
Abstract
Background
This study was designed to research the effect of hypercholesterolemia and ascorbic acid on forearm blood flow (FBF) reactive hyperaemia (RH). Reactive hyperaemia seems to be at least partly endothelium-dependent. Endothelial dysfunction has been described in patients with hypercholesterolaemia, and has been reversed with ascorbic acid administration.
Method
Forearm blood flow was studied with venous occlusion plethsmography in 26 healthy volunteers and 46 hypercholesterolaemic patients. Hypercholesterolaemic patients were divided into two groups. Group A comprised 25 patients, who received ascorbic acid and group B comprised 21 patients, who received placebo. All subjects underwent measurement of FBF at baseline and during RH (phase A). Forearm blood flow during RH was measured every 15 seconds for three minutes. Subsequently patients in group A received 2 g of ascorbic acid orally in the form of effervent tablets, and patients in group B received placebo orally in the same form. Forearm blood flow measurements at baseline and during RH were repeated two hours later (phase B).
Results
Maximal percent increase of FBF was significantly higher in healthy subjects than in hypercholesterolaemic patients (139.1 ± 12.1% versus 73.1 ± 11.0% respectively, P<0.05). Duration of RH was smaller in hypercholesterolaemic patients compared to normal subjects (60.9 ± 17.1 seconds versus 105.6 ± 10.2 seconds, P<0.05). Administration of ascorbic acid but not of placebo increased the duration of RH (69.1 ± 11.1 seconds versus 104.1 ± 12.2 seconds, P<0.05) but not of peak RH FBF.
Conclusion
Hypercholesterolaemia seems to impair both the early and late phase of RH. Ascorbic acid improves only the duration of RH, possibly due to its antioxidant effect on endothelium.
Introduction
Reactive hyperaemia (RH) is a protective adaptation that has evolved in mammals to ensure prompt restoration of blood flow and metabolic debt repayment when flow is interrupted abruptly and ischemia is induced. Myogenic [1, 2] and local factors [3–9] are believed to play a crucial role in RH response. Recently the role of vascular endothelium has been recognised in the regulation of RH in the human forearm, via the production of vasodilating substances, mainly nitric oxide (NO) [10–13] and prostaglandins [13–16]. The quantitative contribution of each factor to RH seems to depend on the vascular bed and the mechanism by which ischemia or tissue hypoxia is produced. Despite the fact that the role of vascular endothelium in the different phases of RH in human forearm remains a matter for further investigation, most studies show that it participates more in the mid to late phase of RH rather than the early phase, mainly through the production of NO [10, 11, 13].
The effect of hypercholesterolaemia on microcirculation as assessed by RH forearm blood flow (FBF) is not well known. Diverging conclusions concerning peak RH FBF in hypercholesterolaemic patients have been reached [17–20], while no evidence exists on the effect of hypercholesterolaemia on the duration of RH. Impaired endothelial function has been recognized as an early event in patients with hypercholesterolaemia [21, 22], a well-known risk factor predisposing to coronary artery disease. Endothelial dysfunction, as assessed by endothelium-dependent vasodilation, has been described in hypercholesterolaemic patients, in macrocirculation [23, 24] and microcirculation [18, 21, 22]. Reduced bioavailability of the major endothelium-derived relaxant factor, that is, nitric oxide, caused by increased vascular oxidative stress [22], seems to be the leading cause of endothelial dysfunction in hypercholesterolaemia.
Ascorbic acid is the most potent water-soluble antioxidant in human plasma [25]. It is effective in scavenging intracellular superoxide or other reactive oxygen species [26], and plays an important role in the regulation of intracellular redox state through its interaction with glutathione [27]. Ascorbic acid has been successfully used in order to reverse endothelial vasomotor dysfunction in patients with hypercholesterolaemia [28].
The purposes of this study were (a) to test the hypothesis that hypercholesterolaemia impairs forearm reactive hyperaemia blood flow and (b) to examine whether administration of ascorbic acid reverses the potentially impaired forearm reactive hyperaemia blood flow.
Methods
Subjects
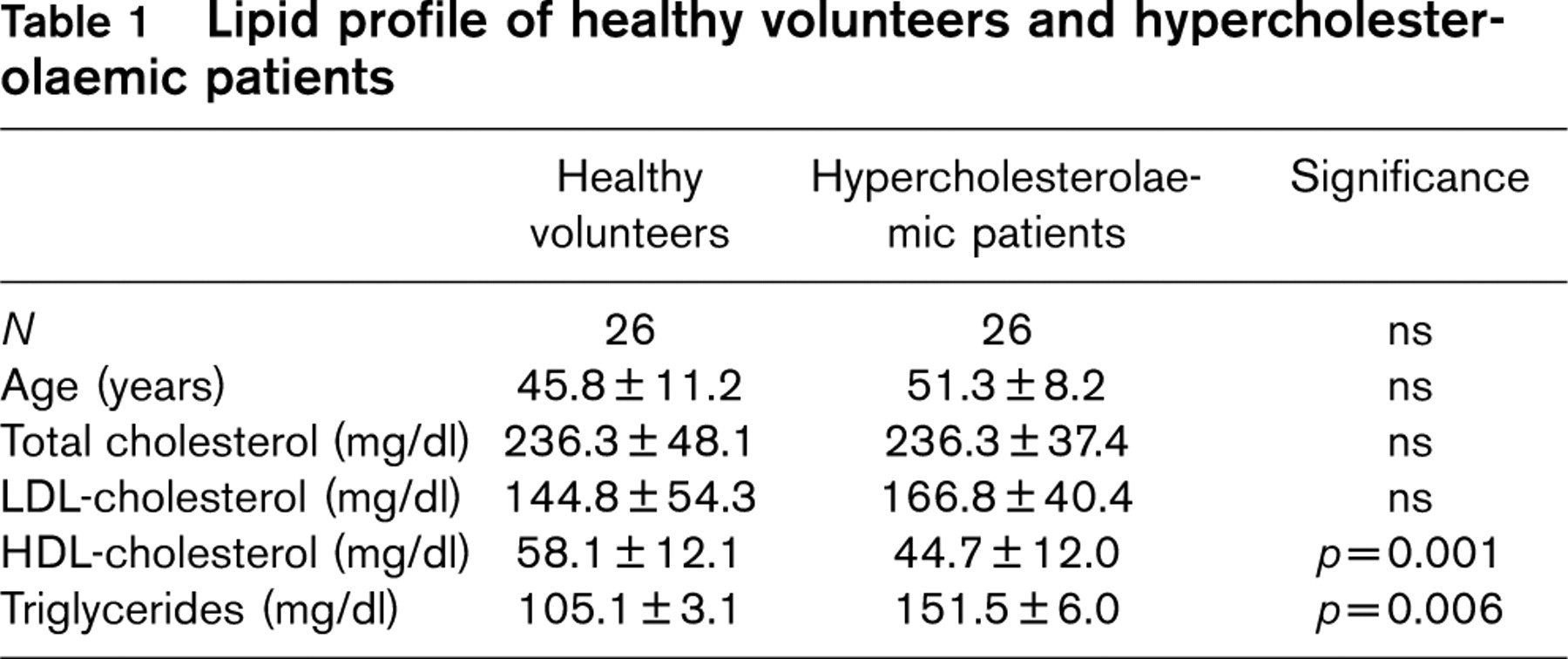
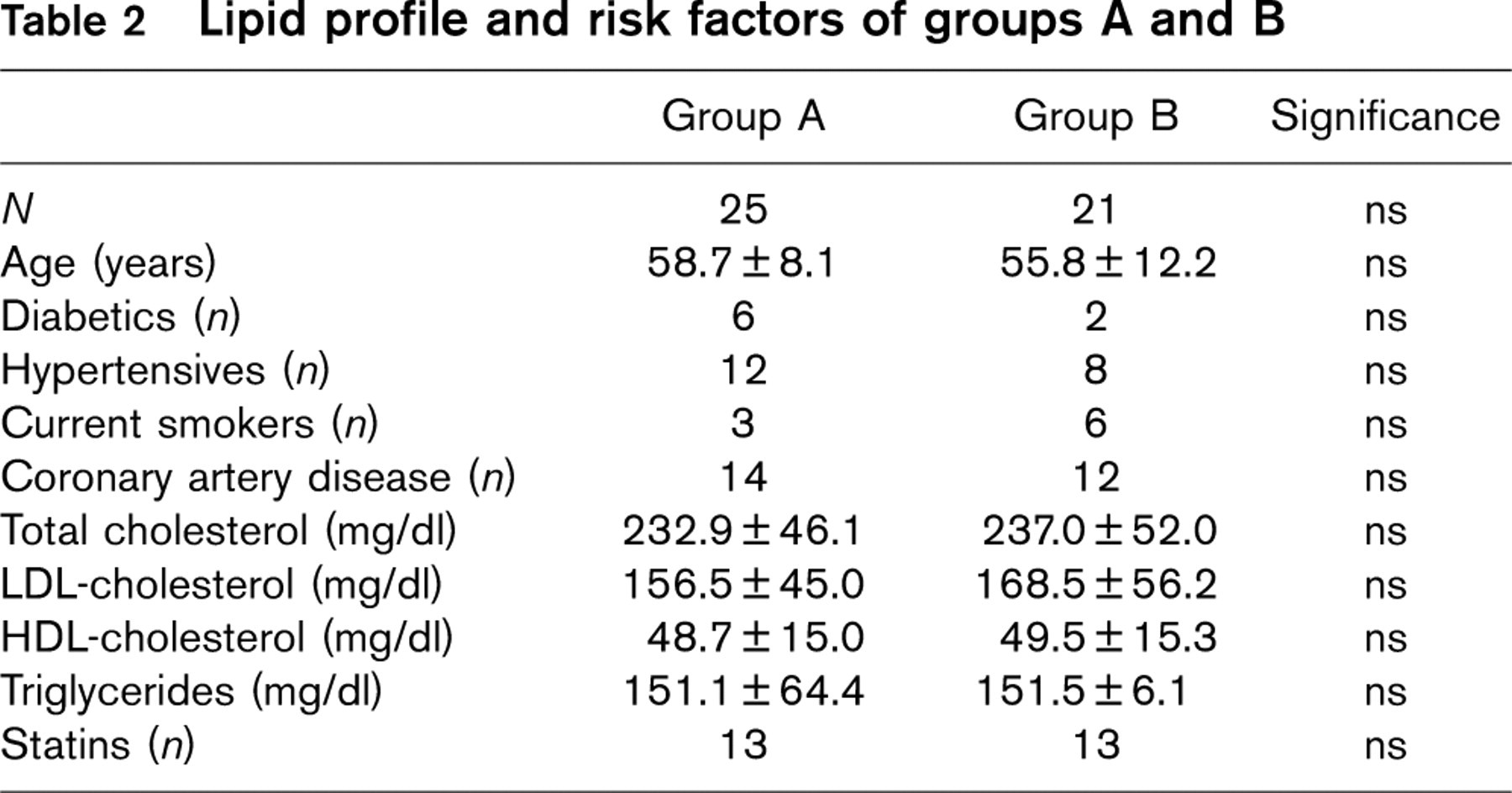
Twenty-six healthy volunteers (19–69 years old, mean 45.8 ± 11.2 years) and 46 hypercholesterolaemic patients (26–78 years old, mean 56.7 ± 7.3 years) participated in the study. Informed consent was obtained from each subject and the local Scientific Committee approved the protocol. All hypercholesterolaemic patients were on a low lipid diet and 26 were treated with statins. Eight patients had diabetes mellitus, 25 had coronary artery disease, 22 had hypertension, and nine were current smokers. Healthy volunteers had no clinical sign of cardiovascular disease. Their lipid profile is described in Table 1. All hypercholesterolaemic patients were randomised into two groups. Group A comprised 25 patients (21 males, mean age of 58.7 ± 8.1 years), who received ascorbic acid and group B comprised 21 patients (19 males, mean age of 55.8 ± 12.2 years), who received placebo. Their lipid profile and other risk factors are described in Table 2. Thirteen patients in each group were on statin treatment. The two groups were comparable concerning lipid profile, age and other risk factors. We selected 26 patients with hypercholesterolaemia (26–68 years old, mean 51.3 ± 8 years) out of 46, in order to get an age-matched population of hypercholesterolaemic patients comparable to healthy subjects. Their lipid profile is described in Table 1.
Study design
The study was performed with subjects in a supine position having their right arm supported at the elbow and wrist with foam blocks, in steady room temperature. All participants underwent measurement of FBF at baseline and during RH (phase A). Forearm blood flow during RH was measured every 15 s for three min. Subsequently patients in group A received 2g of ascorbic acid orally in the form of effervent tablets, and patients in group B received placebo orally in the same form. Forearm blood flow measurements at baseline and during RH were repeated two h later (phase B). Blood pressure was measured by clinical sphygmomanometer in the contralateral arm at baseline and during RH (at 0 min, 1 min, and 2 min after the release of arterial occlusion), in both phases. All participants were instructed not to have any food, drink, smoke or medication during the two-hour interval and not to have any vasoactive medication at least 48 h prior to the vascular tests. On the contrary statins were not discontinued throughout the study. Since it is known that ascorbic acid does not influence endothelial function in normal subjects, we did not examine the effect of ascorbic acid in the control group [28].
Lipid profile of healthy volunteers and hypercholesterolaemic patients
Lipid profile and risk factors of groups A and B
Plethysmography
Strain gauge venous occlusion plethysmography, a well known and highly accurate method for the study of small arterioles [29, 30], was used to study FBF. Forearm blood flow studies were performed by using a strain gauge plethysmograph (model EC5R, Hokanson DE). Mercury-filled silastic strain gauges of appropriate size for each subject were placed 5 cm below the antecubital crease, while a rapid cuff inflator (model E20, Hokanson DE) and an air source (AG101 air source) inflated a vascular cuff to 50 mmHg, which was used to occlude venous outflow from the extremity at the level of the upper arm. Forearm blood flow was calculated as relative percent change of limb volume (mL/min per 100 mL). Reactive hyperaemia was produced by inflating a wrist cuff to suprasystolic pressure for four minutes. It is known that such a duration of arterial occlusion produces close to maximal vasodilation of the blood vessels and maximal peak RH FBF [17].
Ascorbic acid concentration
Oral ingestion of 2 g ascorbic acid is known to produce a 2.5-fold increase in plasma concentration two h after ingestion, but within the physiological range (30–150 mol/L) [39], and a plateau is maintained for five h after ingestion [31]. This dose of orally ingested ascorbate was proved to be efficient in reversing endothelial vasomotor dysfunction in patients with coronary artery disease [31]. On the basis of this knowledge we chose to study hypercholesterolaemic patients two h after ingestion of 2 g of ascorbate.
Derived parameters
Peak RH FBF corresponds to the maximal RH blood flow that was observed immediately after arterial occlusion release. Percentage change of flow (dfl%) during hyperaemia was calculated as [(RH FBF-Basal flow)/Basal flow]100. Maximal percentage change of flow (maxdfl%) corresponds to dfl% during peak RH FBF. Duration of hyperaemia for each subject was defined as the time the hyperaemic flow returned within baseline. Baseline for each subject was defined as the subject's basal flow plus the difference of group's lower hyperaemic blood flow minus the group's basal flow.
Statistical analysis
All variables are expressed as mean ± SD. T-test and chi-square tests were applied in order to evaluate differences in demographic traits and lipid profiles of patients, as well as baseline FBF and peak RH FBF. Analysis of variance (ANOVA) for repeated measures between groups and within groups was applied for evaluation of flow parameters (duration of hyperaemia, dfl%). The group's lower hyperaemic blood flow was determined as the smaller RH FBF significantly higher than the group's basal flow (post hoc ANOVA for repeated measures). A P < 0.05 was considered to be the level of statistical significance. SPSS version 10.0 was used.
Results
Control volunteers versus age-matched hypercholesterolaemic patients
Forearm blood flow at rest and peak RH FBF did not differ significantly between control and hypercholesterolaemic patients (Table 3). Max dfl% was significantly higher in healthy subjects than in hypercholesterolaemic patients (139.1 ± 12.1% versus 73.1 ± 11.0% respectively, P<0.05) (Table 3). Duration of RH was smaller in hypercholesterolaemic patients compared to normal subjects (60.9 ± 17.1 s versus 105.6 ± 10.2 s, P<0.05) (Fig. 1).
Group A
Forearm blood flow at rest did not differ significantly before and after treatment with ascorbic acid (Table 3). Peak RH FBF also did not differ significantly before and after administration of ascorbic acid respectively (Table 3). Max dfl% did not differ significantly before and after treatment with ascorbic acid (Table 3). Duration of RH FBF was improved in hypercholesterolaemic patients who received ascorbic acid from 69.1 ± 11.1 s to 104.1 ± 12.2 s, P<0.05, (Fig. 1).
Group B
Forearm blood flow at rest did not differ significantly before and after treatment with placebo in group B (Table 3). Peak RH FBF also did not differ significantly before and after placebo treatment (Table 3). Max dfl% did not differ significantly before and after treatment with placebo in group B (Table 3). Duration of RH FBF did not improve in hypercholesterolaemic patients who received placebo (58.8 ± 12.3 s versus 62.2 ± 96.1 s, ns) (Fig. 1).
Plethysmographic parameters
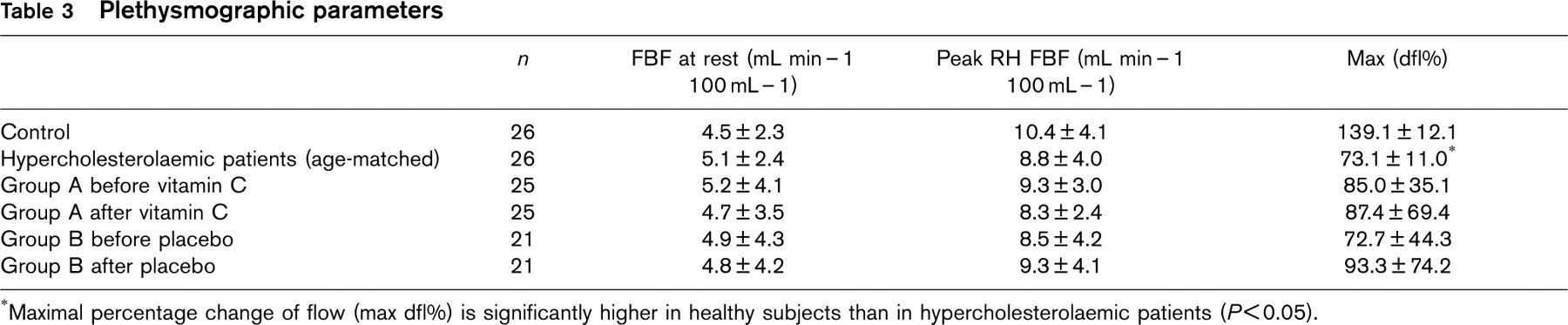
∗Maximal percentage change of flow (max dfl%) is significantly higher in healthy subjects than in hypercholesterolaemic patients (P<0.05).
Discussion
The role of vascular endothelium in different RH response phases
Reactive hyperaemia blood flow may be considered to have two phases, regarding its physiological mechanisms of development [10]; an early phase immediately after cuff release and a mid-to-late phase. In this study, the early phase corresponds to the first plethysmographic recording after the release of the wrist cuff, and it is expressed by peak RH FBF and maxdfl%. Mid-to-late phase of RH is expressed as duration of RH.
Vascular endothelium has a controversial role in RH response
The release of endothelium-derived vasodilating factors such as NO, as well as prostacyclin, is stimulated by physiological changes like hypoxia and shear stress, both features of RH [32–36]. Nevertheless various controversial studies have been published concerning the contribution of NO [10–13] and of prostacyclin [13–16] in RH response. Nitric oxide seems to play minimal role in early vasodilation, that is in peak RH FBF and max dfl% [10, 11, 13]. On the other hand NO appears to play a modest yet significant role in the mid-to-late phase of RH FBF, that is contributing to maintaining the vasodilation after peak RH FBF, augmenting in this way the duration of RH [10, 12, 13]. It is assumed that increased flow during peak RH FBF in the early phase of RH induces NO production due to increased shear stress. Nitric oxide is expected to exert its vasodilatory action after a short delay of approximately 60 s [11, 24], increasing thereby the duration of RH by enhancing the mid-to-late phase of RH and not peak RH FBF. The role of prostaglandins in the different phases of RH is not yet completely understood either. Peak RH FBF seems to be reduced by 15–30% when prostaglandin production is inhibited [13–15]. Conflicting results exist so far concerning the participation of prostaglandin in mid-to-late phase of RH, showing both increased and decreased blood flow responses to prostaglandin inhibition [13, 16]. Finally, adenosine, another well-known factor contributing to RH, has been postulated to be produced by endothelial cells [5] and to participate in peak RH FBF, but not in duration of RH [5]. It should be taken into consideration that all previous studies examined healthy subjects and there is no evidence concerning endothelial NO and prostacyclin contribution to RH in hypercholesterolaemic patients.
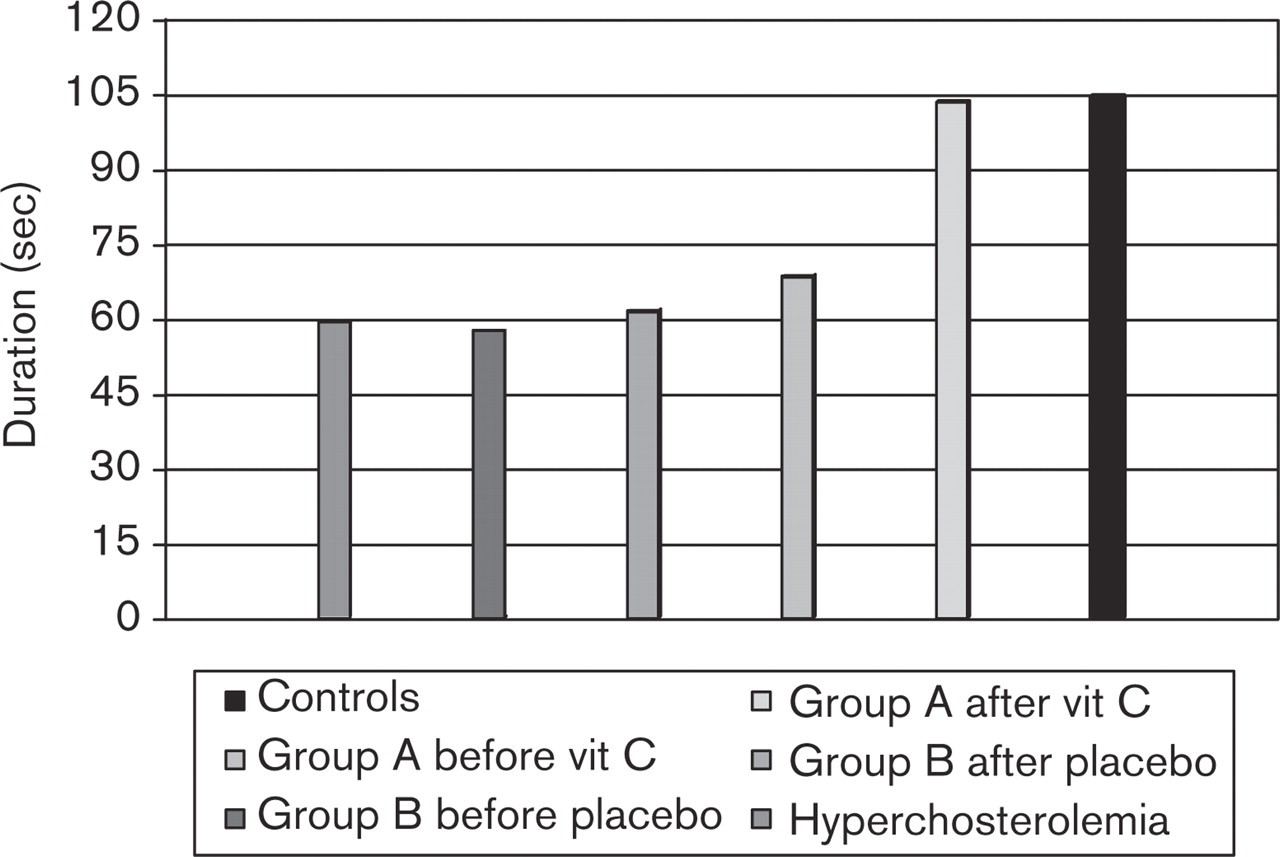
Duration of reactive hyperaemia. Analysis of variance (ANOVA) for repeated measures. Duration of RH was smaller in hypercholesterolaemic patients compared to normal subjects (60.9 ± 17.1 s versus 105.6 ± 10.2 s, p<0.05). Duration of RH FBF was improved in hypercholesterolaemic patients who received ascorbic acid (69.1 ± 11.1 s to 104.1 ± 12.2 s, p<0.05).
Hypercholesterolaemia, endothelial vasomotor dysfunction and RH
Endothelial dysfunction in the microcirculation of hypercholesterolaemic patients as assessed by acetylcho-line intra-arterial infusion has been previously observed [21]. On the other hand, the effect of hypercholesterolaemia on RH is not well known. Diverging conclusions concerning peak RH FBF in hypercholesterolaemic patients have been reached [17–19], while no evidence exists on the effect of hypercholesterolaemia on the duration of RH. Zelis et al., [17] studied RH at both upper and lower extremities. They found that among hypercholesterolaemic patients only those with type III hyperlipoproteinaemia had lower peak RH blood flow compared to normal subjects. They also found that peak RH blood flow significantly decreased as the age of the subject increased. On the other hand, Creager et al., [18] studied younger hypercholesterolaemic patients and they showed no significant changes in peak RH FBF compared to normal subjects, apart from the fact that endothelial dysfunction and even smooth muscle dysfunction were present. Schobel et al., [19] showed that peak RH FBF increased after long term treatment with fluvastatin, indicating a beneficial effect on structural abnormalities in the vascular smooth muscle, secondary to high serum cholesterol. Finally, Cotrella et al., [20] found no significant changes in peak RH FBF between young hypercholesterolaemic patients and normal subjects as well as that treatment with statins had no effect on peak RH FBFB. On the other hand, in the same study Cortella et al., [20] found reduced peak RH blood flow and flow debt repayment at the lower limb, which were reversed by treatment with simvastatin. All four studies mentioned above used venous occlusion plethysmography in order to assess limb blood flow. It may be supported that differences in population traits (such as age), as well as in vascular bed (lower and upper arm) are responsible for differences found in results.
Our results∼FBF at baseline
Endothelial dysfunction in microcirculation in hypercholesterolaemic patients has been observed [21]. Despite the fact that FBF at rest has been shown to be endothelium-dependent [10] and basal release of NO is, beyond any doubt, contributing to basal FBF, no difference has ever been observed by other investigators in FBF between healthy subjects and hypercholesterolaemic patients [18]. In our study also no significant difference was observed in FBF at rest between healthy subjects and hypercholesterolaemic patients. Furthermore, ascorbic acid did not seem to have any effect on basal FBF. A reasonable explanation for these results could be that the mechanism of NO's basal release remains intact in hypercholesterolaemic patients.
Our results∼RH
In hypercholesterolaemic patients the early phase of RH as expressed by maxdfl%, but not as peak RH FBF, was decreased compared to healthy subjects. It seems reasonable to consider that maxdfl% may reflect in a more accurate way vasodilatory changes of resistance vessels in the early phase of RH than absolute peak RH FBF values, since even non statistical differences in basal FBF that are present in our study may be evaluated in this way. We believe that our results (Table 3) would be underestimated if only absolute blood flow values were appreciated. Nevertheless we should acknowledge the fact that the use of maximal percent increase of blood flow might sometimes over-emphasize such differences and therefore should be used very cautiously. Ascorbic acid has been successfully used in many studies for the reversal of endothelial vasomotor dysfunction in hypercholesterolaemic patients but it has never been used in RH. In this study ascorbic acid administered at a dose of 2g had no effect on the early phase of RH (peak RH FBF and maxdfl%). This may be due to insignificant participation of the endothelium in the early phase of RH. On the other hand, peak RH FBF response has been considered to serve as an index of maximal vasodilatory capacity of resistance vessels [37] and as an hemodynamic index of structural changes in conduit vessels [18, 19]. An ischemic stimulus presumably dilates the arterioles sufficiently, so that the caliber of larger arteries, that is, the inflow vessels, becomes the critical site for resistance. Therefore, a reduction in peak blood flow to an extremity indicates a reduced caliber in the conduit vessels if there is no evidence of arteriolar disease [17, 38]. Such subclinical lesions may be present in our hypercholesterolaemic population. If this were true it would be unlikely to observe any improvement after acute administration of ascorbic acid. Finally, it is possible that the root of administration or the quantity of ascorbic used was not sufficient for the reversal of potential endothelial dysfunction in the early phase of RH.
Duration of RH was found to be impaired in hypercholesterolaemic patients compared to healthy subjects. It was also found that ascorbic acid, but not placebo, increased RH duration in hypercholesterolaemic patients up to a level similar to that measured in control subjects. Ascorbic acid seems to be responsible for the increase of RH duration in hypercholesterolaemic patients since stimulation of endothelial cells by shear stress due to increased blood flow, as expressed by max dfl%, is of equal degree among group A and group B. Therefore increased oxidative stress may be responsible for reduced RH duration. Endothelial dysfunction due to increased oxidative stress may be at least partly responsible for reduced RH duration in hypercholesterolaemic patients compared to healthy subjects. In this study ascorbic acid was administrated at a dose of 2 mg. Ascorbic acid concentration in plasma could not have exceeded normal concentration [31] and it is unlikely that a direct scavenging effect on free radicals has been achieved [40], since a ten times higher concentration is needed for such an action. It is more likely that intracellular redox state changes mediated a positive effect on endothelial function [27, 40, 41].
Limitations
Hypercholesterolaemia was the common feature of our patients study group. Nevertheless the existence of other factors (smoking, diabetes mellitus, hypertension, coronary artery disease) that are related to endothelial dysfunction should be considered at least partly as coresponsible for impaired RH. The effect of ascorbic acid may also have been more profound in our study group since increased oxidative stress is considered to be one common pathway underlying endothelial dysfunction in all situations mentioned above.
Conclusion
The early as well as the mid-to-late phases of RH are impaired in hypercholesterolaemic patients and percentage change of FBF seems to be a more sensitive index of vascular dysfunction than absolute value of FBF. Maxdfl% is not affected by administration of ascorbic acid in hypercholesterolaemic patients suggesting that peak RH FBF may be useful as an index of structural lesions but it is unlikely to be related with endothelial function. Duration of RH is increased by ascorbic acid administration in hypercholesterolaemic patients, possibly by reducing oxidative stress and reversing endothelial dysfunction. Therefore it seems reasonable that duration of RH may be used as an endothelial function test of forearm resistance vessels, and more studies are necessary on this item.