
Abstract
Background
Folic acid therapy has been shown to improve endothelial function in patients with familial hypercholesterolaemia via a possible antioxidant mechanism. Data on the possible role of folic acid in hypercholesterolaemic patients receiving statins are lacking. In the present study we tested the hypothesis that folic acid supplementation improves endothelial function in patients with hypercholesterolemia and treatment with statins.
Methods
Thirty-four hypercholesterolaemic patients receiving statins participated in the study; all subjects underwent measurement of endothelium-dependent, flow-mediated dilatation of the brachial artery and subsequently randomized to receive 5 mg of the folic acid (n = 17) or placebo (n = 17) for 4 weeks. Flow-mediated dilatation of the brachial artery was repeated at the end of the 4-week period.
Results
Folic acid and placebo groups were comparable regarding age, sex, smoking, hypertension, coronary artery disease, obesity, family history and blood lipids. Folic acid administration resulted in an improvement of flow-mediated dilatation (4.7 ± 3.2% to 7.1 ± 3.1%, P = 0.02), whereas there was no improvement after placebo administration (5.7 ± 3.8% to 5.6 ± 2.2%, ns). No significant change in nitrate-induced, endothelium- independent dilatation was observed after folic acid or placebo (ns).
Conclusions
Oral administration of folic acid (5 mg) for 4 weeks improves endothelial function in patients with hypercholesterolemia treated with statins, with possible beneficial effects on the prognosis of these patients.
Introduction
The endothelium plays an important role in maintaining vascular integrity through the production and release of vasoactive substances such as nitric oxide (NO) [1]. Endothelial dysfunction is an early and important feature in the development of atherosclerosis, appearing long before the formation of atherosclerotic lesions [2]. Hypercholesterolaemia is one of the risk factors leading to endothelial dysfunction [3], while cholesterol reduction improves both coronary and systemic endothelial function [4,5]. The mechanisms responsible for the observed endothelial dysfunction have not been completely elucidated but increased oxidative stress has been implicated as a possible cause; indeed treatment with antioxidants improved endothelial function in humans and animals [6,7].
Folic acid therapy has been shown to improve endothelial function in hyperhomocysteinaemia and familial hypercholesterolaemia [8,9]. Possible mechanisms include the reduction of homocysteine levels, regeneration of biopterin, an essential cofactor for NO synthase and finally an antioxidant effect of folates [10–12. Data on the possible beneficial role of folic acid supplementation in patients with hypercholesterolaemia receiving statins as lipid-lowering therapy are lacking. Therefore we tested the hypothesis that folic acid supplementation can improve endothelium-dependent, flow-mediated dilatation of the brachial artery in patients with hypercholesterolaemia and treatment with statins.
Methods
Patient population
Thirty-four hypercholesterolaemic subjects followed in the Lipid Center of the Department of Clinical Therapeutics, Alexandra University Hospital participated in the study according to a double-blind design. All patients were on treatment with statins for at least 6 months before the beginning of the study. Seventeen patients had known coronary artery disease. All patients gave informed consent before entering the study and the study protocol was approved by the local Ethics Committee.
All vasoactive medications were withheld for at least 12 h before study and all long-acting vasoactive medications were withheld for at least 24 h before measurements.
Study protocol
Endothelium-dependent, flow-mediated dilatation of the brachial artery was determined as described previously [2], using high-resolution echo-Doppler ultrasound (Acuson 128 X P, Mountain View Calif, 7.0 MHz transducer). In brief, the subjects were studied in the morning having abstained from alcohol, caffeine and food for 8 h before the study. Optimal imaging of the right brachial artery was obtained and a resting scan was recorded using a pulsed Doppler signal at 601 angle in the centre of the artery. The skin was marked and all subsequent images were obtained at the same location. Increased flow was then induced by inflation of a blood pressure cuff on the forearm to 250 mmHg for 5 min; after release of the cuff reactive hyperaemia occurs; brachial artery was scanned continuously for 30 s before and 90 s after cuff deflation. For the study of endothelium-independent dilatation, 0.4 mg of nitroglycerin was given sublingually and the brachial artery was imaged 4 min later.
All images were recorded on super VHS videotape for offline analysis by two observers (JL, CP). Artery diameter measurements were taken from the anterior to the posterior m-line at end-diastole using electronic calipers. Blood flow at baseline and during hyperaemia was calculated as the product of velocity and πr2 (π = 3.14, r = vessel diameter/2) multiplied by the corresponding heart rate. Flow-mediated dilatation (FMD) was calculated as the percent increase in arterial diameter during hyperaemia as compared with resting scan. Also nitrate-induced dilatation was calculated similarly. The intraobserver and inter-observer variability for repeated measurements of artery diameter are 0.1 ± 0.12mm and 0.08 ± 0.19 mm respectively in our laboratory. In flow-mediated dilatation studies performed on two separate days, the mean difference in brachial vasodilator response was 1.1 ± 1%.
Baseline characteristics of study population
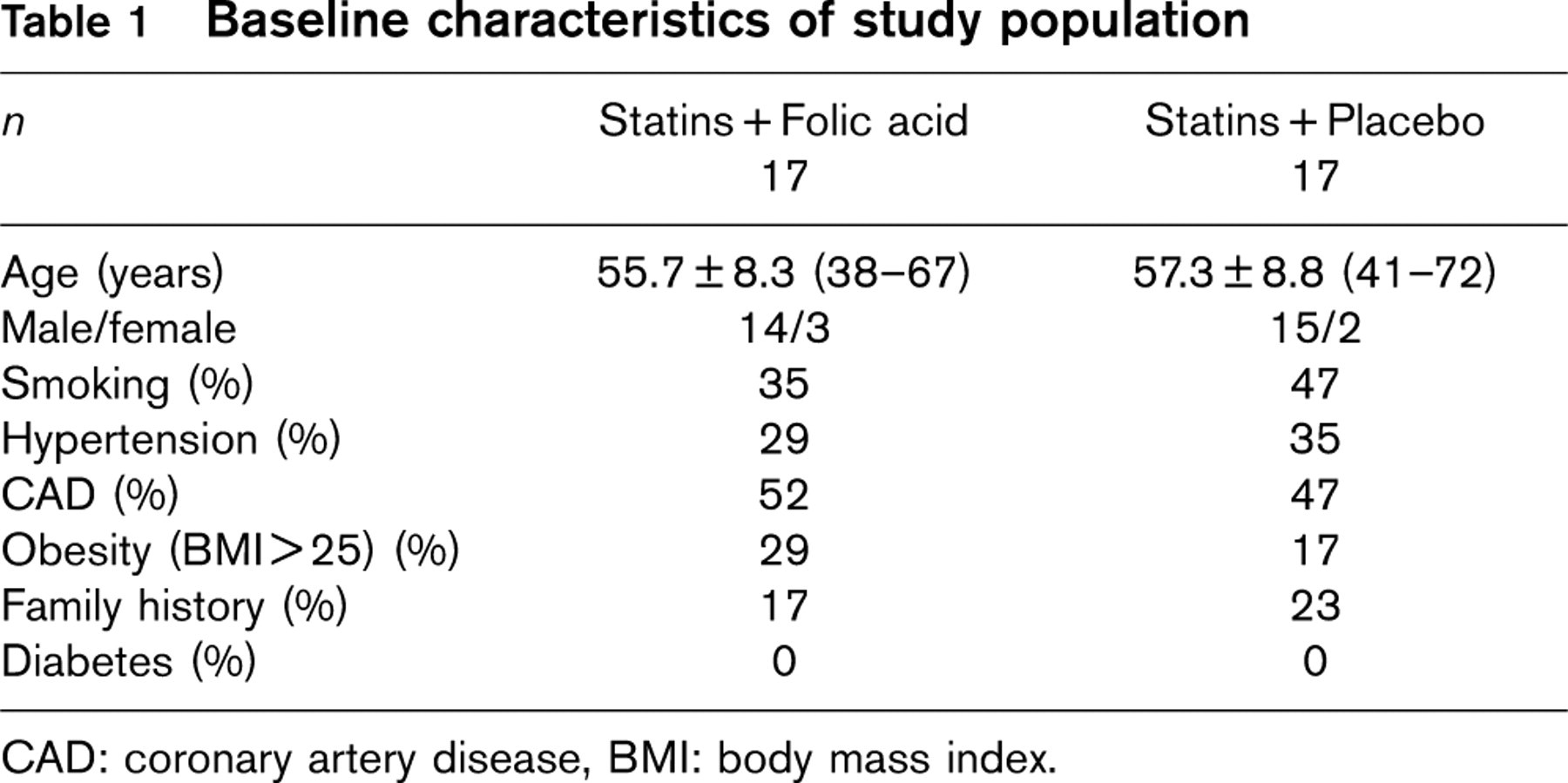
CAD: coronary artery disease, BMI: body mass index.
After completion of the first vasoreactivity study patients were randomized to receive either 5 mg of folic acid orally for 4 weeks (17 patients, group A) or placebo (17 patients, group B) in addition to their treatment. The folic acid and placebo groups were similar to their baseline characteristics (Table 1). Medications did not change during the period of the study. After the completion of the 4-week period of the study vasoreactivity studies were repeated as described above.
Biochemical studies
Blood was drawn from all patients at the beginning and at completion of the study for determination of the following parameters using standard techniques. Total cholesterol, triglycerides, HDL-cholesterol, LDL-cholesterol, serum folic acid and vitamin B12.
Statistical analysis
All data are presented as mean ± SD. Continuous variables were normally distributed as indicated by the Kolmogorov-Smirnov one-sample test. Baseline clinical characteristics vessel diameter, blood flow, blood pressure, heart rate, flow-mediated dilatation and nitrate-induced dilatation, blood lipids, folic acid and vitamin B12 were compared for the folic acid and placebo groups by the student's unpaired t-test. Categorical variables such as sex, smoking, hypertension, coronary artery disease, obesity and family history of CAD were compared by using a χ2 test. Effect of treatment (folic acid or placebo) on the various haemodynamic and biochemical parameters was examined by student's paired samples t-test. Statistical significance was accepted at a P- value < 0.05.
Results
Baseline characteristics of the folic acid and placebo groups are shown in Table 1. Two groups were comparable regarding age, sex, smoking, hypertension, coronary artery disease, obesity and family history of CAD. None of the patients had diabetes mellitus.
Biochemical measurements at the beginning (measurement 1) and the end of the study (measurement 2) in the two groups are presented in Table 2. Cholesterol, triglycerides, HDL-cholesterol, LDL-cholesterol, folic acid and vitamin B12 were comparable in the two groups at the beginning of the study (ns); cholesterol, triglycerides, HDL-cholesterol, LDL cholesterol and vitamin B12 did not change significantly during the study and were comparable in the two groups at the end of the study (ns). Folic acid increased significantly in patients receiving folic acid supplementation (7.8 ± 5.6 to 13 ± 6.0 ng/ml, P = 0.01) and was significantly higher compared with the folic acid levels of the placebo group at the end of the study period (13 ± 6.0 vs. 6.9 ± 5.4 ng/ ml, P = 0.004).
Folic acid administration resulted in an improvement in endothelium-dependent, flow-mediated dilatation from 4.7 ± 3.2% to 7.1 ± 3.1% (P = 0.02), whereas there was no increase in flow-mediated dilatation with placebo administration (5.7 ± 3.8% to 5.6 ± 2.2%, ns).
To examine whether folic acid increased arterial dilatation through an effect on smooth muscle cells we compared the responses to nitroglycerin in the two groups. No significant change in nitrate-induced endothelium-independent dilatation was observed after administration of folic acid or placebo (ns) (Fig. 1).
Table 3 shows the haemodynamic changes during the treatment period. Baseline brachial diameter, baseline blood flow, systolic and diastolic blood pressure were comparable in the two groups and did not change significantly during the study after folic or placebo administration (ns). Administration of folic acid or placebo did not change the degree of reactive hyperaemia, which is the stimulus for endothelium-dependent brachial artery dilatation (ns).
Lipids, folic acid and vitamin B12 changes during the treatment period
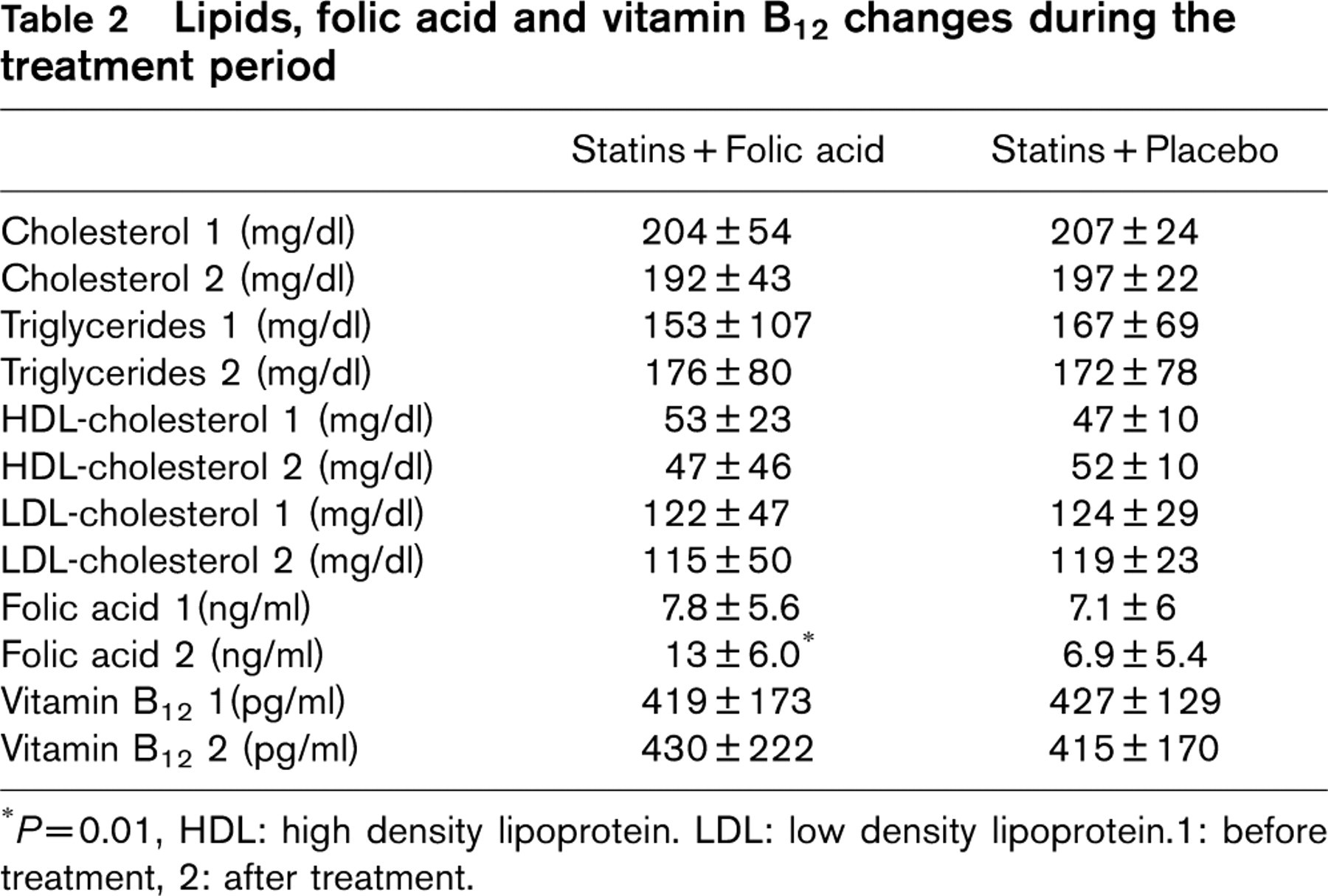
∗ P = 0.01, HDL: high density lipoprotein. LDL: low density lipoprotein.1: before treatment, 2: after treatment.
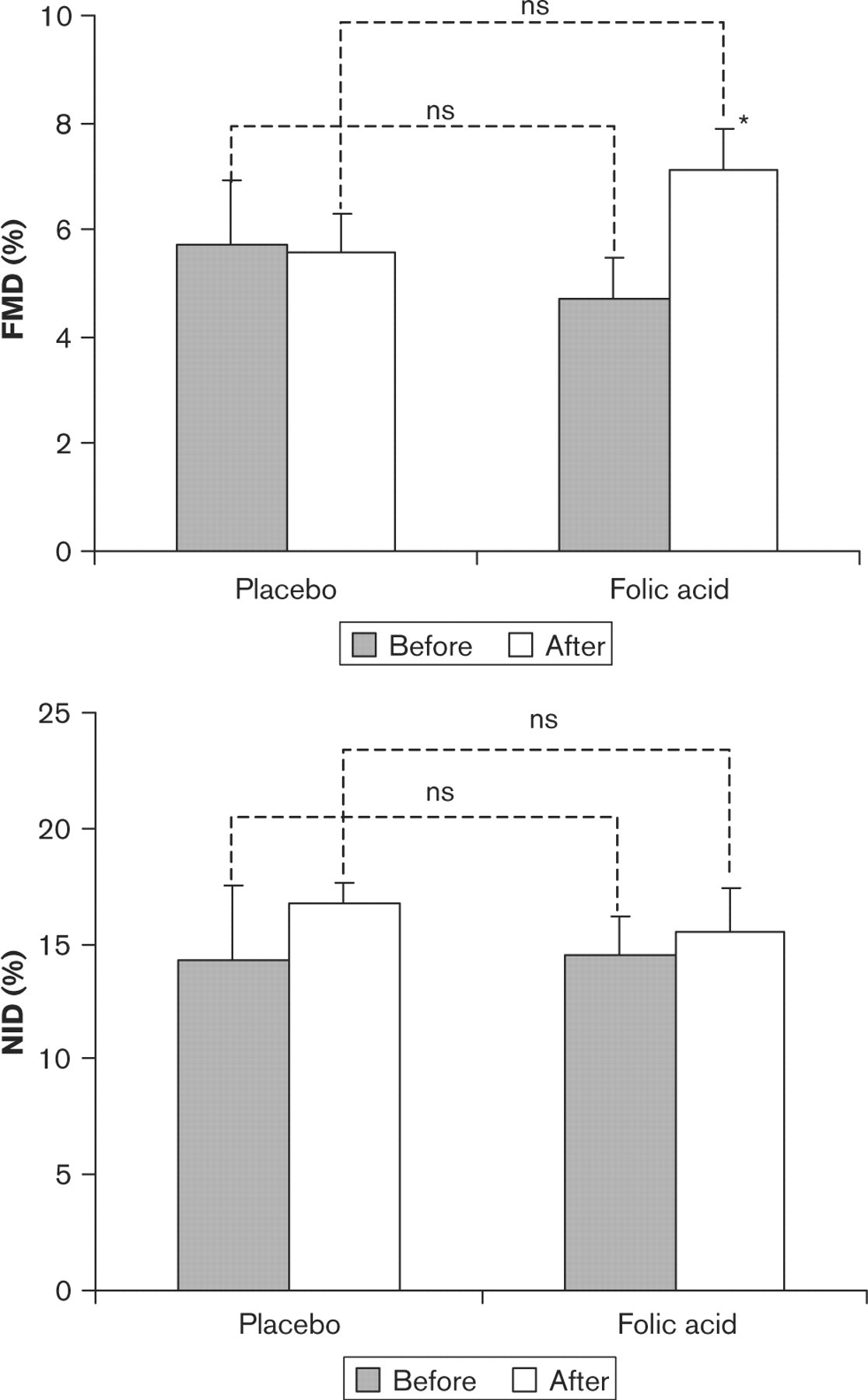
Flow-mediated dilatation (FMD) and Nitrate-induced dilatation (NID) in the brachial artery of hypercholesterolaemic patients on therapy with statins before (solid bars) and after (white bars) placebo or folic acid. ∗ P = 0.02 between FMD before and after folic acid treatment. Bars represent standard error of mean values.
Haemodynamic changes during the treatment period
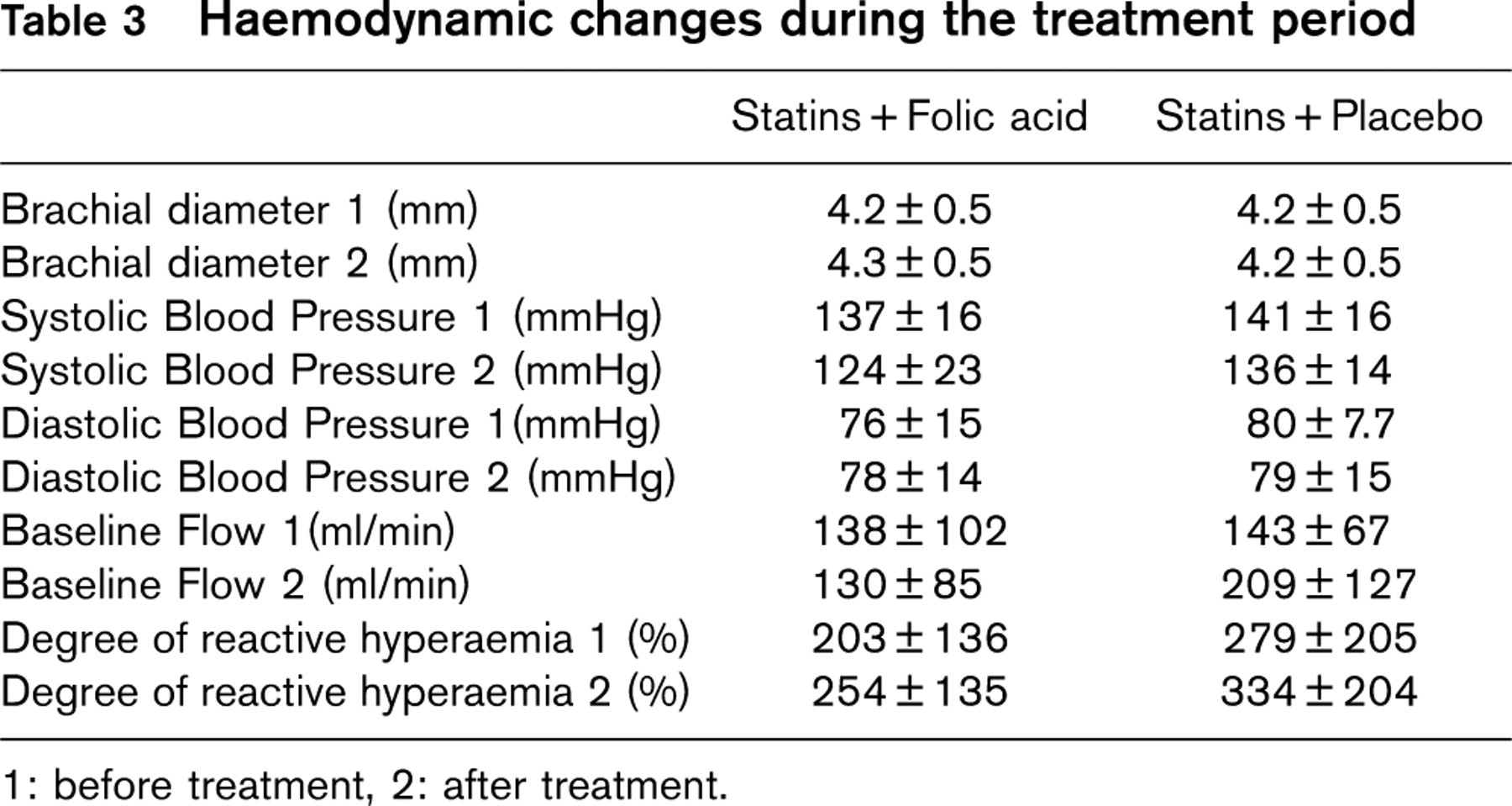
1: before treatment, 2: after treatment.
Discussion
The results of this placebo-controlled, randomized, double-blind study document that oral administration of folic acid (5 mg) for 4 weeks improves endothelial function in patients with hypercholesterolaemia treated with statins. The improvement in flow-mediated dilatation of the brachial artery was not due to an increase of the stimulus for dilatation (hyperaemia), a change in baseline arterial diameter or an effect on the smooth muscle cells of the arterial wall. Taken together, these results suggest that administration of folic acid improved NO release and/or action in the conduit arteries of these patients.
Hypercholesterolaemia and endothelial function
Hypercholesterolaemia is associated with impaired endothelial function in both resistance and conduit vessels [2,3], in coronary and peripheral vascular beds [10–12. Cholesterol-lowering intervention can reverse endothelial dysfunction in both the coronary and peripheral arteries [4,5,13–17]. In our study all patients were on treatment with statins for at least 6 months and we can assume that at the beginning of the study the beneficial effect of statin therapy on endothelium had been accomplished. It should be noticed that the brachial artery flow-mediated dilatation of our patients in the beginning of the study was lower than the values obtained from normal controls in our laboratory [18], as well as in other laboratories [19], suggesting that chronic lipid-lowering treatment improves but does not normalize endothelial function. Anderson and coworkers [20] demonstrated that treatment with a combination of lovastatin and an antioxidant improved coronary artery endothelium-dependent vasodilator response to acetylcholine compared with dietary treatment, while the effect of lovastatin alone was modest. The degree of impairment of endothelial function is correlated with serum cholesterol [15], but therapy with statins may improve endothelial function through other mechanisms, some of which could be independent of its cholesterol-lowering effect [21,22]. It is not clear whether more aggressive lowering of LDL-cholesterol would benefit endothelial function in our study. The levels of LDL cholesterol in our patients were close to those recommended for primary and secondary prevention and it is clear that the endothelial dysfunction was still present in many patients; therefore in these patients either a more aggressive lipid-lowering therapy is needed or adjunct therapy is required further to improve endothelial function.
Folic acid and endothelial function
Folic acid has been shown to improve endothelial function in patients with hyperhomocysteinaemia; flow-mediated dilatation of the brachial artery improved significantly after 6–8 weeks of oral treatment with folic acid (5–10 mg daily) [8,23], while biological markers of endothelial injury (plasma soluble thrombomodulin and von Willebrand factor) improved after 3 months treatment with folic acid and vitamin B6. Acute intra-arterial administration of 5-methyltetrahydrofolate, the active form of folic acid, restored endothelial function in patients with familial hypercholesterolaemia and normal serum folate and homocysteine levels [25], while oral supplementation of folic acid for 4 weeks improved endothelial function in familial hypercholesterolaemia [9]. In all these patients with familial hypercholesterolaemia, studies were performed at least 2 weeks after withdrawal of lipid-lowering medications while none of the participants had clinical signs of coronary heart disease. On the contrary, in our study folic acid was given to patients who were older, already on treatment with statins, while almost half of them had coronary artery disease; such patients represent a major part of the routine cardiology practice in primary and secondary prevention.
A modest effect of folic acid on homocysteine levels [9] may have contributed to the observed enhancement of endothelial function in our study, although it should be noticed that acute administration of the active form of folic acid restored endothelial function without significant alterations in homocysteine levels [25]. An antioxidant effect of folic acid is a very attractive possible mechanism; 5-methyltetrahydrofolate causes a reduction in the e-NOS and xanthinoxidase induced production of superoxide in hypercholesterolaemic patients [25] and, therefore, the degree of inactivation of nitric oxide by superoxide anion may be decreased with subsequent improvement in endothelial function. The present study does not provide any data to elucidate the possible mechanisms for the improvement of endothelial function by folic acid. It should be noticed that folic acid (5 mg/day for 6 weeks) improved endothelial function in CAD patients by a mechanism largely independent of homocysteine [26] and it is likely that the majority of improvement in endothelial function is due to direct pharmacological action of folic acid rather than reduction in homocysteine levels.
Impaired endothelial function appears to be an early sign of atherosclerosis while in patients with established atherosclerosis a decrease in NO resulting from endothelial dysfunction increases thrombogenicity and leads to an increase of cardiac events [27]. A close relation between coronary artery endothelium-dependent vasomotor response to acetylcholine and flow-mediated dilatation of the brachial artery has been described [28], suggesting that our findings on endothelial function of the brachial artery are possibly applicable to the coronary arteries. Therefore the folic acid supplementation in patients with hypercholesterolaemia on therapy with statins could lead to further improvement of endothelial function in coronary arteries with possible beneficial effects on the prognosis of these patients.
It should be emphasized though that the effects of folic acid therapy on the clinical outcome after percutaneous coronary intervention is a subject of controversy; Swiss Heart Study [29] showed that homocysteine lowering therapy with folic acid and vitamins B6 and B12 decreased the incidence of major adverse events after percutaneous coronary intervention. On the other hand, Lange et al. [30], recently reported that administration of folic acid and vitamins B6 and B12 after coronary stenting may increase the risk of in-stent restenosis. It is known that the proliferation of smooth muscle cells and matrix formation are the most important mechanisms leading to restenosis after coronary stenting, a process different than the atherosclerotic process and the genesis of acute coronary syndromes in coronary vessels without coronary stenting. Further clinical studies are needed to clarify the effects of folic acid supplementation on the clinical outcome of patients with hypercholesterolaemia and/or CAD undergoing conservative therapy.