English words to express distress. Some may be fearful of expressing their difficulties because they fear being deported if found to have a mental illness or due to fear of retribution if they talk about what has happened to them.
Symptoms of PTSD can be overlooked and the disorder underdiagnosed, especially in children, as distressing dreams, jumpiness, low mood and poor sleep patterns can be wrongly assumed to be a common and normal response to torture. Levels of anxiety and depression are thus high on arrival and may be compounded by the realities of adjusting to life in the UK—social isolation, learning a new language and adapting to a different culture, racism and hostility from the local population.
The complete disorientation which must come from suddenly arriving in a new country and the rigours of going through the asylum system contribute to the reasons why mental health in particular may deteriorate during the first 2–3 years after arriving in the UK. The negative image frequently portrayed by the UK media does little to improve matters. Most asylum seekers have no choice as to where they are placed to live and are unable to work resulting in poverty and loss of skills and abilities, compounding isolation and mental health problems. It is not surprising that asylum seekers are one of the highest risk groups for suicide.
Children, adolescents and unaccompanied minors
Children will have had similar experiences to adults but it may impact on them differently, for example causing behavioural problems and bedwetting, or malnutrition impacting on child development. They may also be less able to talk about their difficulties or find the right words to express themselves. Unaccompanied minors are particularly prone to social isolation and are a very vulnerable group from a mental health point of view.
Women's health needs
There is lower uptake of contraceptive services, cervical screening and breast screening amongst asylum seekers, presumably due in part to frequently moving address and not receiving reminders. There are poor outcomes for pregnant asylum seekers—they are seven times more likely to develop complications during childbirth and three times more likely to die than pregnant women in the general UK population. This may be due to a lack of access to antenatal care and poor nutrition. Awareness of practices such as female genital mutilation is important to consider although not specific to asylum seekers; the resulting menstrual, sexual health and childbirth problems that arise from this may be severe.
Failed asylum seekers and destitution
Destitute asylum seekers represent a particularly vulnerable group with high levels of physical and mental ill health. They are much less able to access regular medical and dental care due to being homeless and moving around frequently. This homelessness and transience prevents them building up stable relationships and, together with the effects of feeling accused of lying in their asylum claim, has a significant impact on their mental health. The fear of being deported and of returning to their home country may exacerbate PTSD. Living in poverty results in lack of food, malnutrition and potentially unsafe housing. This results in worse physical and mental health outcomes. Failed asylum seekers are also more likely to be exploited. For example, they may be forced into domestic servitude, prostitution or unregulated work to obtain accommodation, money or forms.
Ensuring health care access
Having already faced the loss of leaving their home country and sometimes the rejection of their UK asylum claim, many asylum seekers choose not to access health care for fear of further rejection and of being charged for consultation or treatment. It is vital that their formative experience of the NHS is positive enough to retain this vulnerable population to follow-up.
As for any risk factor for any disease, the effect of these potential barriers can be reduced if the primary care team is knowledgeable and aware, skilled in eliciting the relevant clinical and social information and equipped and proficient in using the clinical tools available to address and overcome them. The services an asylum seeker must have access to in order to be able to ‘exercise their rights’ in accordance to statement 3.4 and to benefit fully from the UK health system are thought to be
Access to primary care with full and permanent registration Information about health services Appropriate and comprehensive health assessments including physical and mental health Adequate access to translation, interpreting and advocacy services in appropriate languages Adequate and appropriate responses to mental health problems Access to specialist services for survivors of torture and organized violence Advice and information on health promotion
Language
In any situation where a patient can speak only minimal English, it is the clinician's ethical responsibility to ensure that all important clinical information is gathered accurately, that the clinician is understood and that key health care decisions are relayed back to the patient successfully. This is the case for issues of informed consent as well as implied consent, which only has validity if the patient genuinely knows and understands what is being proposed.
The curriculum statement states that GPs must ‘develop communication skills including working with interpreters to deal with patients from diverse backgrounds’. The general practice consultation relies heavily on effective communication and consequently, much GP registrar training focuses on developing higher consultation skills. Without knowledge or proficiency in speaking the myriad of languages spoken by asylum seekers, a clear communication barrier is created. In situations where prior warning is made or if the patient is already known to your primary care service, it is often possible to organize for an interpreter to be present.
A benefit to using unknown interpreters over family members is to avoid misinterpretation, but they can also avoid the stigma attached to mental illness in some cultures and the shame of sharing experiences of a sensitive nature such as torture and sexual violence. In these situations, the use of family and friends is not advised. Working with interpreters is a skill in itself and when using an interpreter, it may be helpful to keep the suggestions in Box 2 in mind.
In situations where patients may wish to disclose issues of sexual violence, domestic abuse and problems of a sexual nature, they may prefer the anonymity of a faceless telephone interpreter. The timing of such disclosures is incredibly unpredictable and so faceless telephone interpretation is regarded by some as a necessity in all cases. There are two immediately accessible telephone interpreting services in the UK, with contracts with a large number of Primary Care Trusts. These are not only available to clinicians but also to government agencies, to big business and to the consumer.
Experience, however, of the use of telephone interpretation in the clinical setting is mixed with criticisms such as ‘difficult to use’, ‘prohibitively expensive’, ‘inconvenient’ and ‘overly time-consuming in an already time stretched consultation’ (Ray, 2010). GPs with wider experience of using telephone interpretation services argue that ‘with a hands-free telephone and a bit of practice (a telephone interpretation service) is actually easy to use, and the instant access to an interpreter vastly makes up for not having a person in the room’. For clinicians who use telephone interpretation service frequently, a dual handset phone designed so that the clinician and patient can listen and talk simultaneously may be helpful.
Case study to highlight factors to consider when using an interpreter.
Mrs B is an Iraqi asylum seeker. A colleague has booked her an appointment to see you in 2 days after seeing her out-of-hours. His note says that Mrs B seemed anxious and unsettled and that it was difficult to ascertain fully the presenting complaint as she kept slipping between English and another language he could not understand. He also mentions she is receiving Section 4 support.
Allow enough time, e.g. to book a double appointment slot Ask in advance if you may book an interpreter and whether the patient has a preference regarding the interpreter's gender Spend a few minutes with the interpreter before the session to outline the purpose of the meeting
Maintain eye contact with the patient Talk directly to the patient (do not speak in the third person) Understand patients may choose to speak English to psychologically distance themselves from the traumatic experience Patients usually comfortable using English may slip into using their first language when distressed
Spend a few minutes with the interpreter at the end of the session for a short debriefing Where possible, try and use the same interpreter for subsequent appointments
It is essential to appreciate that telephone interpretation services have become a key clinical tool to ensure patient safety. Proficiency in telephone interpretation is a mandatory skill for any practising GP committed to ensuring good quality patient care.
Cultural differences
Statement 3.4 reads ‘recognize the concepts of ethnicity and culture’ yet despite health professionals' best efforts to ensure effective communication, further cultural barriers may exist which prohibit the exchange of vital information. For example, some practitioners have found that prior education to familiarize the patient with the western model of mental health is beneficial before patients can successfully engage with mental health services (Ashton and Moore, 2009).
When, for example, an asylum seeker becomes unwell, the NHS appointments-based system may not be familiar to someone coming from a different health system. Turning up and expecting to be seen immediately upon arrival, or outside appointment times, may not be perceived as inappropriate or problematic. This situation managed insensitively may prevent future attempts to access care. There is a clear opportunity to ensure quality care is accessed and that clear information about the NHS and the UK health system is shared, which will instead improve future attempts to access care.
To prevent misperceptions from standing in the way of good quality care, there is a need for ongoing training in cultural, religious and gender sensitivity: factors increasingly included in medical training and that require regular updates for the primary care team as a whole.
Specialist and allied organizations
The contribution of local voluntary agencies to the health needs of asylum seekers is unique and flexible in comparison to mainstream NHS services, as is their ability to respond more swiftly to the local social context. It is essential to understand the services and advocacy they provide in your locality and for this to feed into the health care you provide. New health problems may be picked up in the community before they present in practice, allowing vital preparation.
Acting as a bridge between voluntary and health sector are advocacy workers and some authors have suggested investment in advocacy workers to be more efficient than providing a greater number of health care staff. One suggestion has been that upon registration, all newly arrived asylum seekers are provided with practical information regarding the location of other health care settings such as hospitals, dentists and voluntary agencies.
Wider determinants
Johnson (2003), in a report for the Home Office, described that the presence of asylum seekers highlighted existing gaps in health care provision rather than creating new problems and that these health system failures were the main barrier to the effective and efficient delivery of health care services to asylum seekers. Solutions to the systemic health inequalities faced by asylum seekers must be developed through broad social, political and economicaction to promote social integration through education, employment and through building supportive social networks of asylum seekers and health and allied professionals.
Gaining and maintaining experience
Very few asylum seekers are registered with some general practices and patients moving around during application and settlement threatens continuity of care. As a trainee, it can be difficult then to gain clinical experience and to maintain essential clinical skills once qualified. However, in keeping with the core principles of statement 3.4, asylum seekers accessing care in an area with few other asylum seekers deserve an equal standard of care to those attending a high volume practice.
To gain valuable experience, you could organize to visit the temporary hostels and specialist GP services in your region, arrange a tutorial with your mentor discussing care for this group, organize a practice meeting to update your colleagues on the relevant services in your area, arrange a half-day release programme to involve practical experience through using translation services and simulated patients or invite specialist GPs and groups such as Refugee Council, Medact, Refugee Action or Medecins Sans Frontières to share their experiences.
Key points
Asylum seekers are a heterogeneous group The complex UK asylum process can lead to poor health outcomes if misunderstood There are a range of barriers to health care access Asylum seekers are high risk for mental health problems, infant/maternal mortality and HIV/TB Use of interpreting services is essential and should be regarded a mandatory clinical skill Find out about your local voluntary sector organizations or specialist NHS services and use them