
Abstract
Cervical cancer is the 11th most common cancer in women. Cervical screening aims to reduce the number of women who develop invasive cervical cancer and, consequently, the number of deaths caused by cervical cancer, by regularly screening women so that cervical abnormalities that might otherwise develop into invasive cancer can be identified and treated. GPs play an important role in raising awareness of cervical cancer and ensuring that women are provided with the necessary information and advice to assist them in making an informed choice about attending cervical screening appointments.
The GP curriculum and cervical screening
The knowledge-based requirements in
Be familiar with and implement the key national guidelines that influence healthcare provision for women's problems
Use screening strategies relevant to women (e.g. cervical, breast, other cancers, postnatal depression) and advise patients on their advantages/disadvantages
Inform patients of the results of screening and ensure follow-up
In addition,
Explain to the patient and/or their relatives the evidence about a screening programme and debate whether it is worthwhile—for individuals or groups
Epidemiology
In the UK, in 2009 there were 3378 new cases of cervical cancer diagnosed, making it the 11th most common cancer in women and accounting for 2% of all cancers in women (Cancer Research UK, 2012a). Cervical cancer almost exclusively occurs in women who are or who have been sexually active. There are two peaks of incidence, one in women aged 30–34 years and the other in women aged 80–84 years. Four out of every five women with cervical cancer have squamous cell cancer; the remainder adenocarcinoma. Incidence is dropping, probably due to the cervical cancer screening programme and changes in sexual practices. In England, it is estimated that cervical screening saves approximately 4500 lives every year.
Pathology
Cervical cancer usually develops slowly over many years. It is preceded by a premalignant phase characterised by the transformation and abnormal growth of cells on the cervix. These cellular changes, known as dyskaryosis, relate to defined grades of cervical abnormalities known as cervical intraepithelial neoplasia (CIN).
CIN grades correspond to the different risks of progression to cervical cancer. Low-grade disease (CIN 1) is recognised to have low risk of development to cervical cancer, whereas high-grade disease (CIN 2 and 3) has a relatively high risk of progression. Early detection and treatment of CIN can prevent around 75% of cervical cancers developing (NHS Cervical Cancer Screening Programmes, 2006a). The purpose of cervical screening is to identify abnormal cellular changes in the cervix—CIN. Abnormalities can then be managed in accordance with the likelihood of them progressing to invasive cervical cancer.
The role of human papillomavirus
Human papillomavirus (HPV) is found in more than 99% of patient samples that show cervical cancer. There are over 100 subtypes of HPV, but the high-risk HPV subtypes (HR-HPV), notably types 16 and 18, 31 and 33, are associated with cervical cancer.
HPV is one of the most common sexually transmitted infections; the majority of sexually active women will contract HPV at some point in their lives. Most infections will be resolved by the body's immune system. However, in a minority of women HPV can persist. Persistence of high-risk strains of the virus confers a higher risk of developing cervical cancer.
Symptoms
Abnormal changes to the cervix that occur prior to the development of cancer (i.e. CIN) are usually asymptomatic and thus not detected by the woman. However, there are several symptoms that may indicate the presence of malignancy. These commonly include intermenstrual bleeding and post-coital bleeding. Vaginal discharge may also rarely occur, as can discomfort or pain during sexual intercourse (usually in more advanced disease). Importantly, cervical screening should never be used as a diagnostic test to investigate women who have these symptoms; screening is for asymptomatic women only. Any woman who experiences symptoms suggestive of cervical cancer should be seen and assessed in the practice or at a genito-urinary medicine clinic, where suitable investigations and, if necessary, a referral to secondary care can be arranged.
Criteria for a screening programme
The idea of cancer screening is attractive—the ability to diagnose and treat a potentially serious condition at an early stage when it is still treatable. An ideal screening test should pick up all those who have the disease (have high sensitivity) and must exclude those who do not (high specificity). It must detect only those who have a disease (high positive predictive value) and should exclude only those who do not have the disease (high negative predictive value).
The World Health Organization (WHO) recommends that screening should only be introduced to the target population if the following (Wilson–Jungner) criteria are met (Wilson & Jungner, 1968):
The condition being screened for is an important health problem
The natural history of the condition is well understood
There is a detectable early stage
Treatment at early stage is of more benefit than at late stage
There is a suitable test to detect early stage disease
The test is acceptable to the target population
Intervals for repeating the test have been determined
Adequate health service provision has been made for the extra clinical workload resulting from screening
Risks, both physical and psychological, are less than the benefits of screening
The costs of screening are worthwhile in relation to the benefits gained
All cervical screening programmes within the UK are required to fulfil these criteria. It is estimated that cervical screening can prevent around 45% of cervical cancer cases in women in their 30s, rising with age to 75% in women in their 50s and 60s, for those who attend regularly (Cancer Research UK, 2012b). The increased effectiveness in older women is reflected in the lengthening of the screening interval at the age of 50, from 3 to 5 years. A summary of screening statistics for the UK devolved nations is included in Table 1.
Cervical cancer screening statistics in the devolved nations of the UK

Source: Cancer Research UK (2012b).
The cervical screening process
Cytology
The National Health Service Cervical Screening Programme (NHSCSP) uses cytological screening to detect abnormal changes to cells on the cervix that relate to CIN. As opposed to histology, which examines tissue structure, cytology allows screening professionals to examine changes at a cellular level. A sample of cells is taken from the area of the cervix where the majority of cervical cancers originate, known as the transformation zone.
The sampled cells are then sent to a laboratory for examination under a microscope by a cytologist and the results are classified, according to the grade of changes seen, as low-grade (mild) or high-grade (moderate or severe) dyskaryosis, or borderline nuclear changes only. Depending on the findings and the patient's screening history, a cytology report will recommend an appropriate course of action for the patient's clinical management.
Introduction of liquid-based cytology
The NHSCSP now uses liquid-based cytology (LBC). This replaces the previous cytology practice of cervical smear testing, in which the cervical sample was smeared in a layer directly onto a glass microscope slide, leading to the adoption of the term ‘cervical smear’.
In LBC, the cells are collected with a brush and the head of the brush is either broken off into a small vial containing preservative fluid or rinsed in the fluid. The vial is sent to the laboratory where it is treated to remove obscuring material. A random sample of the remaining cells is then taken, and a thin layer of the cells is deposited onto a slide. The slide is then examined in the usual way under a microscope by a cytologist.
In 2003, the National Institute for Health and Clinical Excellence recommended that LBC should be used as the primary means for processing samples in the NHSCSP. This was based on a range of factors, including the potential for increased sensitivity and better quality of slide preparation, allowing faster and more reliable screening by laboratory staff, and a lower rate of inadequate samples. Cervical sampling using LBC became the standard method of screening within the NHSCSP from October 2008, following successful pilot programmes in three areas of England that evaluated the effects, costs and practical implications of introducing LBC technology.
For GPs taking cervical screening samples, it is important to have adequate training. Poor sample taking misses 20% of abnormalities. Courses are available and ideally skills should be updated every 3 years. Practices should regularly audit their own performance in relation to other practices and also the performance of individual sample-takers within the practice.
Colposcopy
Women whose samples show abnormalities needing further investigation are referred for colposcopy, where a detailed assessment of the cervix takes place. During the procedure, biopsies may be taken.
Age and eligibility
Throughout the UK, women are invited for regular cervical cancer screening but arrangements are slightly different in each of the devolved nations (Table 2).
Screening programmes in different parts of the UK

Women older than the upper age for screening can be screened if they have never been screened previously or are under recall for previous abnormal results.
When does screening begin?
Cervical screening works by diagnosing and treating many more cases of CIN than would ever develop into cervical cancer. For women in their mid-20s onwards the balance of opinion is that benefits outweigh harms. However, for younger women the benefit is of a lesser magnitude. Cervical abnormalities are common in women under the age of 25, but cervical cancer in this age group is very rare. In the vast majority of cases in these younger women, the abnormalities are transient. If abnormalities are found, the follow-up gynaecological investigation and colposcopy can increase the likelihood of the woman having a pre-term delivery during pregnancy, which can endanger both the baby and mother.
In England and Northern Ireland, the screening age was raised from 20 years in 2003, following a recommendation from the independent Advisory Committee on Cervical Screening (ACCS). In June 2009, the Committee reviewed the policy and agreed unanimously that there should be no change. International research, including that produced by the WHO's International Agency for Research on Cancer, suggests that screening women under the age of 25 years does not reduce mortality from cervical cancer. Figures released by the Office for National Statistics show that there has been no increase in mortality in the under 25s since the starting age was raised in 2003 (Office for National Statistics, 2012).
Young women do, however, present with cervical cancer, albeit rarely. To address this the Department of Health has published clinical practice guidelines for the assessment of young women aged 20–24 years with abnormal vaginal bleeding (Department of Health, 2010a). The screening age for women remains 20 and over in Scotland and Wales.
What determines the screening interval?
In 2003, it was recommended that women be invited for cervical screening from 25 years old and then recalled every 3 years between the ages of 25 and 49 years and every 5 years between the ages of 50 and 64 years in England and this policy was subsequently adopted in Northern Ireland too (Luesley & Leeson, 2010). This is because a 3-yearly screening interval for younger women offers significantly improved disease outcomes, whereas screening more frequently than every 5 years in women aged 50–64 years is not effective in improving outcomes (Sasieni, Adams, & Cuzick, 2003). The sceening interval is 3 years whatever the age of the woman in Scotland and Wales.
Why does cervical screening stop at the age of 65 years?
The natural history and progression of cervical cancer means it is highly unlikely that women aged 65 years and over, who have been regularly screened, will go on to develop the disease. Consequently, women are taken out of the call and recall system unless they need ongoing surveillance or follow-up. However, women aged 65 years and over who have never had a test are entitled to one.
Where are women screened?
Women can choose to be screened either at a GP practice or at a community sexual health clinic. All practices with General Medical Services contracts are expected to perform cervical screening for all women registered with the practice in the eligible age range as an additional service. Opting out results in a 1.1% decrease in the Global Sum Payment. Practices undertaking cervical screening can also gain Quality and Outcome Framework points through their cervical screening programmes. A full list of GP responsibilities in relation to cervical screening is set out in Box 1. In most GP practices practice nurses undertake the majority of cervical screening tests, with GPs taking samples opportunistically and from patients with whom practice nurses have had difficulty.
GP practices are responsible for
Ensuring that the woman is provided with the necessary information and advice to assist her in making an informed choice about whether to participate in screening or not
Maintaining a register of tests taken
Ensuring that there is a system for notifying women of their test results in writing. This may be through the routine call and recall system administered by the primary care trust. The GP is responsible for checking that the address on the test request form is up to date
Ensuring that arrangements are made for women who fall outside the call and recall system (such as temporary residents) to be given their test results
Checking that a test result has been received from the laboratory for every sample taken
Acting on non-responder notifications for women who have not responded to an invitation for:
A routine test
An early repeat test
Colposcopy
When appropriate, explaining to a woman with an abnormal result why urgent referral is required
Referring the woman urgently, if this is not done automatically
Referring a woman for colposcopy, if required
Ensuring that colposcopy has taken place (the GP is responsible for this even if there is a direct referral system from the laboratory to the colposcopy clinic)
Responding to fail-safe enquiries by laboratories. Failure to respond is a clinical governance issue
Identifying women for whom screening is not appropriate (such as women who have had a total hysterectomy and adequate subsequent follow-up) and ensuring that they have been removed from the call and recall system.
Cervical screening in lesbian women
In the past it was believed that high-risk HPV could only be transmitted through heterosexual relationships, leading to the incorrect assumption that lesbian women are not at risk of cervical cancer and therefore do not need to be screened. However, HPV can be transmitted through intimate skin-to-skin contact between partners (i.e. penetrative intercourse is not required), thus although these women are at low risk, they cannot be said to be at no risk of contracting the virus. Women at low risk should still be invited for screening, although they may choose not to take up their invitation.
The structure of services
In England alone, the NHSCSP screens more than 3 million women each year (NHS Information Centre Statistics, 2011) with separate cervical screening programmes covering Wales, Scotland and Northern Ireland. More than 100 000 NHS employees are involved in the NHSCSP in England. They include sample-takers in GP surgeries and community clinics, laboratory staff who review the samples and administrative staff who run the computer systems. These activities are coordinated by the national office of the NHS Cancer Screening Programmes, and quality assurance (QA) is managed via regional QA Reference Centres.
Establishing the NHSCSP
Health services originally began providing women with cervical screening in the UK in the mid-1960s and by the mid-1980s many women were having regular tests. However, it soon became apparent that a significant proportion of eligible women were not being tested and others who had positive results were not being followed up and treated effectively.
In 1988, the Department of Health published guidelines to facilitate the implementation of a population-based cervical screening programme in England (Department of Health, 1988). Regional health authorities were instructed to carry out cervical screening in an organised programme to ensure that the maximum numbers of eligible women in their locality were invited for screening at the appropriate time, and received their results and any necessary follow-up in a timely manner.
Call and recall
The call and recall system invites eligible women who are registered with a GP for cervical screening, keeps track of their full screening history, any follow-up investigation, and recalls the woman for screening at the appropriate time. Details of women eligible for screening are obtained from GP records. It is therefore important that all women ensure their GP has their correct name and address details and inform them if these change.
Advisory Committee on Cervical Screening
The NHSCSP follows recommendations from the ACCS. This is an independent body made up of cervical screening experts that advises on the development of cervical screening services, monitors the effectiveness and efficiency of the NHSCSP and considers new research about the provision of screening services.
HPV testing
The NHS Operating Framework 2011/12 confirmed that from April 2011 commissioners should work with their local services and the NHS Cancer Screening Programmes to incorporate HPV testing into cervical screening (Department of Health, 2010b). The recommendation came after years of research into the role of HPV in the development of cervical cancer, and work through the HPV pilot scheme and the Sentinel Site Implementation Project, which analysed how to incorporate HPV testing into the NHSCSP most effectively.
HPV triage is a process by which the residuum of the cytology sample in the vials containing cells with low-grade abnormalities [borderline changes or mild (low-grade) dyskaryosis] are tested for high-risk HPV. Under current NHSCSP guidelines, women with abnormalities are referred for further investigation using colposcopy. However, only 15–20% of these women go on to receive further treatment as low-grade cervical abnormalities often clear up on their own. Women whose samples are negative for high-risk HPV are simply returned to routine recall. Test of cure is the process by which women are tested for HPV after they receive treatment for CIN (i.e. at their first follow-up screening). See Fig. 1 for further details of the pathway for different cervical screening results.
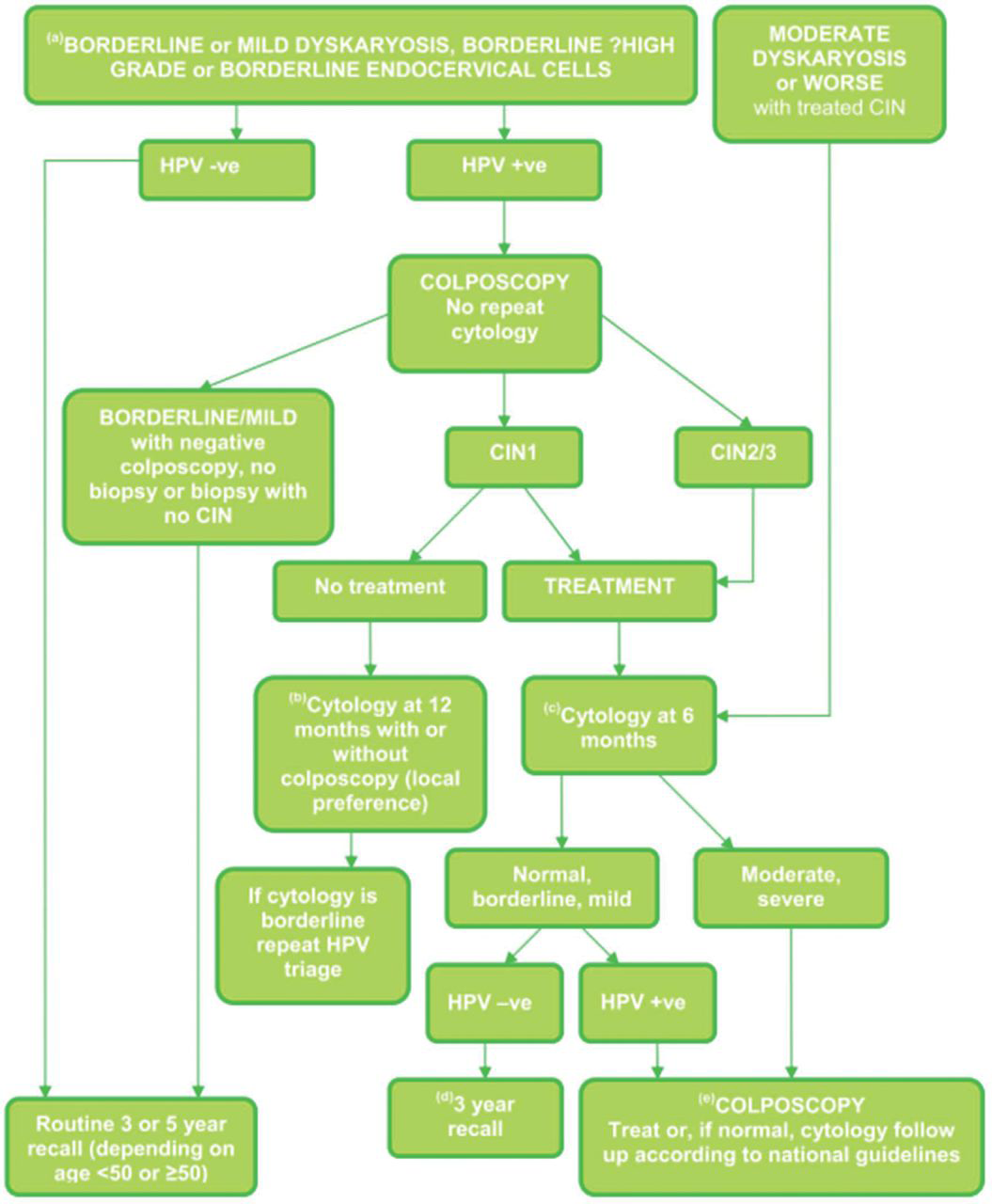
HPV triage and test of cure protocol for the management of women aged 25–64 years in the NHSCSP.
Six sentinel sites were established in 2008 to assess the practical implementation of national roll-out of HPV triage for women with borderline changes or mild dyskaryosis, and also of HPV testing as a test of cure for women who have been treated for CIN. Together these six sites (Bristol, Norwich, Liverpool, Manchester, Northwick Park and Sheffield) covered approximately 10% of the eligible screening population. The sentinel sites programme concluded that with careful management of the initial increase in referrals to colposcopy, HPV triage and test of cure could be successfully implemented.
The roll-out of HPV testing will be an important development. It enables women to be screened more effectively and efficiently, reducing unnecessary repeat tests, and minimising any associated anxiety. HPV triage for women with borderline changes or low-grade abnormalities found at routine screening is being introduced in 2012/13, along with test of cure for women newly treated for CIN. In 2013/14, HPV triage will be extended to all borderline/low-grade results (from both routine and follow-up screening), and HPV test of cure to all follow-up screenings after treatment.
Ongoing priorities
Improving uptake
Age is a significant indicator of uptake. The number of women aged 25–34 years accepting cervical screening has steadily declined over the last 10 years. This trend was temporarily reversed a few years ago by the public reaction to the diagnosis of cervical cancer in, and subsequent death of, the television celebrity Jade Goody.
Screening inequalities also manifest themselves in reduced uptake among particular groups in society, i.e. fewer people accepting their screening invitation. Understanding why there is low uptake in certain groups allows the NHS to adapt and better position its screening services to improve participation.
Work continues to improve engagement with younger women and other hard-to-reach groups such as black and minority ethnic communities, where uptake is known to be lower. GPs can play an important part in raising awareness among these groups by discussing the benefits of regular cervical screening with eligible women during health appointments and making information readily available within the practices. A variety of publications and materials including informational posters, leaflets and audio learning tools are available free of charge for NHS staff. These can be ordered through the NHS Cancer Screening Programmes either by phone or via the website.
Turnaround times
In recent years, screening programmes have worked hard to collect, process and return cervical screening samples within shorter time frames. Today, turnaround times have been significantly reduced, with 98.6% of results being reported by laboratories within 14 days, compared with 43% 5 years ago (NHS Cancer Screening Programme, 2011).
Key points
Cervical cancer is the 11th most common cancer among women in the UK, accounting for around 2% of all new cases of cancer in women; in 2009, over 3300 new cases of cervical cancer were recorded in the UK
Cervical screening is aimed at women without symptoms. It is not a test for cancer but a method of preventing cancer by detecting and treating abnormalities within the cervix that, if left untreated, could develop into cancer
In England, it is estimated that cervical screening saves approximately 4500 lives every year
GP practices undertake cervical screening as an additional service; opting out results in a 1.1% drop in the Global Sum Payment
GPs undertaking cervical screening tests should have training to do this and regularly audit their practice and own performance