
Abstract
Osteoporosis is a condition in which the bone matrix is compromised, leading to thin, fragile bones that fracture easily. It has a significant socio-economic impact, both from the cost of treating such fractures and for the individual going through what is often a traumatic experience with a lengthy recovery. Therefore, as clinicians our focus should be on the early identification of disease and instigation of treatment. This article focuses on the diagnosis and management of osteoporosis, summarizing current guidance along with providing practical tips on how to manage affected patients in our consultation rooms.
The GP curriculum and osteoporosis
Osteoporosis is covered by
Appreciate the epidemiology, aetiology and natural history of musculoskeletal disorders Manage the primary contact with patients who have a musculoskeletal problem Describe when blood tests and imaging methods are required for diagnosis, how to interpret them and how they influence management Understand the principles of treatment for common musculoskeletal disorders managed largely in primary care Communicate health information effectively to promote better outcomes Describe the key national guidelines that influence healthcare provision for musculoskeletal problems
With an ageing population, osteoporosis is becoming an increasingly important public health issue. It accounts for over 200 000 fractures each year in the UK (National Osteoporosis Guideline Group (NOGG), 2010), with approximately a third of women and one in five men suffering an osteoporotic fracture in their lifetime. Hip fractures are the most serious complication of osteoporosis, carrying a high rate of disability and mortality. The mortality rate within 12 months of a hip fracture is in the order of 20–30% (NOGG, 2010). The primary care team plays a vital role in the early identification of individuals at risk of osteoporosis. Furthermore, initial diagnosis and treatment of osteoporosis is often commenced in primary care.
Pathophysiology
Osteoporosis is ‘a generalised bone disease characterised by decreased bone mass and a deterioration of bone micro-architecture'(World Health Organisation (WHO), 1994). Normal bone is composed of several cell types: osteoblasts, which are responsible for formation and mineralization of bone; and osteoclasts, which are involved in bone resorption. The combination of these processes results in bone modelling and remodelling. Peak bone mass is the bone mass achieved at the end of an individual's growth period through bone modelling and remodelling. It is an important factor in determining the future risk of osteoporotic fractures. Peak bone mass is achieved at approximately 30 years of age, after which bone loss begins and continues throughout life. In women, the rate of loss accelerates after the menopause, and thus early menopause is a significant risk factor for developing osteoporosis. As age increases other factors, such as immobility or vitamin D deficiency, play a role in continued bone loss in both women and men.
Diagnosis
Osteoporosis is often diagnosed after the occurrence of a ‘fragility’ fracture. Fragility or ‘low impact’ fractures are those that occur after falls from standing height or lower. Commonly affected sites are the hip (proximal femur), wrist (distal radius), proximal humerus and vertebral column. The cause of these fractures is not only the low density of bone that occurs in osteoporosis but also factors that may predispose to falls. This is important to remember when assessing patients, particularly when considering their risk of a further fracture.
In the absence of fragility fractures, osteoporosis tends to be diagnosed after measuring bone mineral density (BMD) with dual-energy X-ray absorptiometry (DEXA) in individuals who are suspected to be at risk. Two scores are used to quantify BMD: ‘T’ scores and ‘Z’ scores. The ‘T-score’ is the number of standard deviations the patient's BMD value is above or below the mean ‘standard’ BMD. The standard refers to a normal 30-year-old subject. This score can be used to determine whether an individual has osteoporosis (Box 1).
WHO definitions for osteoporosis and osteopenia
These definitions are applicable to perimenopausal and postmenopausal women, and men above the age of 50.
The ‘Z-score’ is the number of standard deviations the patient's BMD is above or below the mean value for age-matched normal subjects. It therefore indicates whether patients’ bone mass is appropriate for their age. Unlike T scores, Z scores cannot be used to diagnose osteoporosis. However, they can be useful in assessing risk of developing osteoporosis, particularly in younger patients.
Clinical assessment
A comprehensive history and physical examination is important in identifying risk factors for fracture, assessing for complications of osteoporosis and identifying secondary causes. Therefore, the history should include questions about family history of osteoporosis or hip fractures, lifestyle (e.g. alcohol consumption and smoking), relevant medical history, changes in height, previous fractures, menstrual and medication history. Any risk factors for falls should also be considered.
Risk factors for osteoporosis can be categorized into primary and secondary causes (Table 1). Secondary causes tend to be more relevant in the diagnosis of osteoporosis in men or younger women. Some risk factors act independently of BMD to increase fracture risk. For example, a history of a previous fragility fracture is a sensitive-independent predictor of future fractures, approximately doubling the risk (NOGG, 2010). A family history (maternal, paternal or sister) of osteoporosis or hip fracture is another example of an independent risk factor. Other risk factors increase fracture risk through their association with a low BMD, for example, smoking, alcohol and glucocorticoid use.
Established risk factors for osteoporosis

Examination should include height and weight measurements. A loss of 2 inches (5 cm) in height is a sensitive indicator for vertebral compression. The spine should be examined for alignment and spinal tenderness, which may indicate the presence of previous vertebral fractures. It is important to note significant thoracic kyphosis, as this could cause respiratory compromise. General examination may also reveal secondary causes for osteoporosis, as well as neuromuscular dysfunction, which may increase the risk of falls.
Case-finding
There is no universally accepted policy for population screening, or on opportunistic case-finding. However, recent recommendations (NICE, 2012) provide guidance on the groups of patients to target to identify those with a high risk of fracture (Box 2). Utilization of fracture risk-assessment tools in these patients can then guide management decisions.
NICE recommendations on targeting risk assessment
An assessment of fracture risk should be considered in women who are aged 65 years and over and men of 75 years and over A fracture risk assessment should be considered if the following risk factors are present amongst women younger than 65 years or men younger than 75 years:
There has been a previous fragility fracture There is a family history of hip fracture The patient has a history of falls The patient is using oral glucocorticoids or has frequently used them in the past The patient has a potential secondary cause of osteoporosis (e.g. coeliac disease) Low BMI (less than 18.5 kg/m2) The patient is a smoker of more than 10 cigarettes per day or drinks more than four units of alcohol per day Patients who are under 50 years are unlikely to be at high risk, thus a fracture risk assessment is not routinely required. However, it should be considered if major risk factors are present (e.g. current or regular oral glucocorticoid use, or untreated premature menopause).
The WHO has developed a fracture risk-assessment tool (FRAX), which is validated for use in both men and women between the ages of 40–90. The tool can be accessed online (see further information) and requires the submission of patient information that relates to risk factors for osteoporosis (mentioned in Box 2) and BMD, where available. Through this, the tool can calculate an individual's 10-year probability for a hip or other major osteoporotic fracture, helping clinicians make a decision whether treatment is required. In cases where a BMD value is not available, this tool also helps identify those who may benefit from additional investigation with a DEXA scan before commencing treatment.
There are limitations to the FRAX algorithm, including the exclusion of falls as a clinical risk factor, lack of clarity about what constitutes a significant dose of oral glucocorticoid and exclusion of spinal BMD measurements. Thus, clinical judgement is still required when interpreting the results to aid treatment decisions for individual patients.
An alternative tool for fracture risk assessment is QFracture, which is also available online (see further information). This also calculates the 10-year risk of hip and osteoporotic fracture, but it has several differences to FRAX. QFracture was developed and validated on a large representative primary-care population in the UK and thus is specifically designed for use in this population. It is suitable for ages 30–85, includes a detailed assessment of smoking and alcohol intake and incorporates additional risk factors not included in FRAX. The authors of the original study hypothesized that the inclusion of these more detailed variables would result in better estimation of an individual patient's risk (Hippisley-Cox and Coupland, 2009). However, there has been no head-to-head comparison of the two tools. One of the main limitations of QFracture is that it does not incorporate BMD measurements, unlike FRAX.
Laboratory investigations
Laboratory investigations are important in screening for secondary causes. The minimum tests that should be performed are summarized in Box 3. If clinical history or examination is suggestive, other investigations (e.g. blood tests to screen for coeliac disease) should be considered.
Relevant blood tests
Full blood count, erythrocyte sedimentation rate and serum/urine electrophoresis to exclude myeloma Liver and renal function; may influence treatment choice Serum vitamin D Serum calcium and phosphate; may detect hypercalcaemia associated with malignancy or hyperparathyroidism Parathyroid hormone (PTH) - if hyper/hypoparathyroidism is suspected Alkaline phosphatase; may be elevated in severe osteomalacia, malignancy, or Paget's disease Thyroid function Testosterone: consider in younger men with low BMD Follicle-stimulating hormone, luteinizing hormone: if concerns of hypogonadism Coeliac screen in suspected cases
Imaging
Plain X-rays are inaccurate in assessing BMD; bone loss must be greater than 40% before it is visible on X-ray. However, plain radiographs are useful if vertebral fracture or metastases are suspected. Bone scans and magnetic resonance imaging (MRI) are generally reserved for when there is suspicion of other causes of fracture, especially malignancy.
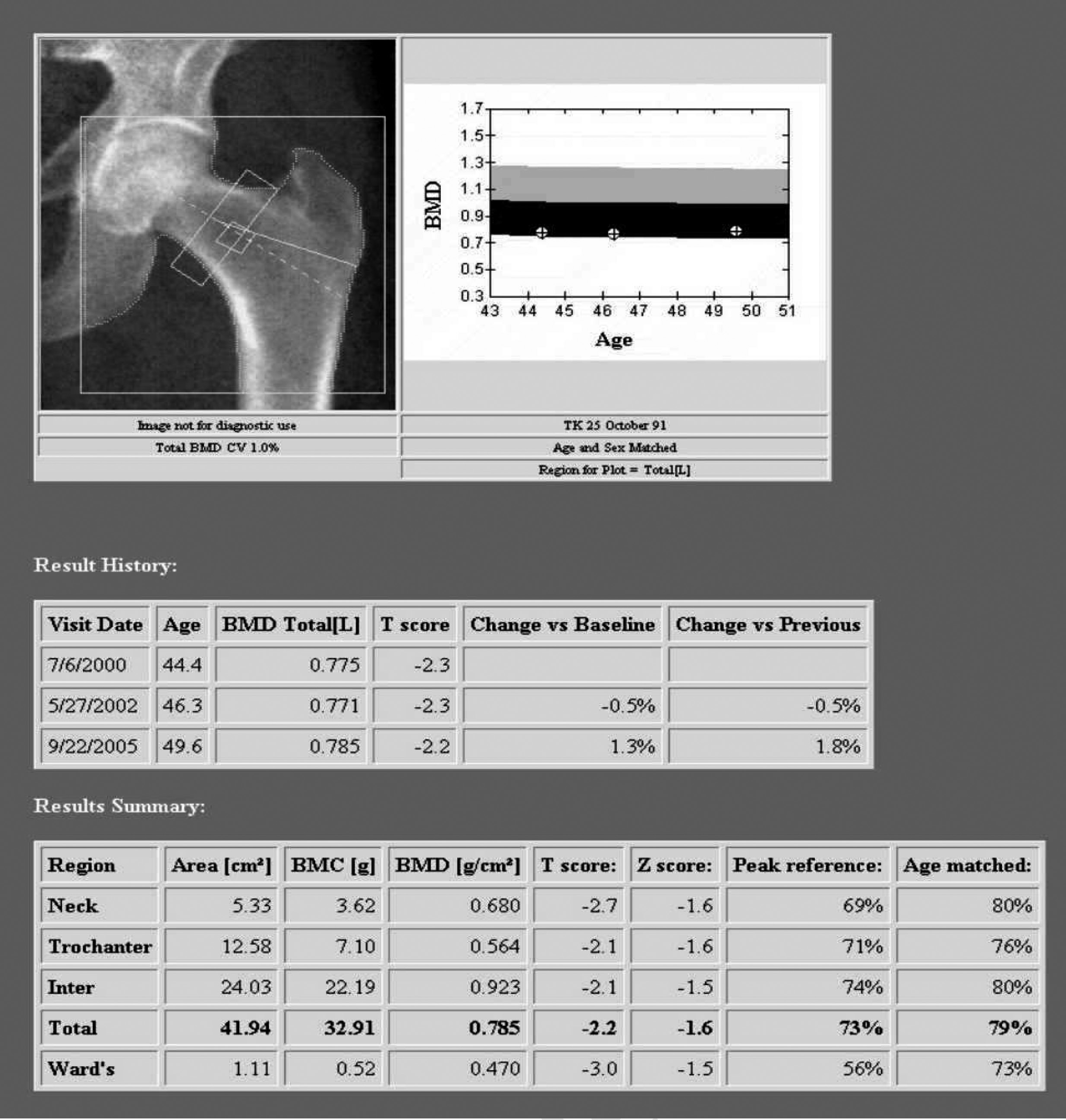
DEXA is the most widely used method for measuring bone density. It is fast, reliable and relatively safe, and is the gold standard in the diagnosis of osteoporosis. DEXA can be used to measure bone mass at both peripheral (e.g. heel, radius, hands) and central sites. Central DEXA measurements of the spine and hip are superior to peripheral sites as they provide a better prediction of future fracture risk. The DEXA report shows the BMD reported as an absolute value in grams per square centimetre (Fig. 1). Measurement at multiple sites increases sensitivity. This is why it is common for the report to include measurements of the spine for L1 to L4 vertebrae and the total spinal BMD (Fig. 2).
A DEXA report showing osteopenia at the hip with a total T-score of −2.8.

A typical DEXA scan report showing osteoporosis of the spine, with a total T-score of −2.2.
BMD is reported as T and Z scores. The WHO recommends that the international standard for diagnosis of osteoporosis be made using the T-score measured at the femoral neck, and this is also the value used by FRAX to calculate future fracture probability. However, guidance by the National Osteoporosis Foundation (NOF, 2010) and the Scottish Intercollegiate Guidelines Network (SIGN, 2003) suggest that in clinical practice the diagnosis of osteoporosis can be made using the lowest T-score of the lumbar spine, total proximal femur, or femoral neck, the rationale being that all of these skeletal sites are good predictors of fracture risk.
DEXA scanning has its limitations. Osteoporosis does not occur equally throughout the body, and thus there may be significant discordance between measurement sites. Spinal osteoarthritis, common in the elderly, may also lead to falsely elevated BMD measurements. Artefacts, incorrect positioning and anatomical deformities, such as a calcified aorta or scoliosis, may also limit the accuracy of DEXA measurements. In such situations, use of the femoral neck T-score to establish a diagnosis of osteoporosis is advised.
Management
Several national guidelines on the topic of osteoporosis management have been produced. NICE has published guidance on the primary and secondary prevention of osteoporotic fractures in postmenopausal women (NICE, 2011). Unfortunately, the NICE guidelines are not directly applicable to premenopausal women or men. However, other bodies have produced guidance that covers both men and women (SIGN, 2003; NOGG, 2010), and the Royal College of Physicians has issued specific guidance on prevention and treatment of glucocorticoid-induced osteoporosis (Royal College of Physicians (RCP), 2002).
The FRAX tool and the NOGG guidance are interlinked. The calculated 10-year risk scores from FRAX can be plotted on a graph via the NOGG website link. This determines whether a person has a low, intermediate or high risk of major fracture. Based on this, NOGG gives advice on further management (Table 2). In general, a 10-year probability of a hip fracture of greater than 3% and that of a major osteoporotic fracture of greater than 20% is an indication for treatment. In all cases, management decisions are based upon a combination of clinical features and risk. Pharmacological intervention is justified when the benefits of fracture risk reduction outweigh the risk of treatment. There are a variety of drugs available, the choice of which is led by national guidance, patient preference and tolerability.
Treatment guidance based on FRAX score and risk of fracture without BMD measurement

Lifestyle advice
Non-pharmacological measures are important in the prevention and treatment of osteoporosis. Patients who are capable of exercise should be encouraged to do so. Thirty minutes of walking at least four times a week should be suggested, as weight-bearing exercise is most effective. Patients should also be encouraged and supported to stop smoking and reduce alcohol intake. Individuals at high risk of falls should be referred to a falls prevention service wherever possible, or at least warrant the involvement of community physiotherapists and occupational therapists.
Calcium and vitamin D supplementation
Adequate calcium and vitamin D intake is important in slowing bone loss. It also has a beneficial effect on musculoskeletal structures, thereby reducing falls. A recent paper has questioned the benefit of calcium supplementation in the management of osteoporosis, in light of several studies suggesting it is linked to an increased risk of cardiovascular events, primarily myocardial infarction (Bolland et al., 2010). The authors even suggested that the cardiovascular risk associated with calcium supplementation might outweigh the benefits of bone protection. However, the studies used in this meta-analysis did not look at combined vitamin D and calcium supplementation, which is more commonly used in the treatment and prevention of osteoporosis. Furthermore, the risk posed at an individual level appears to be quite small. At present, this research has not changed the guidance on calcium and vitamin D supplementation.
The recommended daily intake of calcium for men and women above the age of 50 is 1200 mg. This might be achieved through a normal diet (Table 3). If individuals are able to maintain the recommended daily intake of calcium through dietary means, it may only be necessary to supplement with vitamin D.

Vitamin D is essential for absorption and processing of calcium. The daily recommended intake for an adult is 400 IU. Vitamin D deficiency is common: a British cohort study of 45-year-old adults reported that more than 50% of participants had insufficient levels of vitamin D (Hyppönen and Power, 2007). The main source of vitamin D is from skin photosynthesis following ultraviolet B sunlight exposure. As such, those with pigmented skin and the elderly, who are less mobile, are at the highest risk of deficiency. In addition, dietary sources of vitamin D are limited; the main sources being cod liver oil and oily fish. Therefore, supplementation is often necessary. The advice regarding management of vitamin D deficiency is variable and multiple preparations are available, which can lead to confusion when considering replacement. Standard supplements of calcium and vitamin D contain 500–600 mg of calcium and 400 IU of vitamin D in each tablet. However, for those with significant deficiency this may not be adequate. A recent clinical review in the British Medical Journal (Pearce & Cheetham, 2010) provides practical advice on how to treat vitamin D deficiency according to an individual patient's vitamin D status (Table 4).

Oral vitamin D (calciferol) comes in two bioequivalent forms, either ergocalciferol or colecalciferol. Intramuscular calciferol only comes in the form of ergocalciferol. Intramuscular routes may be preferable in patients with malabsorption disorders. In general, hypocalcaemia and vitamin D deficiency should be corrected before commencing any of the treatments outlined below. Once corrected, combination calcium and vitamin D supplementation should be prescribed long term for those at risk of, or who have, osteoporosis.
Bisphosphonates
Bisphosphonates are the accepted first-line therapy for osteoporosis. They increase bone strength by inhibition of osteoclast activity and induction of osteoclast apoptosis. They can be given via an oral or intravenous route as part of a daily, weekly, monthly or yearly regimen (Table 5).
The bisphosphonates

The oral use of bisphosphonates can be problematic, as they may cause significant gastrointestinal upset and oesophageal ulceration. Side effects can be reduced by making sure the drug is taken correctly (Box 4), yet can still result in poor adherence to treatment; a retrospective cohort study in post-menopausal women found that approximately half of patients discontinued treatment within the first year of commencing oral alendronic acid (Lo et al., 2006). Furthermore, oral formulations are poorly absorbed. Annual intravenous zoledronic acid, however, showed good efficacy in reducing fractures and was generally well tolerated in the HORIZON trial (Black et al., 2007).
Instructions to patients prescribed oral bisphosphonates
Take on an empty stomach first thing in the morning, at least 30 minutes before food or other medication Take in an upright position with plain water Stay upright for 30 minutes after ingestion
Osteonecrosis of the jaw is a rare complication of bisphosphonate therapy. The risk is greater in patients receiving intravenous bisphosphonates in the treatment of cancer compared with those using oral bisphosphonates for osteoporosis. Risk factors that need to be considered include potency of the bisphosphonate, route of administration, duration of treatment (a greater cumulative dose), concomitant treatment (especially steroids), smoking and history of dental disease. The risk of osteonecrosis is increased after dental work, and patients should be made aware of this. All patients, especially those at high risk, should have a dental check up and have any necessary work performed before commencing bisphosphonate treatment. During treatment patients should be advised to maintain good dental hygiene, have regular dental checks and report any oral symptoms.
In recent years, there has also been concern about the risks of atypical femoral fractures in association with bisphosphonate treatment. This is believed to be due to prolonged treatment causing oversuppression of bone turnover, leading to ‘frozen bone’ and thus increased skeletal fragility. Cortical thickening is often seen on plain radiograph. Affected patients are typically on long-term bisphosphonate therapy and usually suffer acute subtrochanteric or mid-shaft femoral fractures. Those who have one atypical femoral fracture are at risk of fracturing on the opposite side. Observational studies suggest that more than 5 years of treatment increases the risk, but the absolute risk is low (Abrahamsen et al., 2009; Park-Wyllie et al., 2011). Nevertheless, patients should be advised to report any thigh, hip or groin pain during treatment.
Contraindications to bisphosphonates include oesophageal disorders, hypocalcaemia and moderate-to-severe renal impairment (the estimated glomerular filtration rate (eGFR) below which therapy is contraindicated varies according to the individual bisphosphonate). Bisphosphonates should also be avoided in women of child-bearing age because of the teratogenic effects that they have on the foetal skeleton, a problem potentiated by their long duration of action.
Strontium ranelate
Strontium is a recommended second-line treatment for primary and secondary prevention of osteoporosis in postmenopausal women, for those who are intolerant of bisphosphonates and meet age, T-score and clinical criteria (NICE, 2011). The exact mechanism of action of strontium is unclear, but it is believed to have a dual effect of stimulating bone formation and inhibiting bone resorption. It is given orally at a dose of 2 g once daily in water. The most common side effect is gastrointestinal upset. Very rarely, it can cause severe systemic skin reactions, such as' drug rash with eosinophilia and systemic symptoms', Stevens–Johnson syndrome and toxic epidermal necrolysis. Patients who develop such reactions should immediately, and permanently, discontinue their treatment. Strontium is also associated with an increased incidence of venous thromboembolism (VTE), and the European Medicines Agency (EMA) has recently deemed that it should not be prescribed to patients who have either a current VTE or a history of VTE. Neither should it be prescribed to patients with temporary or permanent immobilization (EMA, 2012). It is also contraindicated in renal impairment (eGFR below 30 mL/min/1.73 m2).
Raloxifene
Raloxifene is a selective oestrogen receptor modulator. Depending on the target tissue, it can act as either an oestrogen agonist or antagonist. NICE does not recommend it for the primary prevention of osteoporosis, but it can be used for secondary prevention in post-menopausal women, as an alternative for those who are intolerant to bisphosphonates. It is taken orally at a dose of 60 mg once daily. Common side effects include hot flushes and leg cramps. Raloxifene is contraindicated in those with a history of VTE, cholestasis, endometrial cancer or undiagnosed uterine bleeding.
Teriparatide
Continuous exposure to an excess of parathyroid hormone (PTH)—as occurs in hyperparathyroidism—increases osteoclastic activity, thus causing a detrimental reduction in bone mass. However, the intermittent use of recombinant human PTH (teriparatide) actually stimulates bone formation and has been shown to achieve a significant reduction in vertebral and non-vertebral fractures, although not hip fractures (Hodsman et al., 2005). It is given as a daily subcutaneous injection for a maximum duration of 18 months and is indicated as third-line therapy in the secondary prevention of osteoporosis in postmenopausal women if specific T-score and clinical criteria are met (NICE, 2011). Specialist advice should be sought if patients meet these criteria before initiation of therapy in primary care. Common side effects include gastrointestinal upset, headaches and dizziness. It should be avoided in patients with pre-existing hypercalcaemia, primary or secondary bone malignancy, Paget's disease, hyperparathyroidism and a history of skeletal radiotherapy.
Denosumab
Denosumab is an established monoclonal antibody that is now available for the prevention and treatment of osteoporosis in post-menopausal women. It is a fully humanized monoclonal antibody that selectively binds to (receptor activator of the nuclear factor κB ligand (RANKL). Under normal circumstances, RANKL interacts with its receptor, promoting osteoclast differentiation and activation. Denosumab interferes with this interaction, thus having the targeted effect of reducing osteoclast activation and bone resorption. It is given as a 60 mg subcutaneous injection every 6 months. NICE has recently updated its guidance to include denosumab as an option in the primary and secondary prevention of post-menopausal women (NICE, 2010). Side effects include pain in the extremities and minor infections, particularly cellulitis. There is also an association with osteonecrosis of the jaw, and therefore the same advice should be given as for patients taking bisphosphonates. Hypocalcaemia should be corrected before treatment is commenced. Denosumab can be prescribed to those with renal impairment, but it should be noted that patients might be at higher risk of developing hypocalcaemia if their eGFR is below 30 mL/min/1.73 m2.
Specific circumstances
Osteoporosis in men
Osteoporosis in men is under-diagnosed and under-treated, yet it is very much a condition of our time. In many cases, a specific cause may not be identified, although family history, as in women, is a strong predictor. As expected, the secondary causes of osteoporosis in men largely overlap with those in women and include glucocorticoid use, hyperparathyroidism, thyroid disease and excessive alcohol use (which may play a more significant role than in women). Another important cause is physiological hypogonadism, which results in low levels of circulating testosterone. A significant iatrogenic cause of a low testosterone level is androgen-deprivation therapy, often used to treat prostate cancer. The treatments available for osteoporosis have been less extensively researched in men, and currently only bisphosphonates and teriparatide are recommended.
Glucocorticoid-induced osteoporosis
Oral glucocorticoids are associated with a significantly increased risk of fracture at the hip and spine, particularly when taken at higher doses. Loss of BMD is highest in the first few months of treatment. Patients aged over 65 years or who have had a previous fragility fracture should be commenced on bone protective therapy at the time of starting glucocorticoids, without the need to measure BMD. In other individuals, it is recommended that a DEXA scan is performed to assess fracture risk (RCP, 2002); a T-score of −1.5 or lower may indicate the need to commence bone protective therapy, although individual choice and suitability should be taken into account.
Osteopenia
Individuals who have a T-score of between −1 and −2.5 on DEXA scanning should be educated about osteoporosis, including risk factors for its development. Lifestyle factors such as levels of alcohol consumption, smoking and exercise should also be discussed. Calcium and vitamin D supplementation should be recommended, especially in those with a poor diet. Repeat DEXA scanning after 3–5 years should be considered in those who remain at high risk of developing osteoporosis.
Follow-up and duration of treatment
There is no consensus on how long to continue bone protective treatment. This is of particular concern with bisphosphonate therapy, which causes an increased incidence of adverse events with prolonged duration of treatment. Bisphosphonates continue to prevent fractures even after treatment is stopped at 5 years, suggesting residual effects on BMD. Therefore, it may be reasonable to discontinue treatment after 5 years. However, this decision should be based upon individual patient factors. For example, a ‘drug holiday’ may be a suitable option for patients who have a stable BMD, no history of previous vertebral fracture and who are at low risk of future fracture. However, high-risk patients should probably continue treatment for at least 10 years. The duration of the drug holiday may vary from 1 to 5 years, with the decision to restart treatment dependent on a variety of factors, including a measured decrease in BMD, change in clinical risk for fracture, or occurrence of fragility fracture. Ideally, decisions about when to institute a ‘drug holiday’, and for how long, should be made with specialist guidance.
Follow-up DEXA scanning can be used to assess treatment efficacy and is often used in clinical trials. However, no trials have assessed the utility of follow-up DEXA in routine clinical practice (SIGN, 2003) and usually it is unnecessary, because it should only be carried out if the results are likely to influence clinical management. Circumstances in which it may be required include a patient who fractures on treatment, if considering a change in treatment, or when considering restarting therapy after a drug holiday. Different localities may have their own policies for follow-up scans. If a repeat DEXA is needed, the best site to monitor is the lumbar spine, as this site quickly responds to therapy. If the lumbar spine is not available, due to spinal deformities or degenerative disease, then the proximal femur should be used for comparison. Ideally, the same DEXA scanning machine should be used for comparison, and generally a repeat scan should only be undertaken after 2 years of therapy. The BMD response, rather than changes in T-score, should be assessed. Increases of at least 3–4% BMD are required as evidence for treatment efficacy (SIGN, 2003).
Primary care has an important role to play in the management of osteoporosis; this is reflected in the new quality and outcomes framework (QOF) indicators (Box 5). Most patients with osteoporosis can be adequately followed up and managed without the need to involve secondary care services. However, certain scenarios may pose difficulties, for example, due to diagnostic uncertainty or poor treatment response; these situations warrant referral for a further opinion (Box 6).
QOF clinical Indicators for osteoporosis
Practices need to have a register of patients who have had a fragility fracture after 1 April 2012, who are either aged 50–74 years with a diagnosis of osteoporosis confirmed on DEXA scan, or aged 75 years and over QOF points are awarded according to the percentage of these patients who are currently receiving an appropriate bone-sparing agent, with one indicator for the 50- to 74-year age group and another for those aged over 75 years
Referral for a specialist opinion
Urgently in those you suspect have an alternative cause for their fracture, for example, malignancy or myeloma In which a diagnosis of osteoporosis is unusual, such as pre-menopausal women and men Patients in whom first line therapy is contraindicated or not tolerated, and either intravenous bisphosphonate, teriparatide or denosumab may be suitable Patients who develop fragility fractures despite being on treatment
Conclusion
Osteoporosis is a common condition that is becoming increasingly prevalent as our population ages. It is associated with a significant socioeconomic health burden, as resultant fractures have a severe impact on a patient's quality of life, and the rehabilitation process that is often needed can be arduous and lengthy. Therefore, there is a growing trend towards opportunistic finding of patients at risk and early commencement of treatment. GPs have a vital role to play in this process. Fracture risk-assessment tools can help in identifying those in need of treatment, and national guidance provides advice on appropriate management.
Key points
Osteoporosis is common and has a significant impact on patient morbidity and mortality Management should focus on early detection of osteoporosis, prevention and exclusion of secondary causes Patient education and engagement is a crucial part of the management of this debilitating condition National clinical guidance and risk-assessment tools are useful adjuncts when making treatment decisions
Footnotes
Acknowledgements
We would like to thank Dr Vasandhara Thoroughgood for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.