
Abstract
Aims
The intention of this study is to investigate the relationship of the demands/control/strain model with hard coronary events in an epidemiological, prospective, multicenter, European study.
Methods and results
Six cohorts (Brussels, Ghent, Lille, Barcelona, Göteborg and Malmö) from four European countries (Belgium, France, Spain and Sweden) consisting of 21 111 middle-aged male subjects participated between 1993 and 1996 in the baseline survey of the Job Stress, Absenteeism and Coronary Heart Disease in Europe (JACE) study. The Karasek strain model of psychological demands (five items)/control (nine items) was used. During a mean follow-up of 40 months 185 acute coronary events or coronary deaths were observed. Age-adjusted hazard ratios (HRs) for developing an acute coronary event were 1.46 [CI 95% confidence interval (1.08–1.97)] for high against low psychological demands and 1.53 (95% CI 1.0–2.35) for strained (high demands plus low control) against relaxed (low demands plus high control) groups. After adjustment for standard cardiovascular risk factors the HR for developing a coronary event for those above or equal to the median against those below the median of psychological demands was 1.46 (95% CI 1.08–1.97) whereas the HR for strained against relaxed groups is 1.46 (95% CI 0.96–2.25). Sensitivity analyses confirmed the robustness of the results.
Conclusion
In this European, multicenter, prospective, epidemiological study the Karasek job strain model was an independent predictor of acute coronary events, with the psychological demands scale emerging as the important component.
Keywords
Introduction
The terms strain and stress were coined by engineers and physicists in the nineteenth century and have exact measurable definitions which predict deformation of different materials by strain gauges. Later on when applied to the biological and mainly psychosocial sciences the terms became more vague although two models emerged in the twentieth century: the ‘fight or flight’ concept proposed by W. Cannon in 1929 [1] and the general adaptation syndrome by H. Selye in 1936 [2].
The latter linked various pathologies including atherothrombotic cardiovascular diseases to physiopathological activities of the autonomic nervous system and the adrenals.
Empirical studies proposing pathogenetic mechanisms were already published three to five decades ago [3–6]. Moreover possible associations between life stress and cardiovascular disease were already proposed by H.G. Wolff [7] and I.G. Stewart [8] more than five decades ago.
The sociological basis of stress was outlined by French and colleagues in 1970 through the ‘person/environmental fit’ concept [9].
The general life stress concept evolved to that of occupational or job stress in the 1980s. In 1980 a paper observed a possible independent contribution of occupational stress to incidence of major coronary events by ecological comparison of a Belgian public sector low strain savings bank and a high strain private bank [10, 11]. Subsequently two sociologists, R. Karasek from the US and J. Siegrist from Germany, proposed psycho-sociobiological models linking job stress to coronary heart disease (CHD). The former introduced the demands/control model which postulated that high psychological job demands together with low job control (a combination of decision authority and skill discretion) would lead to job strain [12], whereas the latter proposed that job strain is the result of perceived imbalance between efforts at work and reward [13].
The success of the Karasek model is probably due to the fact that it is basically simple, has a high face validity and has been found to be at least partly supported by a number of empirical studies in the fields of epidemiology, psychophysiology and organizational health psychology.
Extensive reviews have been published on the basis of available evidence: Schnall et al. [14] was the first to make an extensive review in 1994. Kuper et al. [15] made a systematic review of psychosocial factors in the etiology and prognosis of CHD and found that out of 13 studies investigating psychosocial work characteristics, 10 observed a strong or moderate association with CHD. Noteworthy is that some only found an inverse relationship with one or the other of the Karasek scales, either psychological demands or job control. The most recent review on the Karasek model, which also included an assessment of a methodological quality of the studies, was published in 2004 [16].
Thus although the epidemiological observational body of evidence linking job strain with CHD is growing, there is still a lack of coherence in the reported results.
In 1995 the European Union funded a study known as Job Stress Absenteeism and Coronary Heart Disease: European Cooperative Study, or the JACE study. This is to our knowledge the first European multicenter prospective study testing the Karasek model. The study was carried out in six centers spread over four countries in Europe.
Materials and methods
The design of the study has already been reported extensively [17, 18].
Organization of the study
The JACE study is a Biomed I concerted action. The JACE group consists of eight participating centers from six countries: Belgium (two centers), France, Italy, Spain, Sweden (two centers) and The Netherlands. The coordination of the study is in Brussels (School of Public Heath; Brussels Free University). The Leiden group, although part of the JACE group, did not contribute to the myocardial infarction (MI) incidence study as no specific follow-up had been planned [17, 18].
The Milan center participated with a single cohort of municipal employees, mostly female. Two different Job Content Questionnaire versions were adopted in subsequent time periods, the second to comply with JACE requirements. Due to these restrictions, already cautioned against in the final report of the JACE Study sent to the Directorate General XII of the EEC [19] as well as the low number of MI events (the effect of the combination of the low incidence MI rate in the Italian population and the very short follow-up) it was decided at the start not to include this cohort in the JACE-MI substudy.
Thus we present here results from six European centers in four countries: Brussels and Ghent (Belgium), Barcelona (Spain), Lille (France) and Malmö/Göteborg (Sweden).
Choice of populations for the study and samples sizes
Barcelona, Göteborg and Malmö used a population sample out of which only those at work were included in the present study. The three remaining centers recruited men employed in a wide variety of occupations and industries. All subjects on the payroll working full or part time were invited to participate. Fields of activity included, among others, manufacturing, power supply, car assembly, municipal employees, healthcare, postal service, insurance and banking and the chemical industry.
Only men were included in the JACE-MI incidence study as the study was not statistically powered to do similar analyses in the 11 419 women who participated in the project due to a much lower incidence of major CHD events, as outlined in the design papers [17, 18].
Questionnaires were self-administered except in Barcelona where they were all administered by an interviewer due to functional literacy problems.
Men aged 35–59 years were screened for the core study.
The participation rate varied across centers from a low 38% in Malmö and 45% in Brussels to a high 73% in Barcelona with intermediary figures for Göteborg (64%) and Ghent (65%).
Study design
This concerted action applies a prospective study design with an average follow-up of 40 months for incidence of acute coronary events.
The questionnaires
In the core questionnaire the following information was collected.
Sociodemographic
Along with age, the following sociodemographic data were recorded.
Occupations were coded in each center using the International Standard Classification of Occupations (ISCO)-88 classification [20]. For practical reasons, however, full precision coding (four digits) could not be attained in every center, thus one digit coding was considered as the lowest common denominator. Between-center quality control was regularly assessed by comparing ISCO-88 codes assigned to a sample of 20 occupations. Kappa agreement between six centers was 79.6% (precision, two digits).
Three levels of education were standardized across the six centers using the MONICA questionnaire [21].
Smoking habits were recorded using the MONICA survey questionnaire [21].
Job content questionnaire
Two key scales were available in all centers, namely, psychological demands (five questions) and decision latitude (nine questions) enabling us to allocate participants to each of the four quadrants defined by the combination of those two dimensions [22, 23]. Four groups were considered: participants under strain (i.e. scoring above or equal the median for demand and below the median for control). Relaxed subjects (below median for psychological demands and above or equal the median for control), active subjects (above or equal the median both for demands and control) and passive subjects (below the median both for psychological demands and control). Because Malmö had different response options for the same questions a calibration study was conducted in a sub-sample using the two questionnaires, which allowed scores to be converted (R. Karasek, in preparation). All medians were center and ISCO specific. The questionnaire was translated from English-American to Swedish, Dutch, French, and Spanish versions and then back-translated to English to assess the semantic equivalence of the different versions. Validity and reliability of the scales were studied for the Dutch, French and Spanish versions of the questionnaire [24–26].
Missing value replacement
Whenever at most one item happened to be missing per scale (i.e. one of five for demand and/or one of nine for control) this item was attributed the mean value of other items for that dimension in the same individual [27].
For prevalent CHD at baseline one standardized question recorded hospitalization for CHD in four centers.
Clinical and biological measures
For each participant a single standardized screening visit was organized in order to obtain data on height and weight, arterial blood pressure and total serum cholesterol. The Malmö center had serum cholesterol measured only in part of their cohort.
The Ghent center co-ordinated the quality control of the lipid measures which were all sent to an external quality control system. The measurement of blood total and HDL cholesterol was part of the core program of JACE. In the core protocol and in the manual of operations recommendations were given regarding the procedure of venous puncture, serum handling and preservation. Particular emphasis was given to the sequence of filling the vacutainers, to the position of the participant during venous puncture and to the use of the tourniquet. Furthermore, the laboratories were requested to provide results from an external quality control system either with the lipid reference center of the World Health Organization in Prague or with the US Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia. The results concerning the external quality control of total cholesterol measurements (coefficients of variation and biases) were all within the acceptable criteria in three centers. In two other centers the coefficients of variation exceeded sporadically the acceptable criteria.
Blood pressure was taken in a standardized manner based on the MONICA project manual [21]: in a sitting position on the right arm, after 5 min rest. The mean of two measures was recorded.
Follow-up
The main events were nonfatal and fatal MI as well as sudden cardiac death. The Belgian arm also included procedures of revascularization during hospitalization for an acute coronary event. Follow-up ended in all centers on 31 December 1999.
Detection of acute coronary events
Brussels, Ghent and Lille
Sickness absences of 28 days or more were reported by the department of human resources. General practitioners (GPs) were contacted, and, for all hospitalized participants with a suspicion of CHD, records were retrieved in order to confirm an acute MI or acute percutaneous transluminal coronary angioplasty or coronary artery bypass grafting during a hospitalization for an acute coronary event. All deaths were communicated by the department of human resources and diagnosis given by hospital records or GPs. Sudden deaths without a clinical diagnosis were considered as coronary deaths.
Barcelona
All participants of the JACE study were contacted by phone with a short questionnaire on hospitalization. Record linkage was also made of all JACE cohort members with the MONICA register and the mortality register from the Department of Health.
Malmö
All Malmö deaths were linked to the JACE cohort and International Classification of Diseases code 410 (8 and 9e revision) was included as an MI; nonfatal MI was detected by the Malmö Myocardial Infarction Register from the Malmö University Hospital, the only hospital in the city for acute MI patients [28].
Göteborg
All fatal events were found through the national central register on deaths and nonfatal events were detected through the national Swedish hospital register, which has very few misses.
Although different techniques of detection were used all were deemed exhaustive and finally all CHD deaths and nonfatal acute coronary events were validated through MONICA criteria.
Statistical analyses
The statistical power of the study was computed from the control group of the Belgian Heart Disease Prevention Project, a factory randomized trial from the 1970s. On the basis of an observed incidence of 2.5 per 1000 patients-years in the middle-aged male working population a sample of 15 000 men would detect a Risk Ratio (RR) of 1.8 between extreme tertiles with 80% power at the α = 0.05 confidence level [29].
Job demand and job control scores were dichotomized between under p50 and p50 or greater. Owing to the differences of distribution of job titles across centers, computations of medians were center and ISCO specific (stratification for three ISCO groups at the one digit level of precision, i.e. ISCO 1 + 2 + 3, 4 + 5 + 6 and 7 + 8 + 9).
Job strain construct was designed as follows: subjects scoring < p50 for demand and ≥ p50 for control were the reference category (relaxed); subjects scoring < p50 for demand and < p50 for control formed the passive group; subjects scoring ≥ p50 for demand and ≥ p50 for control were defined as the active group; and eventually, subjects scoring ≥ p50 for demand and < p50 for control formed the strained group.
In univariate analysis, log-rank and Breslow χ2 tests were computed to test the difference between Kaplan-Meier survival probabilities between job stress categories.
The Cox proportional hazard model was used to study the association between, respectively, baseline job demand, job control and job strain with the incidence of fatal and nonfatal acute coronary events.
Models were adjusted for age (continuous) and two coronary risk factors: smoking (current versus never plus ex-smokers) and systolic blood pressure (continuous). Effect of further adjustment for serum cholesterol or prevalence of CHD was performed on subsets of the database where those data were available.
Exposure variables and other covariables were entered in one block. Dummy indicators were used to represent each categorical variable.
Proportional hazard assumptions were assessed graphically by inspection of the -ln(−ln S(t)) survival curves for every variable included in the models.
The interaction terms job stress factor × center was tested in every model to check whether pooling data across centers was appropriate.
Results
Table 1 shows the screening period and some characteristics of the six centers. The total number of subjects was 21 111 and 185 hard coronary events occurred during a mean and median follow-up of 40.1 and 39.2 (interquartile range 20.7) months respectively.
Participating centers and incidence of hard coronary events
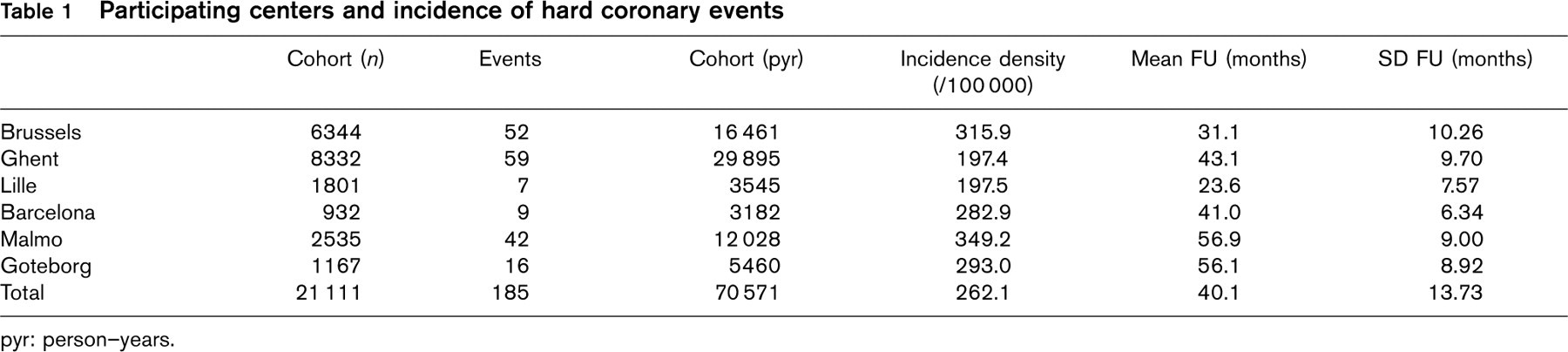
pyr: person–years.
Age ranges, International Standard Classification of Occupations (ISCO) categories and incidence of hard coronary events
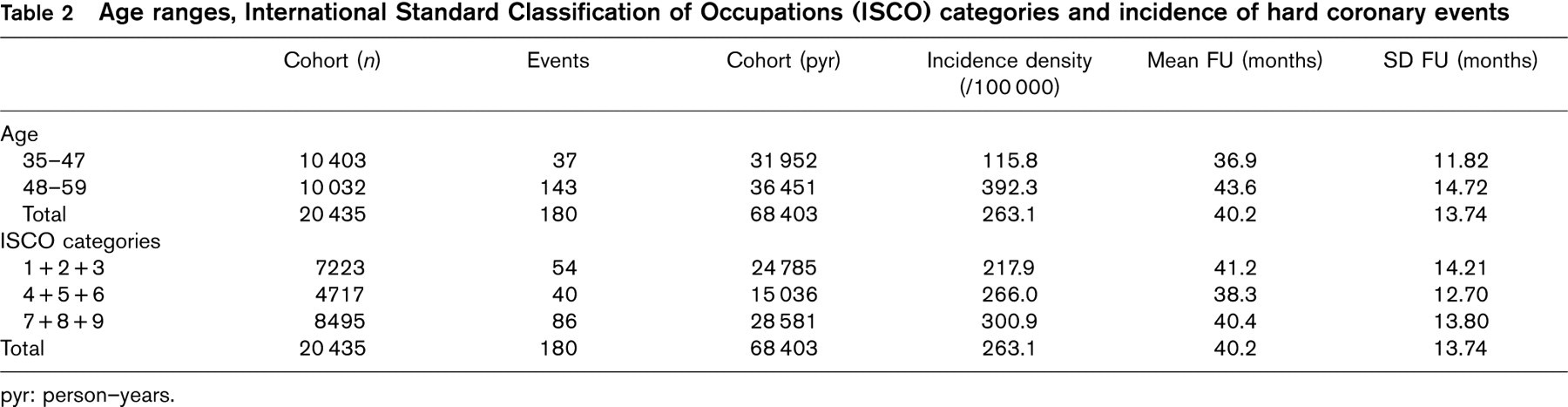
pyr: person–years.
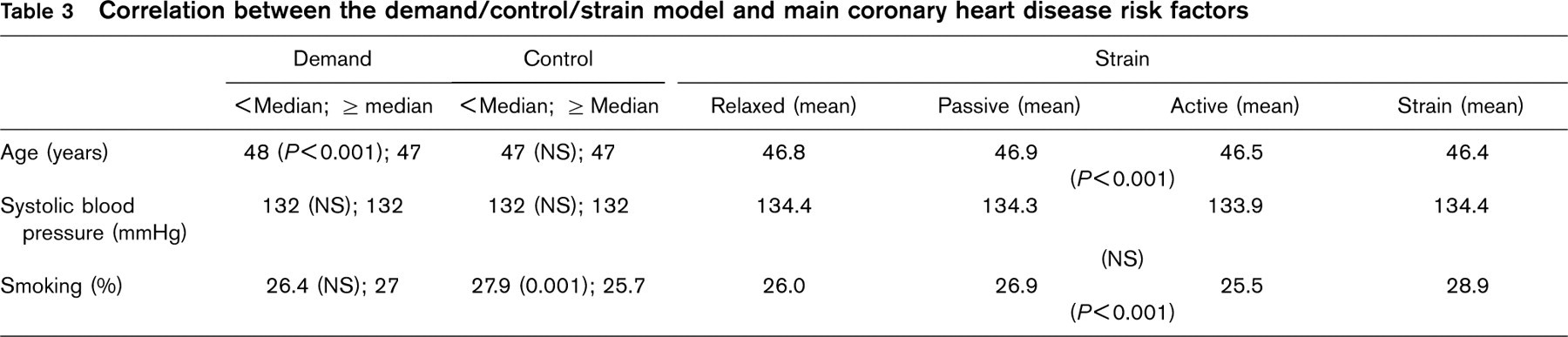
Correlation between the demand/control/strain model and main coronary heart disease risk factors
The incidence density was highest in the Malmo and Brussels, lower in Barcelona and Goteborg and the lowest in Ghent and Lille.
The incidence rate was related to age and inversely related to socio-professional level defined by ISCO categories (Table 2). Table 3 shows the correlation of baseline CHD risk factors and the Karasek model; as can be seen there are small differences in age and smoking behavior as related to psychological demands and quadrants of the strain model, that warrants multivariate adjustments.
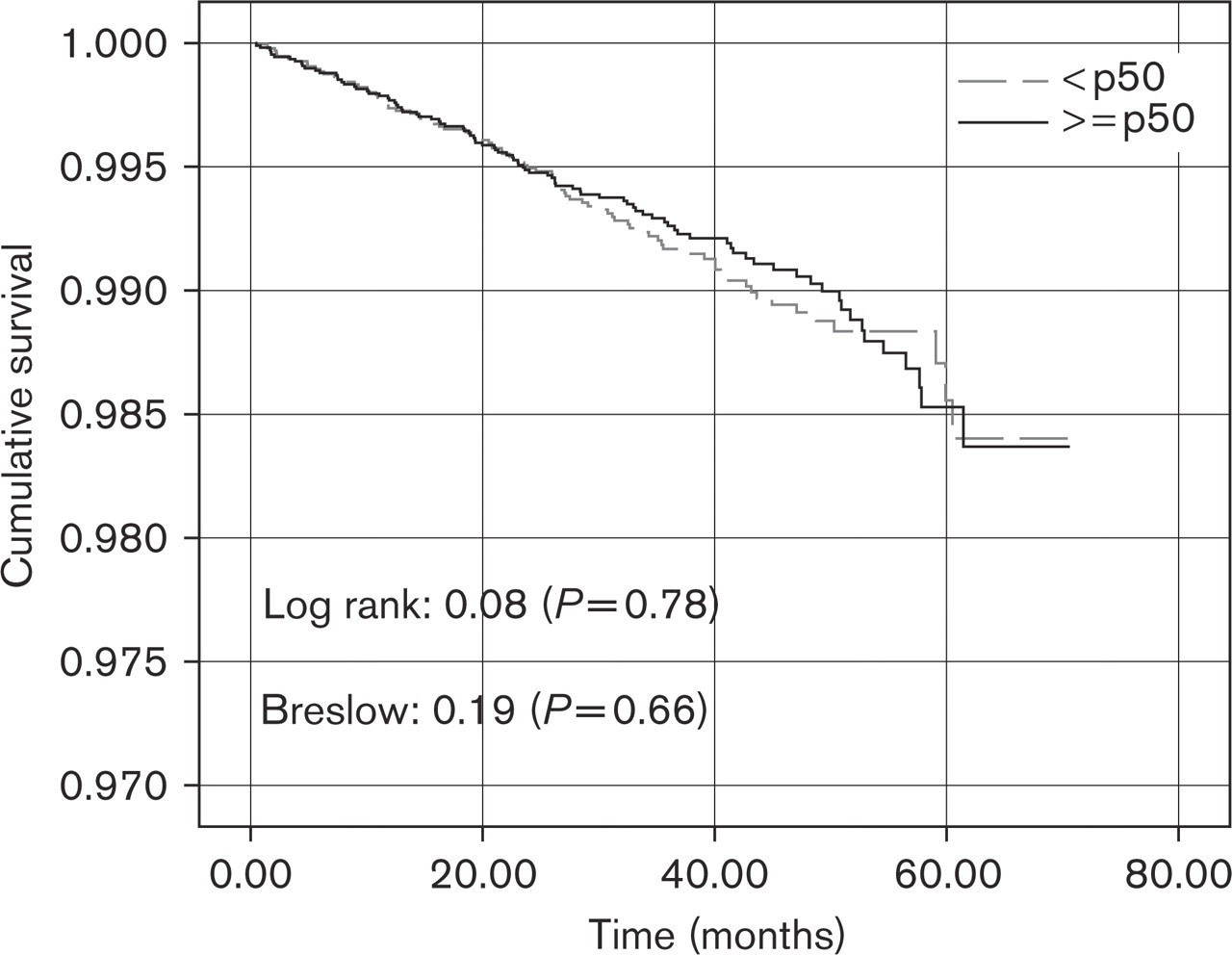
Kaplan–Meier survival curves show a significant shorter survival without event for subjects above or equal the median as compared with those below the median for psychological demands for both the log rank and Breslow tests (Fig. 1). No associations were observed with job control (Fig. 2). As compared to these subjects defined as ‘relaxed’ (low demands and high control), those defined as strained (high demands and low control) show a significantly shorter survival without events by both the log rank and Breslow tests (Fig. 3).
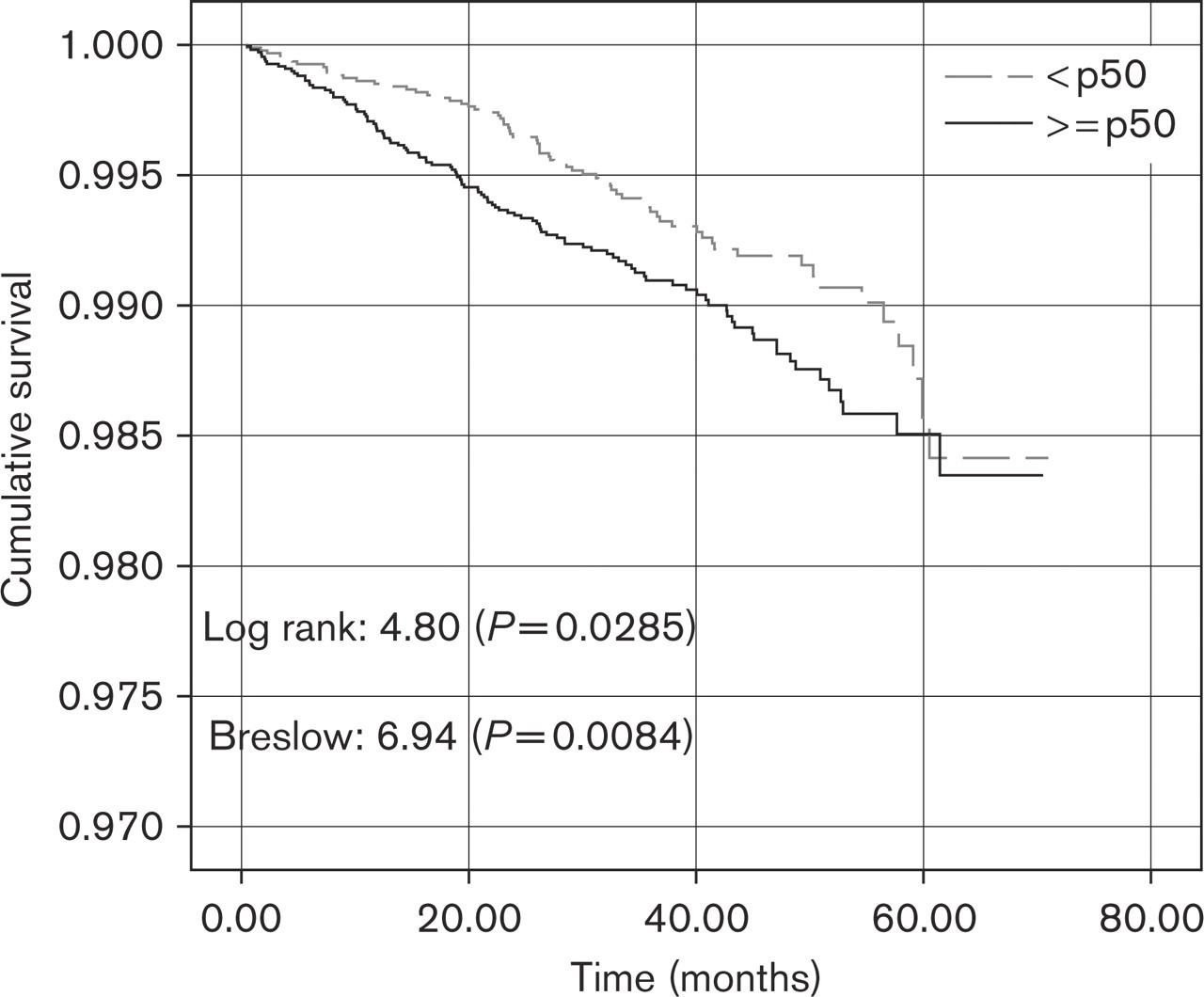
Survival curves of coronary heart disease incidence and baseline psychological demands.
Survival curves of coronary heart disease incidence and baseline control.
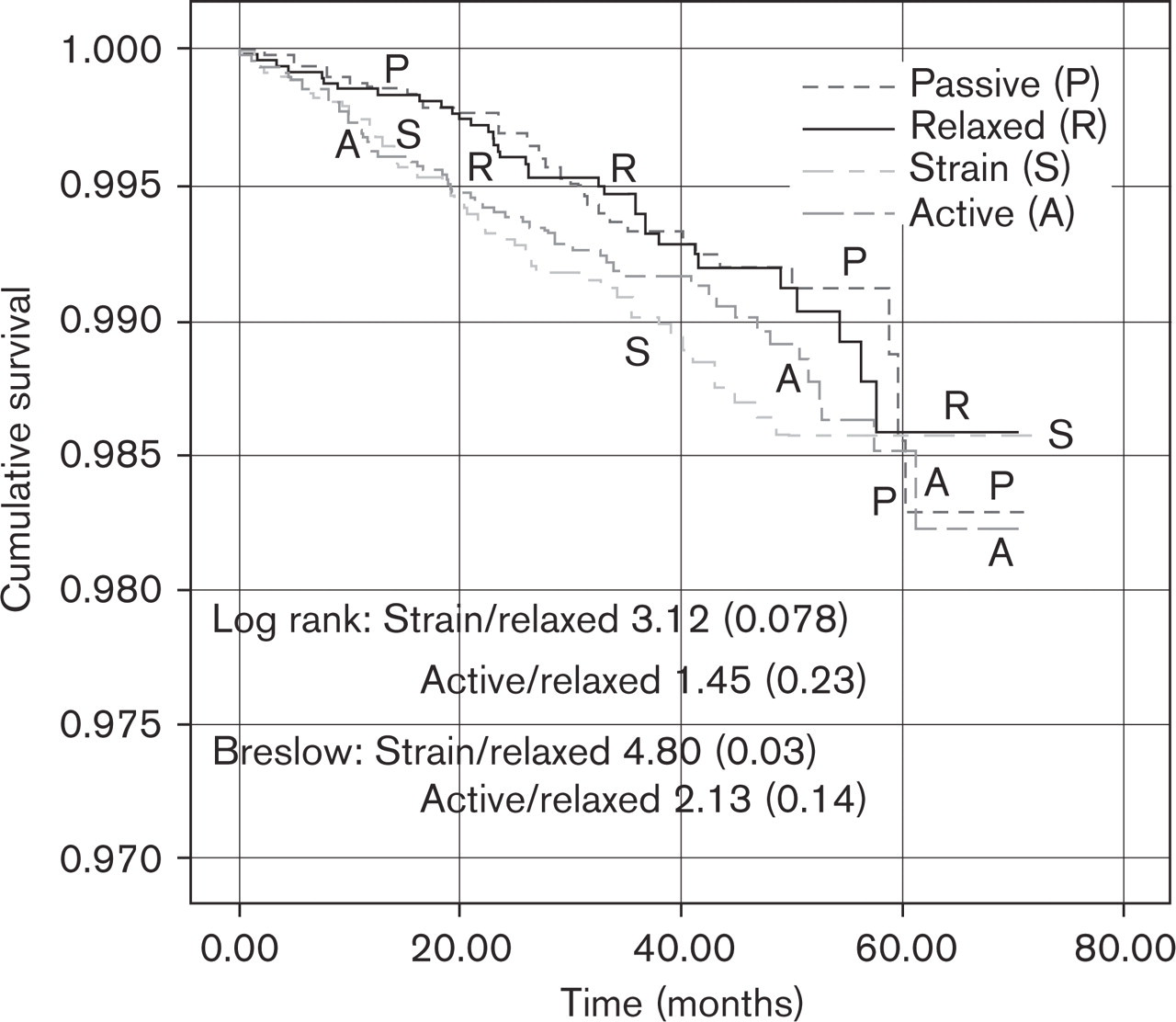
Survival curves of CHD incidence and baseline Relaxed/Active/Passive/Strain status.
When adjustments were made for age, smoking and systolic blood pressure, subjects above the median for psychological demands and those defined as job strained as compared with those below the median for demands and those defined as relaxed, show higher event rates with hazard ratios (HRs) of 1.46 [95% confidence interval (CI) 1.08–1.97] and 1.46 (95% CI 0.96–2.25) respectively, whereas a test of heterogeneity between centers was not statistically significant for psychological demands but significant for job strain (Table 4).
When demands and control were introduced as continuous variables in the Cox model along with the interaction term demands × control none of these variables proved to be significantly associated with acute coronary events (results nor shown).
Sensitivity analyses
The Malmö center had serum cholesterol measured at baseline survey in 1076 out of 2535 subjects. Multivariate analyses were performed adding serum cholesterol, thus reducing the number of events from 185 to 157. The HR for psychological demands (above or equal the median/below the median) was 1.32 (95% CI 0.96–1.81) the P for interaction between centers being nonsignificant; the HR for strain (strain/relaxed) was 1.34 (95% CI 0.86–2.10) again without a significant interaction between centers.
Only four cohorts had a standardized question on previous hospitalization for a major coronary event: Brussels, Ghent, Barcelona and Goteborg.
Excluding those who had a hospitalization for a major coronary event before the baseline survey reduced the number of events to 129. Again after adjusting for age, systolic blood pressure and smoking, the HRs for those free of non-silent major CHD events at baseline were 1.42 (95% CI 1.00–2.03) and 1.44 (95% CI 0.89–2.33) for psychological demands (high/low) and strain (strain/relaxed), respectively.
When stratifying for level of education the HRs for high against low psychological demands were 1.46, 1.27 and 2.50 for lower, middle and higher level of education, respectively; for job strain (strain/relaxed), those HRs were 1.10 and 1.77 for lower and middle education level, whereas the model did not fit for higher education (too few events).
Discussion
In this multicenter European prospective study with an average follow-up of 40 months high psychological job demands as well as job strain were independent predictors of acute coronary events taking age, smoking habits and blood pressure into account with some degree of heterogeneity. Sensitivity tests show the results to be robust in men free of major CHD events at baseline as well as in a multivariate analysis adding serum cholesterol.
For more than four decades different pathogenetic mechanisms have been proposed linking stress or alternatively job strain to coronary heart disease: decrease of coagulation time [5], increase of coagulation factors VII and VIII as well as adenosine diphosphate-induced platelet activation [30], increased platelet aggregation [31], increased blood fibrinogen [32, 33], alteration of lipid metabolism with increased apolipoprotein B and triglyceridemia [34], exaggerated vascular resistance responses during experimental laboratory stress, a marker of endothelial dysfunction [35], endocrine disturbances with increased hormone excretion along the corticotropic releasing factor (CRF) pathway and increase of ACTH secretion and stimulation of the adrenal cortex and increased sympathetic nervous system activity with increased catecholamine excretion by the adrenal medulla due to hypothalamic arousal. These disturbances would lead to accumulation of visceral fat, which is a precursor of the insulin resistance syndrome, which, in turn, is a CHD risk factor [36]. Decreased cellular immunity [37] and increase of the proinflammatory cytokine interleukin-6, which also stimulates the hypothalamic pituitary adrenal axis [38] and leads to an increased ambulatory blood pressure during working hours [39, 40].
Multivariate Cox regression analyses
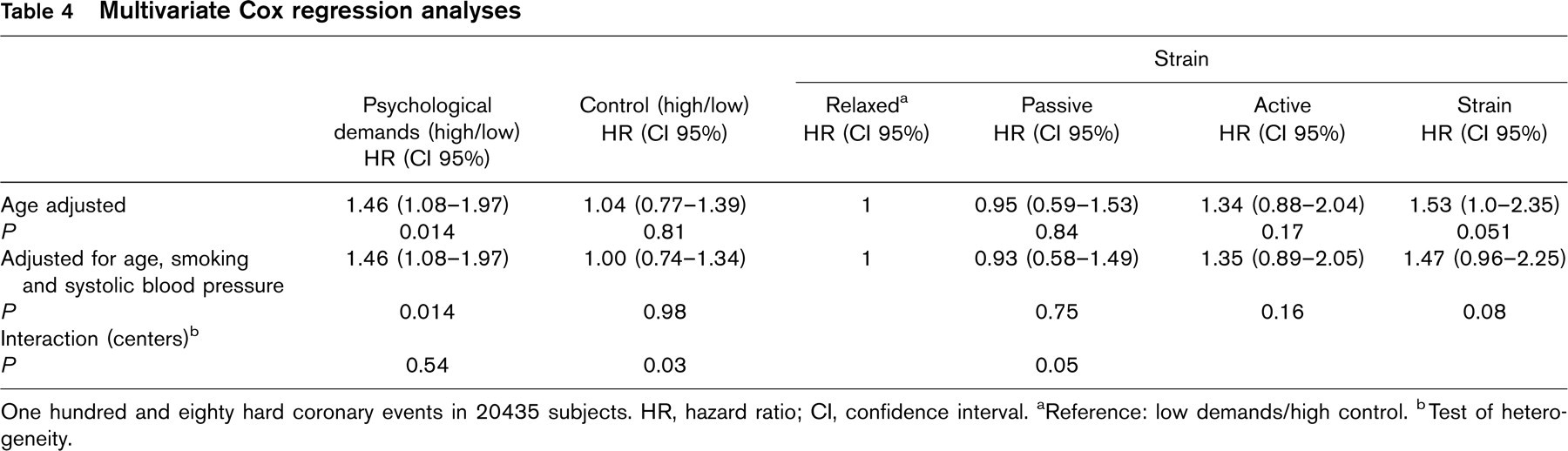
One hundred and eighty hard coronary events in 20435 subjects. HR, hazard ratio; CI, confidence interval.
aReference: low demands/high control.
bTest of heterogeneity.
Experimental [41] and observational studies in dominant and subordinated baboons [42] add some arguments concerning the biological plausibility linking psychosocial stress with CHD.
Finally evolution of carotid intima–media thickness over a 4-year period correlates with baseline psychological job demands [43].
Although the search for new risk factors for coronary heart disease has been claimed to be ‘occupational therapy for epidemiologists’ given that the main CHD risk factors satisfy public health criteria for causality and explain at least 75% of new cases of CHD [44] research on psychosocial risk factors for CHD receive increasing attention by interdisciplinary research between sociologists, psychologists and epidemiologists [15, 45].
Psychosocial characteristics at work have lately been an object of research at the bench, clinical and epidemiological level. Sociologists like to propose ‘models’ and it was to the merit of R. Karasek to come forward with a questionnaire asking for psychological demands and decisions latitude at the work site. The high demand/low decision latitude became the ‘job strain model’ [12]. The third scale, the so-called buffer scale of social support at work was added later [46]. The job title covering type of work performed would put groups of subjects within the working force into one of four possible quadrants: low demands/high decision latitude or relaxed subjects; low demands/low decision latitude or passive subjects; high demands/high decision latitude or active subjects and finally high demands/low decision latitude or strained subjects.
Taking the mean for each scale for each job title a so-called ‘imputation method’ could be used in order to perform post-hoc longitudinal studies [47–51].
Psychologists and epidemiologists starting de novo epidemiological research on job stress used a self-administered questionnaire giving ‘perceived’ psychological demands, decision latitude and strain at the work place.
Thus two different techniques are used with the Karasek model, a possible cause for divergent results and indeed two decades of research using that model empirically have not yet given a clear-cut answer related to the criteria of causal inference as used in observational epidemiology: temporality, power of association, gradation, coherence and biological plausibility.
Endpoints vary from all cause mortality [52, 53], cardiovascular mortality [51] and coronary mortality [47] to incidence of both soft and hard CHD events [27, 54]. Design varies from case–referent [55–57] to prospective cohort studies in civil servants [27], industry [58–60] or random population samples [61, 62].
In case-referent studies, cases present a survival bias including only those reaching the hospital alive and well enough to participate to the study except when the imputation method is used. Another problem is a possible reporting bias, cases perceiving a link between the CHD event and job strain.
For controls memory bias such as ‘forgetfulness’ could play a role.
Another reporting bias is related to the inclusion of self-reported angina, a soft endpoint as an event [27]. As pointed out by Macleod, the results from a Scottish prospective cohort study show only a subjective soft endpoint, angina, to be related to perceived job stress but not admission for MI in hospital [63]. The same was also observed by Hollis et al. in the Multiple Risk Factor Intervention Trial (MRFIT) [64]. When reporting the results of the same cohort at 5.3 years follow-up [65] and 11 years follow-up [66] endpoints are predicted by low job control at the first follow-up and later only by high psychological demands respectively: again hard CHD events are not predicted by the strain model in adjusted models.
The demand/decision latitude instrument has nine or alternatively five items for psychological demands and nine items for decision latitude. Published results show a variety of modifications of the instrument both in number of items used [50, 67] or modifications to the instrument by self-made new items [27, 59].
Given all these observations no wonder conflicting results are the hallmark of all reviews, the latest one by Belkic et al. [16].
In that review only seven out of 15 longitudinal studies confirm the working hypothesis concerning the job strain model or one of the scales as predictors of CHD [46, 50, 59, 67–69] as well as six out of nine case–referent studies [55, 70–74], or all together 54% (13/24) leaving room for speculation.
Lately a return to a more general concept of objective stressful situations of life or those perceived as such gained momentum with results from two Swedish studies [61, 75] and the impressive Interheart study [76].
Whereas many pathogenetic mechanisms propose one or several links between psychosocial stress or more specifically job-strain and incidence of CHD, results from empirical epidemiological literature using the proposed high demand/low control model are rather ambiguous or incoherent for reasons already outlined. The alternative view would be to use one or two simple questions concerning perceived stress at and out of the work setting as proposed by Wilhelmsen and Rosengren [61, 77] in Göteborg population studies. The recent INTERHEART study tapped into this idea assessing psychological stress with two single-item questions relating to stress at work and home in a very large retrospective case–control study from 52 countries in both sexes; compared to ‘never stress at work’ those men perceiving permanent work stress had an odds ratio for nonfatal MI of 2.34 (99% CI 1.87–2.93) with a population attributable risk of 9% (1–18%) [76]. The same empirical approach with chronic stress based on a score of two items prevailed in the Malmö Preventive Project in a cohort of 13 609 subjects (2741 women) with a median follow-up of 21 years [75]. In the male cohort the fully adjusted RR for incident fatal plus non-fatal CHD was 1.17 (1.02–1.33) [75]. In terms of CHD prevention the two different approaches have important implications. Indeed when using a preconceived model, such as the Karasek model, CHD prevention at the work site could focus on instruments aiming at an increase of perceived decision latitude or decreased perception of psychosocial demands or both in order to decrease the prevalence of perceived strain at the work site. To sum up, only an experimental design such as a randomized trial pairing off occupational units or factories, one experimental the other control, and looking at the relation of experimental modification of perceived job strain with that of incident CHD would establish without a doubt a causal relation between the strain model and CHD, which, in turn, would have far-reaching implications for public health and health economics.
The other approach using very general questions concerning chronic stress mixing stress in and outside work lends itself much less to CHD prevention but could increase focus on an aggressive approach to the modification of the major CHD risk factors at the work site as a contribution to the decrease of the CHD epidemic.
Limitations of the study
The study has some limitations, the first one being selection bias: although many different industries were included in the Brussels, Ghent and Lille centers, they were nevertheless selected industries having agreed to participate. This is not the case for the population samples of Barcelona, Göteborg and Malmö from which subjects at work represented a host of industries and job titles were extracted. The participation rate was rather low in some centers which can preclude generalization of the results. Although standardization was at a high level some centers had already started their survey; thus the Malmö center when applying the Karasek items for psychological demands and control had different scales for answers and a calibration study had to be performed.
Detection of new CHD major events was not standardized over all centers but the MONICA study criteria were applied for the inclusion of new cases.
Moreover a certain level of heterogeneity between centers was observed for job strain. Notwithstanding we feel this study, a first European multicenter prospective epidemiological observational study using the same items of the Karasek model with a short follow-up and sufficient statistical power in order to include only acute coronary events, to have contributed evidence linking the demand/control/strain model to coronary heart disease.
Footnotes
Acknowledgements
We would like to thank Professor Robert Karasek for his judicious advice and revision of the Karasek scales of all participating JACE centers.
Appendix
Participating centers in the JACE study. ∗Indicates principal investigator.