
Abstract
Objective
To examine the relationships of job strain and iso-strain psychosocial work environment exposures to ‘total coronary risk’ (TCR) in a cohort of male and female workers in Belgium.
Methods
The sample consists of 15 079 men and 4639 women aged 35-59 years employed in a wide range of occupations and free of any self-reported personal history of CHD. Karasek's job strain model was used to define high strain (high demands and low control), low strain, active and passive jobs. Iso-strain was defined as the combination of a high strain job with low worksite social support, and is compared to the other combinations. Total coronary risk is a composite measure based on a Framingham function assessing the risk of developing coronary heart disease (CHD) within the next 10 years; high and low levels of TCR were defined. Logistic regressions in each gender were applied to explore relationships, adjusting for age, level of education, occupational class and sector of employment.
Results
In male workers, the age-adjusted prevalence of high TCR is highest in (1) in the lowest quartile group of job control and (2) in the ‘high strain’ group. The multivariate logistic regressions comparing high strain, active and passive work exposures to low strain work did not indicate a significant association with high TCR. Likewise, iso-strain jobs were neither found to be associated with high TCR.
Conclusion
Our cross-sectional analysis provides no support for the hypothesis that the psychosocial work environment is strongly associated with the TCR estimate in healthy workers. Eur J Cardiovasc Prevention Rehab 10:345-354 © 2003 Lippincott Williams & Wilkins.
Introduction
Research over the past decades on chronic psychosocial stress at work has resulted in a large body of empirical evidence of the adverse health effects of work that are high in psychological job demands and low in level of job control [1]. In the late 1970s, both elements were combined by Karasek into his two-dimensional ‘job strain’ model, proclaiming that ‘high strain’ occurs when there are excessive workload demands with low decision latitude or job control [2]. This situation can be contrasted to other psychosocial work exposure categories such as ‘active’ (high demands with high control), ‘passive’ (low demands with low control) and ‘low strain’ jobs (low demands with high control). The main hypothesis is that high strain jobs will show the highest occurrence of stress-related illness while low strain jobs by contrast are considered much better from a health perspective. Active and passive jobs are expected to show average or some intermediate levels of adverse health effects, but will differ markedly with respect to active/passive behavioural correlates of jobs, such as learning ability and motivation [2, 3].
Later on, the model was elaborated in several ways but the most important extension relates to the addition of a third dimension: worksite social support. According to the extended ‘iso-strain’ model, the most noxious combination is high demand together with low control and low support. The impact of this model has been the basis of much research and generally has found considerable support in empirical studies [4–9].
In the field of cardiovascular diseases (CVD), results of a first prospective study using the job strain model appeared in 1981 showing a significant association between working in high strain jobs and increased likelihood of subsequent development of heart disease symptoms and/or cardiovascular mortality among the Swedish male working population [10]. In the late 1980s, it was observed that low social support at work had a main effect on CVD or could amplify the effect of job strain on CVD outcomes [4, 5, 7]. More recently, an authoritative state-of-the-art review on the subject covering 23 studies using different designs concludes that the evidence suggests a dose-response relationship—both in terms of point exposure [11] and temporal duration [12]—between exposure to job strain or low job control and subsequent CVD, at least in men [13]. Likewise, in five out of seven reviewed studies among women using either a prospective cohort or a case-control design, it was equally found that exposure to high job strain or one of its components (high demands/low control) was associated with higher levels of coronary heart disease (CHD) [14].
Given these findings, a main question to be asked is whether the increased CHD risk linked with psychosocial stress at work is mediated by the conventional coronary risk factors. A lot of research indeed surveyed the effect of individual risk factors. Noteworthy in this respect are the strong and consistent positive associations observed between job strain or one of its components and ambulatory 24h recordings of blood pressure [13–22]. Casual blood pressure recordings generally produced less convincing associations [13]. Among men, smoking intensity rather then smoking prevalence was found to be associated with psychosocial job stressors [13, 23, 24]. By contrast, no clear and significant associations were reported between job strain and serum cholesterol (total and HDL) [13, 14, 25], while findings as regards the link between job strain and sedentary behaviour, obesity or high-fat diet are inconclusive still [13, 14]. Noteworthy however are recently published findings from a longitudinal study among industrial employees in Finland showing that work-related stress predicted adverse changes in biological factors such as cholesterol concentration and body mass index [9].
It has been raised however that, as CHD is multi-factorial in origin, it is important to consider various risk factors simultaneously in order to assess the total risk for an individual of developing coronary heart disease over a limited period of time [26]. Indeed, clusters of risk factors may have a multiplicative effect so that an individual with a number of modest risk factors may be at a considerable larger risk than a person with just one very elevated risk factor. From this, it can be deduced that a due consideration of the impact of work-related psychosocial stress on conventional CHD risk factors in turn should account for these synergistic effects. Some measure of ‘total coronary risk’ taking into account all the major risk factors, is therefore needed. For healthy individuals, one such measure based on a risk function derived from the Framingham study [27] has gained much attention among expert committees dealing with prevention of cardiovascular diseases [26, 28]. More particularly, the Framingham risk function calculates for individuals free from cardiovascular disease the risk of developing CHD within the next 10 years based on a number of recognised risk factors. Risk charts for use in clinical practice based on that function generally perform well in populations with moderate or high levels of CHD incidence [26], which is still the case for Belgium [29, 30].
In this paper, we will focus attention on the cross-sectional relationship of perceived job stress factors to the estimated 10-year CHD risk as predicted by the Framingham function in a cohort of the Belgian workforce. Our research hypotheses may be stated as follows:
Higher levels of job demand and lower levels of job control or of social support at the workplace will be associated with a higher level of ‘total coronary risk'
Within the job strain model, workers in a ‘high strain’ job will display the highest ‘total coronary risk’ profile;
Within the iso-strain model, workers having an ‘isostrain’ job are predicted to be worst off.
Subjects and methods The BELSTRESS study cohort
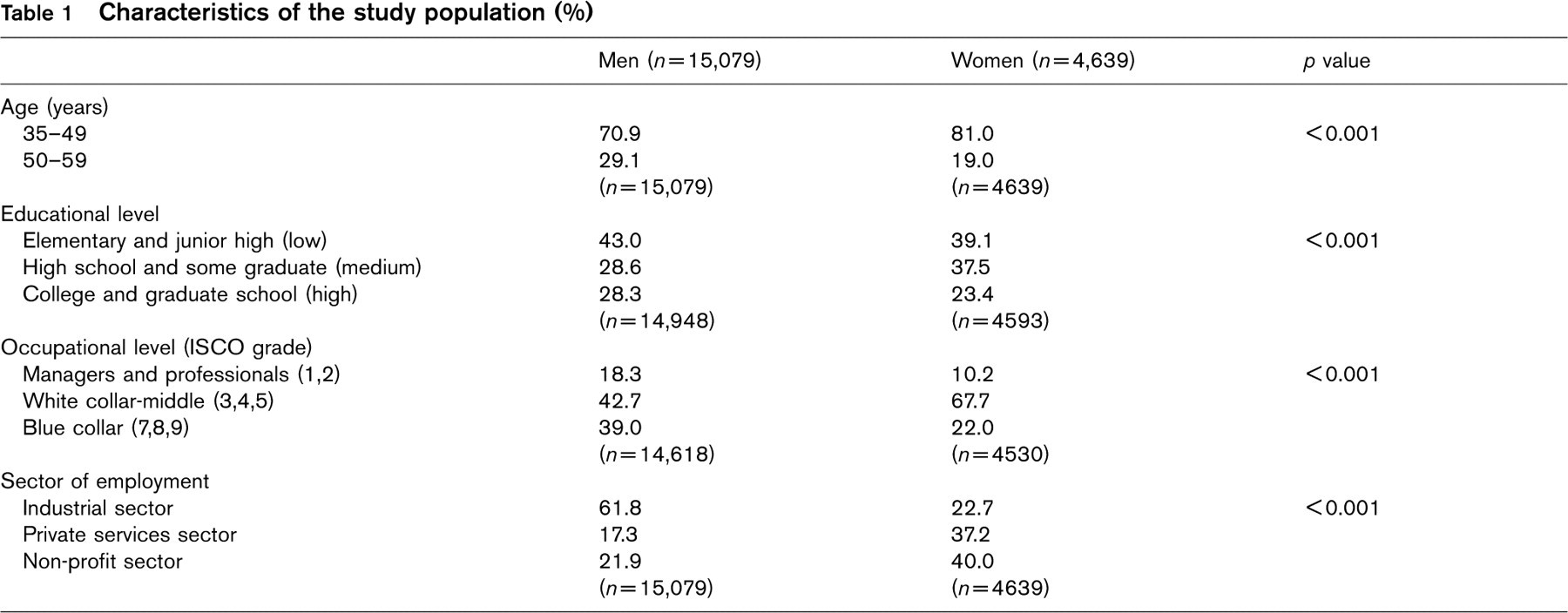
The Belgian Job Stress Project (BELSTRESS) is a multidisciplinary large-scale study dealing with the independent relationship between perceived job stress and health problems [31]. The study is part of the larger JACE-study, the acronym for ‘Job stress, Absenteeism and Coronary heart disease—European cooperative prospective study’ [32]. The initial sample consists of middleaged men and women (35-59 years) at work in 25 large Belgian industries or administrations. The data collection was conducted in the period between 1994 and 1998; a total of 21419 participants (16329 men and 5090 women) complied with the study, giving a participation rate of 48%, (Table 1). Participants were requested to complete a questionnaire and to attend a medical examination at the workplace.
In the present analysis, we excluded 1250 men (7.7%) and 451 women (8.9%) who had a possible history of angina pectoris (Rose questionnaire [33]) and/or a previous hospitalisation for acute myocardial infarction, percutaneous transluminal coronary angioplasty or coronary-artery bypass graft. This was done to minimize the potentially confounding effect of major CHD illness on the relationship between psychosocial work exposure and estimated total CHD risk.
Measurement of the outcome
‘Total coronary risk’ (TCR) based on the Framingham function takes several independent risk factors into account. These include age and gender, systolic blood pressure (mean of two standardized measurements), ratio of serum total cholesterol over HDL cholesterol (levels determined in a central laboratory from a blood sample taken on the site), cigarette smoking (smoking or quit within past year versus otherwise according to the questionnaire), diabetes mellitus (self-reported) and diagnosis of left ventricle hypertrophy (LVH) as measured by electrocardiography [27]. The function generally produces fairly reliable absolute risk estimates in predicting the development of different clinical manifestations of coronary heart disease in individuals free of disease. The function is apt for use in populations with high or moderate levels of CHD-incidence rates, using a prediction interval between four and 12 years [27]. The model is even more robust when discriminating low from moderate-to-high risk subgroups in different populations. We used the standard 10-year interval, so that ‘total coronary risk’ stands for the risk of developing CHD within the next 10 years, (Table 2).
The variable displays extreme skewness so that a recoding into a 1/0 dichotomous variable was considered for use in logistic regressions (Table 2). In men, a standard cut-off point of 0.20 was adopted contrasting men with relatively high risk levels (≥ 0.20) to men with relatively low risk levels (<0.20); in women, a standard cut-off point of 0.10 was adopted accounting for the much lower mean incidence rate.
Measurement of exposure
Items designed to measure ‘psychological job demands’ (9 items), ‘job control’ (9 items) and social support at the workplace (8 items) are those that belong to the full recommended 1985 version of the Job Content Questionnaire (JCQ) [34]. The job control or ‘decision latitude’ scale is composed of two subscales, namely ‘skill discretion’ (6 items) and ‘decision authority’ (3 items). Social support also is built up from two subscales, for example, supervisor support (4 items) and co-worker support (4 items). Each item has a response set of four ordinal categories, varying from ‘fully disagree = 1’ to ‘fully agree = 4′. In order to reduce the number of missing values, it was decided that in case of one missing value per (sub)scale it would have the mean value imputed which would be calculated over the set of remaining valid (sub)scale items for that particular respondent, picking up 5% more cases at most. All JCQ-scales proved to contain acceptable scale reliability (Cronbach's α between 0.66 and 0.87 in men; α between 0.66 and 0.88 in women) and validity in the BELSTRESS cohort [35]. Quartile groups on each scale define different levels of exposure, from low (Q1 = quartile group 1) to high (Q4 = quartile group 4).
Characteristics of the study population (%)
Distribution of total coronary risk per gender
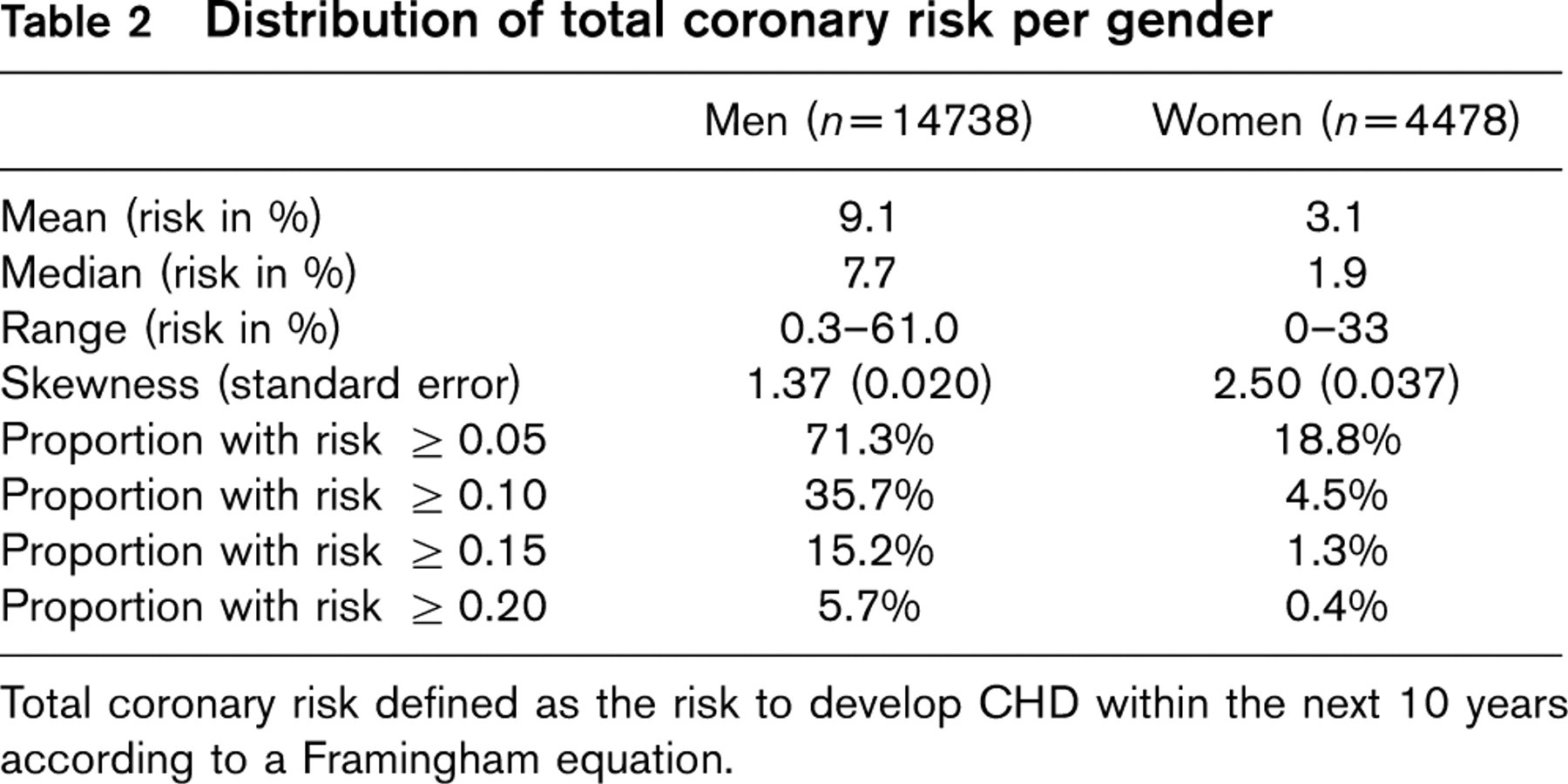
Total coronary risk defined as the risk to develop CHD within the next 10 years according to a Framingham equation.
To measure job strain, the job demands and job control scales were converted to dichotomous measures according to the gender-specific median split. The cross-classification of both measures produced the standard quadrant scheme with the four exposure categories already mentioned: ‘low strain’ (low demands with high control), ‘active’ (high demands with high control), ‘passive’ (low demands with low control) and ‘high strain’ (high demands with low control) [6, 20].
As an alternative, we also constructed a more diverse job strain variable based on the distribution in quartile groups of job demands and job control. It discriminates between six exposure categories: ‘extreme low strain’ (Q1 of job demands with Q4 of job control), ‘mild low strain’ (Q2 of job demands with Q4 of job control; Q1 or Q2 of job demands with Q3 of job control), ‘active’ (Q3 or Q4 of job demands with Q3 or Q4 of job control), ‘passive’ (Q1 or Q2 of job demands with Q1 or Q2 of job control), ‘mild high strain’ (Q3 or Q4 of job demands with Q2 of job control; Q3 of job demands with Q1 of job control) and ‘extreme high strain’ (Q4 of job demands with Q1 of job control).
To measure iso-strain, the social support scale was split on the median as well as in each gender, with subjects above the median classified as receiving high support. The ‘iso-strain’ category (high strain with low support) was contrasted to the ‘high strain and high support’ category, the ‘no strain and low support’ and ‘no strain and high support’ categories. Here, ‘no strain’ was defined as the complement of ‘high strain', comprising the active, passive and low strain groups of the standard quadrant scheme.
Finally, ‘job insecurity’ was considered as an additional indicator of the psychological work environment. The measure was built up as a sum score from two related JCQ items, assessing the present and the future situation. The scale ranged between two and eight and had acceptable internal consistency reliability (Cron-bach's α = 0.68 in both genders). Quartile groups defined the levels of exposure, from low (Q1 = quartile group 1) to high (Q4 = quartile group 4).
Measurement of covariates
In Table 1, a set of potential confounders of the relationship between perceived job stress and TCR is listed. Three main occupational groups are discerned based on the grouping of ISCO job titles (senior officials and managers, professionals; white-collar-middle = associate professionals, clerks and service workers; blue collar = craft workers, plant and machine operators and assemblers and elementary occupations) [36]. Also, three sectors of employment are discerned: the industrial sector (12 industrial plants), the private services (seven banks and insurance companies or distribution centres) and the public services (six local administrations or hospitals).
Statistical methods
Age-standardized prevalence rates of high TCR per gender were calculated using the direct method with the five-year distribution of the entire male or female cohort as a reference [37]. The chi-square test was then used as an inferential test. Logistic regression analyses in SPSS 10.0 were used to calculate adjusted odds ratio's (OR) comparing the estimated odds of high TCR in the exposure category to the estimated odds in the reference category. Adjustment was made for all mentioned covariates. In view of the large sample size, a level of α = 0.01 was used to indicate statistical significance based on the Wald chi-square test; accordingly 99% confidence intervals (99% CI) were calculated. The effect of the job strain exposure categories in predicting a high versus a low level of TCR was not only evaluated for the standard cut-off points (0.20 in men, 0.10 in women), but also for alternative cut-off points (0.05, 0.10, 0.15, 0.20 in both genders) enabling to evaluate the stability of observed associations.
Results
Associations between total coronary risk and quartiles of job stress scales
Figure 1 depicts the age-standardized prevalence of a ‘high’ level of ‘total coronary risk’ within quartiles of the job stress scales. Only the inverse association between prevalence of ‘high’ TCR and quartile level of job control in men is found to be significant.
Figure 2 pictures for each gender the odds ratios and confidence intervals associated with subsequent exposure levels regarding job demands, job control and social support, adjusting for the effects of one another and for the standard set of covariates. Clearly, from the confidence intervals crossing the null value (OR = 1.0), no significant associations are observed. More particularly, this observation also holds for the association between level of TCR and quartile levels of job control in men. Including exposure to job insecurity (quartiles) into the model does not change the picture (results not shown).
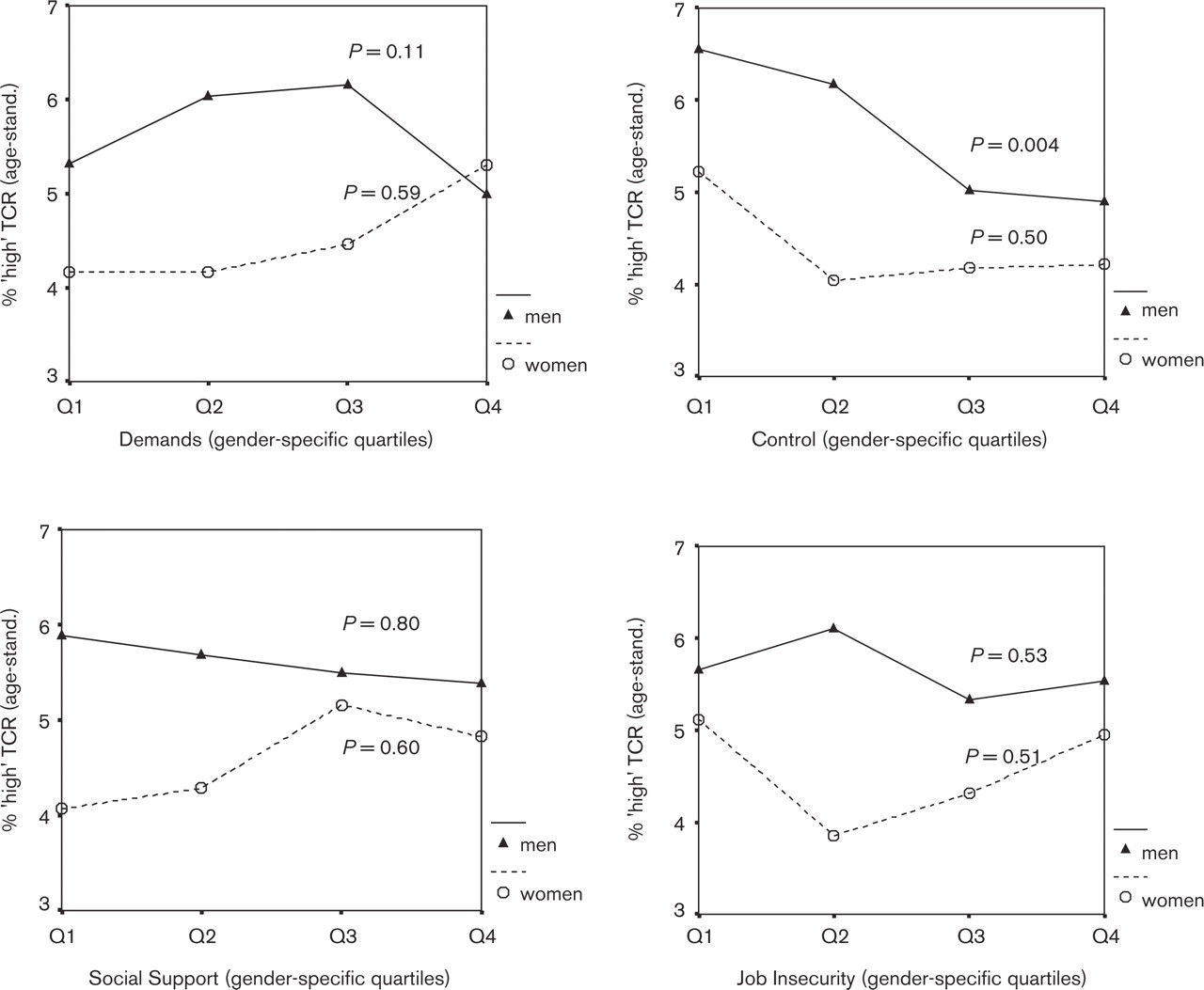
Age-standardized prevalence1 of ‘high’ Total Coronary Risk2 by quartiles of job stress scales per gender. (1) Standardized to the 5-year age distribution of the entire cohort per gender, using the direct method. (2) ‘High’ level of Total Coronary Risk (=10 year CHD risk) is defined as ≥ 0.20 in men and ≥ 0.10 in women.
Associations of total coronary risk and job strain/iso-strain exposure
From Figure 3, a high level of TCR is associated with job strain exposure in men. The highest age-standardized prevalence is observed in the ‘high strain’ exposure group in line with the basic assumption of the job strain model. However, the lowest level is observed in the ‘active’ exposure group though for this group a medium level of TCR was predicted. Again, the suggestion from the figure is mainly that a high level of total coronary risk is more prevalent in workers with a low level of job control (‘passive’ or ‘high strain’ exposure). In women, the association between the age-standardized level of TCR and job strain exposure is not significant, although the highest level again is observed in the high strain group.
Figure 4 presents the association between level of TCR (using the standard cut-off points) and either job strain or iso-strain exposure, equally adjusted for the standard set of socio-demographic covariates. No significant associations are observed. In men for instance, the estimated odds within the model of ‘high TCR’ for workers in a ‘high strain’ job equal 1.26 times the estimated odds for workers in a ‘low strain’ job, but the estimate is rather imprecise containing too large a probability to be 1.0 or even less. Using alternative cut-off points in defining high and low levels of TCR (0.05, 0.10 and 0.15 in men, 0.05, 0.15 and 0.20 in women) does not change the picture, neither in men nor in women (results not shown).
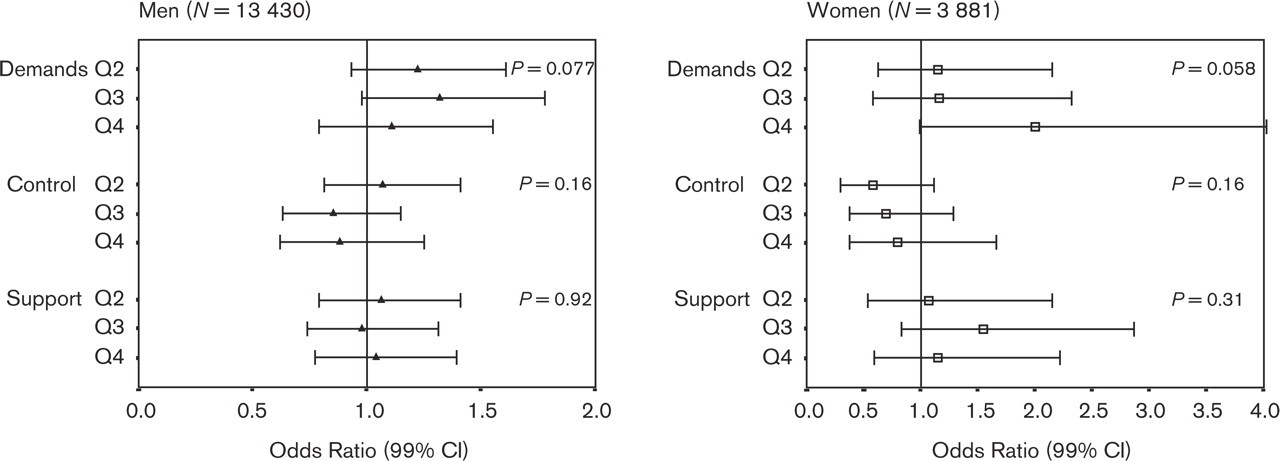
Adjusted association of level of Total Coronary Risk (high vs. low)1 and job stress scale quartiles. Results of logistic regression2, per gender. (1) Standard cut-off points are used, i.e. 0.20 in men and 0.10 in women; high level = 1, low level = 0. (2) The model additionally controls for age, level of education, occupational group and sector of employment. Reference category is Q1 (first quartile) for each scale.
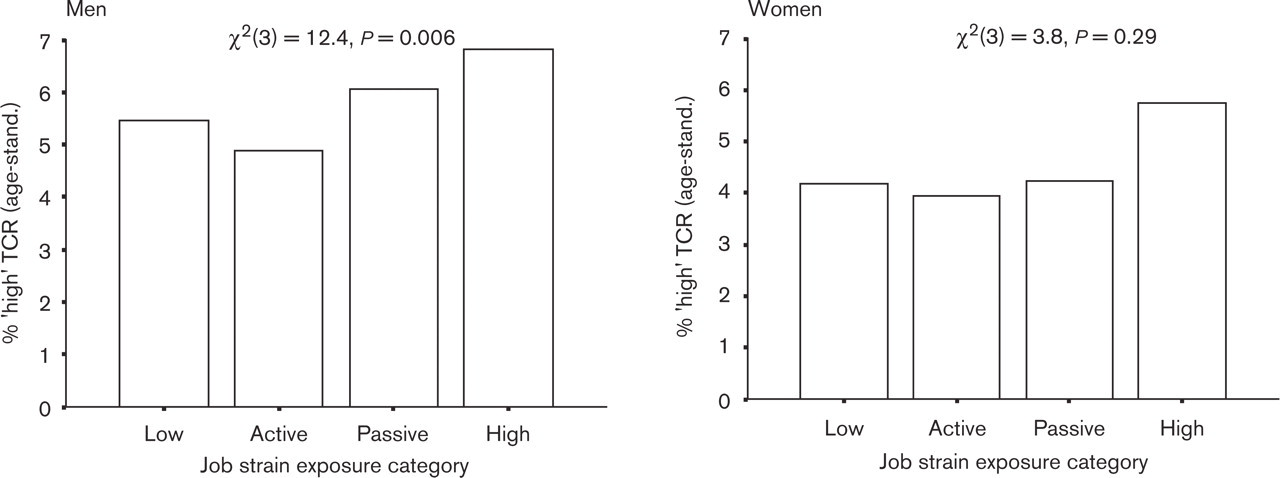
Age-standardized prevalence1 of a high level of Total Coronary Risk2 by job strain exposure group3, per gender. (1) Standardized to the 5-year age distribution of the entire cohort per gender, using the direct method. (2) ‘High’ level of Total Coronary Risk (= 10-year CHD risk) is defined as ≥ 0.20 in men, and ≥ 0.10 in women. (3) ‘Low strain’ = low demands + high control; ‘active’ = high demands + high control; ‘passive’ = low demands + low control; ‘high strain’ = high demands + low control.
The use of the alternative job strain variable with its six exposure categories ranging from ‘extreme low strain’ to ‘extreme high strain', did not point to any significant relationship with level of TCR, whatever its cut-off points. For instance, in the logistic regression model with TCR-levels defined by the standard cut-off points as the outcome and using the alternative job strain exposure variable as a predictor while adjusting for the standard set of socio-demographic covariates, the p value associated with this exposure variable of interest was 0.085 in men and 0.30 in women.
Discussion
Limitations of the study design
Neither the BELSTRESS-cohort nor its large subclass (92%) of subjects without a self-reported personal history of CHD can be considered as representative samples of the Belgian workforce. Although a representative sample and a high response rate are vital in descriptive studies, these characteristics are not considered critical in analytical studies aimed at demonstrating a relationship between exposure and outcome. What matters in the latter group of studies is the substantial variation of the exposure variable under study [38]. For the BELSTRESS-cohort, covering a broad range of occupations, large variations in the job stress scales in line with variations observed in other studies, have been fully described [35].
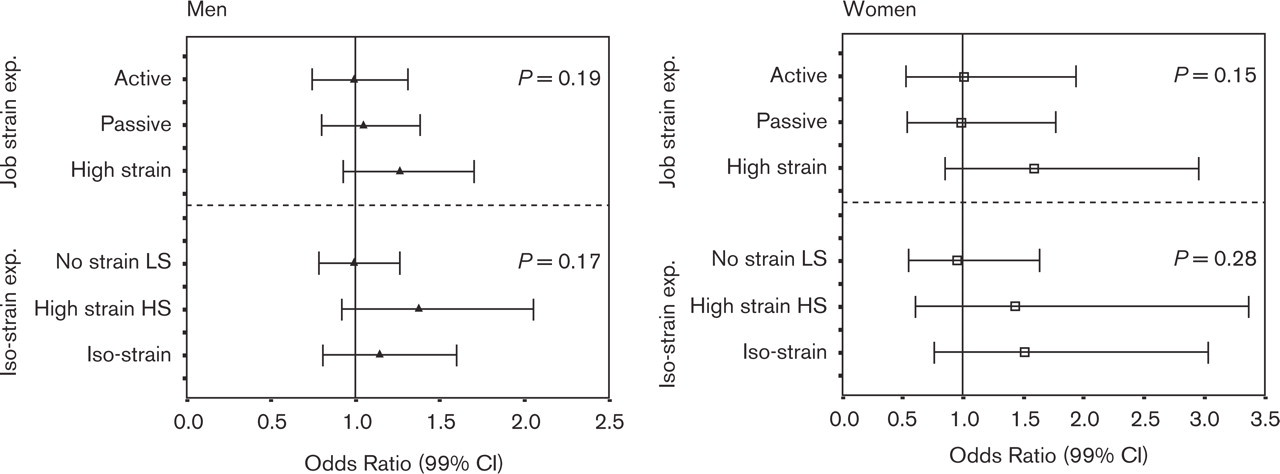
Adjusted association of level of Total Coronary Risk (high vs. low)1 and job strain or iso-strain exposures. Results of logistic regressions2, per gender. (1) Standard cut-off points are used, i.e. 0.20 in men and 0.10 in women; high level=1, low level=0. (2) The model controls for age, level of education, level of occupation and sector of employment. - For ‘job strain’ exposure, the reference category is ‘low strain’ (low demands + high control). - For ‘iso-strain’ exposure, the reference categorie is “no strain HS” with ‘no strain’ (low strain + active + passive) as opposed to ‘high strain’ and with HS=high support, LS=low support.
A more critical objection is that the regrouping of scores in the broad job strain and iso-strain exposure groups according to the median split on the job stress scales has the risk of reducing too much of its variation. In view of the observed dose-response relationship between job strain and myocardial infarction [11], we think this to be a clinching argument. On the other hand, the applied quadrant classification scheme is fairly standard [6, 20] and can be expected to be capable of demonstrating a relationship with health outcomes in a large sample such as the BELSTRESS-cohort. In the realm of psychosocial well-being, with feelings of depression or sleep problems as outcomes, such associations have indeed been demonstrated [8, 39, 40]. Moreover, the use of our alternative job strain variable in the logistic regression model, with its six exposure categories based on one or another combination of quartile groups on the job demands and job control scales, did not point to any significant relationship between this alternative variable and TCR.
Certainly a limitation of this study is its cross-sectional design, although it shares this feature with many other studies on the relationship between job strain and blood pressure or hypertension [14]. Cross-sectional designs generally are subject to information or selection bias if the exposure variable is liable to change over time [41]. In the workplace setting, it is quite conceivable that particularly subjects employed in a high-strain job will tend to move, in due time, to a low-strain or to a more passive type of job. For instance, a recent study among women found that twice as many women among those exposed to high strain jobs (23.8%) at time T1 had moved to another job at time T2 than among women exposed to low strain jobs (12.4%) at T1 (p = 0.003) [42]. The example points to what may be coined as the ‘high strain worker effect', that is, the tendency among high strain workers to change jobs more often than non-high strain workers.
Prevalence studies moreover do not properly account for lag-time effects. If it needs time until adverse health effects of job stressors become apparent, workers in a high strain job today may still have a good health status while workers who have changed from a high strain to a low strain job may already suffer from adverse health effects. It is clear that this would add to the underestimation of the association between psychosocial work characteristics and health status indicators as well. Far better approaches indeed are longitudinal studies. Consecutive screening rounds in the same individuals may then facilitate discrimination between workers consistently scoring high on the job stress scales and those only incidentally scoring high and see how this is related with health effects in due time. This approach also enlarges the variation in the exposure variable, which may add to the detecting of health effects that need time to develop.
Concept of ‘total coronary risk'
The Framingham risk function assessing the ‘absolute risk’ to develop CHD has certain limitations as well. The function is based on a high-risk middle-aged (30-74 years) North American population and its application to European populations may pose a problem [26, 27]. More particularly, the function tends to overestimate absolute risks in low-risk populations. Ideally, the risk function and derived risk charts for use in clinical practice should be based on results of prospective cohort studies assessing the distribution of CHD risk factors in the population to which these charts are to be applied [26]. Until now, no such function has been derived for the Belgian population. In Belgium, the available figures of coronary mortality and morbidity are, on the whole, still very high although decreasing trends over the past three decades are observed [29, 43]. Far more important for our study however is that the estimates of relative risk positioning an individual within his group on the basis of the Framingham equation are likely to be quite robust for all European populations [26]. A more serious problem certainly is that our measure of ‘total coronary risk’ based on the Framingham function does not take into account the typical risk factors that have been shown in the literature to be related to job strain exposure in a consistent way. More particularly, ambulatory rather than casual (systolic) blood pressure [13, 44] and smoking intensity rather then smoking status have been reported to be of far greater prognostic value [13]. On the other hand, serum cholesterol levels are included in the equation but these generally are not reported to be related to workplace stressors. Left ventricle hypertrophy finally is very rare in our study cohort. For that matter, the composite measure may lack ability or rather sensitivity to account for significant changes in coronary risks due to changes in working conditions.
Other risk factors
The above mentioned limitations may well account for our failure to find that high job strain may impact on conventional coronary risk factors. This however notwithstanding, we need to address the possibility that the increased risk of developing CHD is not only mediated by the ‘classical’ risk factors, but alternatively, is also mediated by other factors, which in turn might be related to job stress conditions. One prominent factor is plasma fibrinogen for which a significant association with CHD-incidence has consistently been observed [45–48]. Some studies indeed are suggestive of a link between elevated fibrinogen levels and exposure to job related stress. For instance, in a cross-sectional study among employed Danish men and women, a clear association was found between elevated plasma fibrinogen levels and high job strain [25]. A more recent Swedish study reports a positive association between ‘inferred’ job strain but not between ‘self-reported’ job strain and fibrinogen [49]. Among German managers, fibrinogen was associated with a combination of over-commitment to the job and lack of workplace social support [50]. In the longitudinal Whitehall II study among British civil servants, elevated fibrinogen levels were found to be associated with low job control [51]. In the BELSTRESS-cohort, a positive statistically significant association was also observed between job strain and plasma fibrinogen, though generally only in males. After stratification for educational level, the association became significant also for females in the middle educational level [52]. By contrast, null findings on the relationship between fibrinogen and job strain have been reported as well [53, 54]. More recently, evidence was also provided that high-sensitivity C-reactive protein (CRP), an inflammatory biomarker, may play a role in the development of CHD [55, 56]. In a specific sample of 892 healthy men of the BELSTRESS-cohort, we however did not observe any significant relationship between CRP and levels on the applied job stress scales [57]. Much additional research will therefore be needed in this area before definite conclusions can be reached. Apart from that, the interplay between workrelated stress and family responsibilities also needs attention. In a Quebec-Canadian study among whitecollar women, it was shown for instance that the combined exposure to large family responsibilities and high strain tended to have a much greater effect on ambulatory blood pressure than exposure to either one of these factors. These joint effects were particularly significant in women holding a university degree and lasted during the workday, in the evening and at night [14]. Effects of conditions and roles outside work are assumed to be of particular importance for women, as it has been observed that women experience more stress at home than men [58].
Conclusion
The separate job stress scales and the quadrant definitions of job strain and iso-strain do not display significant associations with the applied composite measure of ‘total coronary risk’ based on a Framingham equation, after adjustment is made for potential socio-demographic confounders. The limitations of our cross-sectional study in a working population, free of a self-reported personal history of CHD, however is acknowledged. A study design that allows one to evaluate prolonged exposure to job strain, preferably in conjunction with measurements of exposure to stress factors outside work, is called for.
Footnotes
Acknowledgements
The BELSTRESS study was supported by a grant from the Federal Office for Scientific, Technical and Cultural Affairs, Belgium (ST/02/007). Edwin Pelfrene was supported by a fellowship from the Fund for Scientific Research (F.W.O.-Vlaanderen, Belgium).