
Abstract

Last July I travelled to Trento, in Northern Italy, to participate in a Hippokrates exchange. The Hippokrates exchange programme, was launched in 2000 and aims to encourage the mobility and sharing of knowledge among young doctors across Europe. Participants either visit another European country for a 2 week exchange or host an exchange participant. The Royal College of General Practitioners (RCGP) Junior International Committee has been able to secure funding for a limited number of exchanges each year through the European Commission's Lifelong Learning Programme, so-called Leonardo grants. I was awarded a Leonardo grant to fund my exchange.
During my time in Trento, I spent each day observing different GPs at work, in both the urban and the rural setting. I also spent time with the out-of-hours service and community palliative care teams and attended university teaching with my Italian peers. This report aims to provide a summary of the main differences and similarities between UK and Italian primary care training and practice. It is based upon my experiences and observations while in Italy and the conversations I had with Italian GP s, trainees and citizens.
GP training
Although the European Community regulations for vocational training for general practice were established in 1986, formal recognition and implementation of a programme were only introduced in Trento in 1992. Prior to this, Italian GPs worked largely unsupervised following their graduation from medical school.
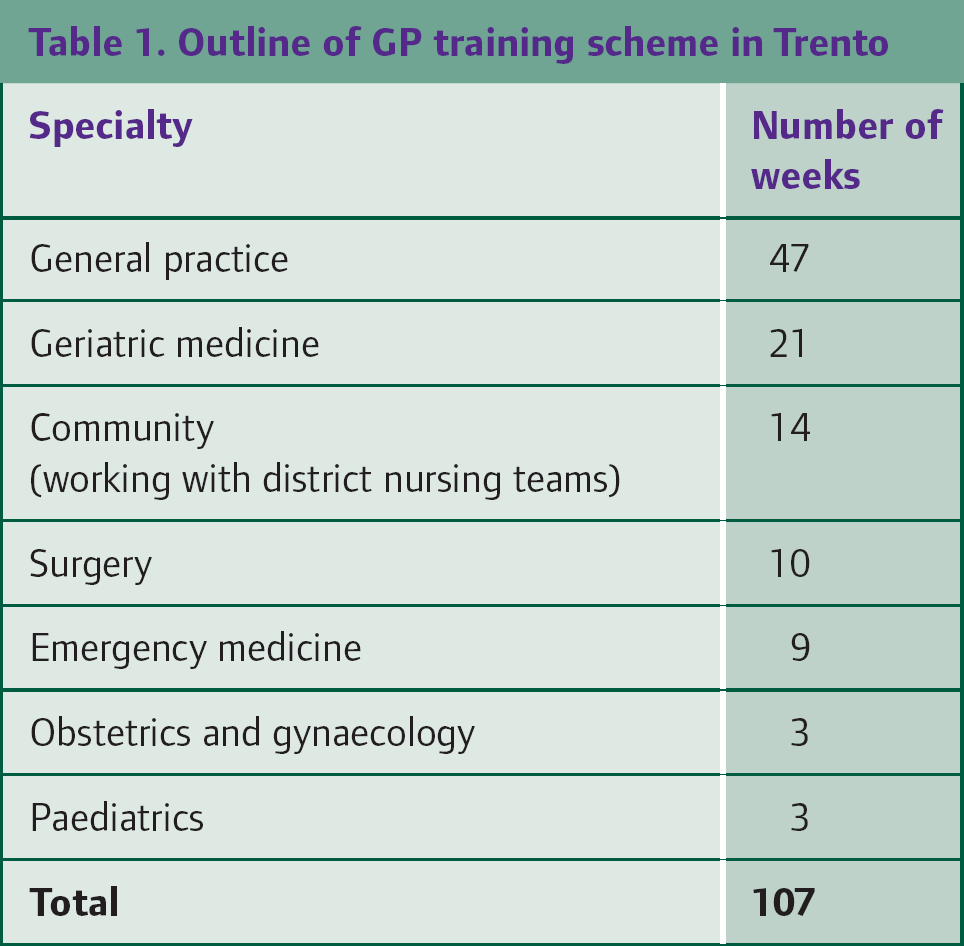
Some aspects of Italian and UK training are comparable. In Italy, potential trainees must sit an entry multiple choice question (MCQ) exam and, as in the UK, those who are accepted for training follow a 3 year programme. Italian trainees are also assigned a GP tutor at the beginning of their training. However, in Italy each trainee completes ‘exactly’ the same rotation (Table 1). The programme also has more of an emphasis on general practice and far less, compared to the UK, on specialty subjects.
Outline of GP training scheme in Trento
During the exchange, I attended some of the teaching sessions for Italian trainees, including lectures by local hospital consultants. The teaching delivered was rather didactic, with an emphasis on theory and volume of knowledge. In contrast, the UK approach relies more heavily on peer-led teaching and problem-based learning. Although simulated patients and role play are widely used in the UK, this teaching method is very much in its infancy in Italy; Trento is unique in having local GPs who are driving the concept forward.
I went out for dinner with one trainee to learn more about her experience of training. She told me that GP trainees are viewed as doctors but not ‘working doctors’. In hospital, the typical day is unstructured; trainees are able to decide what they do. This has advantages, as individuals can choose to observe the care of the more ‘interesting’ patients. However, this approach to learning concerned many trainees; the lack of opportunity to experience working in a team or apply their clinical knowledge left them feeling under-confident in practical skills and clinical decision making.
In primary care, trainees spend the majority of their working week observing the consultations of their GP tutor, with time for discussion between cases. The tutor also observes them carrying out consultations but only two per day. The trainees I spoke to were shocked to learn that at the equivalent stage of training, I consult with patients independently. This apparent lack of autonomy in day-to-day training is at odds with the fact that Italian trainees practise independently before qualification and in the out-of-hours setting.
Financial issues
Another difference between the UK and Italian GP training schemes relates to working hours and remuneration. Italian trainees work an average of 30 hours a week, usually averaging 6 hours a day (although hours seem flexible). For this, they are paid approximately € 850/month (£748 based upon current conversion rates). UK trainees are contracted to work 40 hours/week (excluding additional compulsory out-of-hours shifts) and get paid around £2500/month after tax. Earning three times as much as my Italian counterparts astounded me. What shocked me further was learning that Italian hospital-based junior doctors are paid double that of their primary care colleagues.
I feel this may reflect the lower status of general practice in Italy. A major advantage in terms of work-life balance, however, is that Italian GP trainees get a guaranteed 8 weeks holiday/year, allowing them to develop hobbies or do out-of-hours work to earn some extra cash.
The newly qualified GP
Italian trainees must sit an exam each year to qualify. These exams are free. Once qualified, Italian GPs are recruited and ranked on a centralized government points list based upon years post qualification, experience and exam grades. They are offered a job through the local government when one becomes available. Talking to both experienced GPs and trainees, it can take years be offered a job following qualification and during this time, individuals have no choice but to work the unsociable out-of-hours system to earn money.
GP partnership and collaborative working is relatively nonexistent in Italy. Although groups of GPs often operate out of the same building, all work as single-handed practitioners. They are paid according to individual list size; payment is € 40 per patient per year and the list size is capped at 1500 patients. It can be a struggle to survive at first and can take 7 years to gain a reputable list size. Many newly qualified GPs are forced to work additional anti-social hours with the out-of-hours service to survive. Some doctors simply do not succeed in attracting a viable amount of patients and abandon general practice all together.

Life of the Italian GP
Italy's health care system is a regionally based national health service that provides universal coverage at the point of service. Because of its devolved structure and organization, there is variability in the quality of health care among regions, representing a future challenge for Italy.
The work environment also differs from the UK. For example, many choose to manage their own administrative work rather than take a cut in salary by employing a secretary; it is not at all unusual for Italian GPs to answer the telephone at least two to three times during a face-to-face consultation. I was full of admiration for their ability to stay totally relaxed while consulting, answering the phone, typing a letter, arranging a repeat script by email and translating for me where appropriate. This practice seemed chaotic; yet, the GPs I met seemed more than competent in the art of multitasking!
In the UK, we work in a boundaried environment, with set appointment times and an accepted culture that we must not be interrupted except for emergencies. On one level, I value this and the message it conveys to the patient about the importance of our time. However, I also find myself indoctrinated to work to deadlines and targets; I would like to adopt a little of the Italian GP's ability to be flexible and adaptable.
Philosophy and values
One Italian GP I spoke to described being driven by patient satisfaction, not financial gain. This is reflected in the development of strong, caring relationships with patients, many of who will remain with that doctor for years. UK GPs also develop lasting relationships with patients and are encouraged to develop a whole-person approach; yet, I worry that this may be put at risk by the increasingly prescriptive nature of target-driven care. For example, anxiety about recording the Patient Health Questionnaire (PHQ9) score so that we are awarded our Quality and Outcomes Framework (QOF) points may detract from the more holistic care of our patients. The autonomy enjoyed by Italian GPs, free from top – down regulation and the pressure to deliver on results, may be beneficial. However, the QOF was introduced to reduce variability in the care received by patients, and it has been successful in that respect. While we may learn from our Italian counterparts in keeping a patient focus, they may also take something from us to reduce the problems they face with variable quality in health care.
All Associates-in-Training (AiTs) and those within 5 years of training are able to take part in the Hippokrates exchange programme. From my experience, it is highly recommended. It has broadened my perspective of general practice, opened doors of opportunity and, most importantly, enabled me to make some wonderful friends for life.