
Abstract
Background
Fluoride in drinking water prevents dental disease, which in turn has been reported to increase the risk of coronary heart disease (CHD). Since mortality from CHD in Finland is high in the north-east where the fluoride content of drinking water is low, the association was examined here in more detail.
Design
Mortality from CHD during the period 1961-1995 in 365 rural areas of Finland (188888 deaths) was linked with 2131 drinking water fluoride determinations performed in 1958 using negative binomial regression, adjustments being made for sex, age, mean income of the resident commune and drinking water magnesium and calcium.
Results
An inverse J-shaped relationship was found between drinking water fluoride and CHD, the association being most pronounced in the 1960s and levelling off consistently as a function of time. In 1961-1970, the adjusted mortality from CHD was 22% (95% confidence interval 18-27%) lower in the fourth quintile of fluoride (0.15-0.30 mg/l) than in the first quintile (0.00-0.06 mg/l) but this deficit reduced to 13% (7-18%) in 1991-1995.
Conclusions
Although causality cannot be asserted, the geographical pattern of CHD in Finland is consistent with the concentration of fluoride in drinking water. One mechanism could be that fluoride prevents dental infections, which in turn reduces mortality from CHD. The more widespread use of fluoridated toothpastes, soft drinks and certain food items since the 1960s may have reduced the significance of drinking water as a source of fluoride.
Introduction
Mortality from coronary heart disease (CHD) in Finland shows a distinct geographical pattern, with twice as high mortality in the north-east as in the south-west, and with a sharp boundary between the high and low mortality zones [1]. Only a part of this difference is attributable to the classic risk factors, and especially since the pattern has remained unchanged since the 1960s, despite a 65% decline in mortality, some permanent environmental factor has been thought to be responsible [2]. Proposed environmental factors include softness of drinking water [3], but evidence supporting its significance has remained elusive.
The present study was prompted by previous investigations performed in the 1970s [4, 5], which suggested higher mortality from CHD in areas with lower fluoride content in the drinking water than in areas with higher content, and by recent theories proposing dental infections as a factor in CHD [6]. Due to differing geological properties, ground waters in the north-east of Finland contain less minerals such as fluoride than those in the south-west [7, 8]. Since the principal source of fluoride in man is drinking water [9], the low intake of fluoride in the north-east may have contributed to the poorer dental health [10, 11] and also to the higher occurrence of CHD.
We examined mortality from CHD in Finland from small geographical areas during the period 1961–1995 in relation to drinking water measurements performed in the same areas in 1958 [8]. We also considered the degree of water hardness and mean income, which may confound the association.
Methods
Drinking water determinations
Information on drinking water parameters was based on a nationwide survey performed in 1958 by the Engineering Department of the National Board of Agriculture [8]. In all rural communes of Finland (local government districts), and in rural areas of towns, one primary school per 1000 inhabitants was randomly selected, and one of the 4th grade pupils, central in alphabetical order, was requested to bring a water sample from his or her home well. The total number of samples was 2764. The samples covered the entire land area of Finland, which in 1958 was divided into 548 local government districts (481 rural communes and 67 towns or country towns). To maximize the probability that most people in the area used well water, we accepted only samples taken in proper rural areas. The division into rural and city areas was officially used up to the year 1976–the midpoint of the study period—and only those samples were eligible which had been taken in districts classified as rural in 1976. Out of those 481 communes that had been rural in 1958, the 110 most urbanized ones had been changed to towns by 1976, or amalgamated with adjacent towns, and the remaining 371 communes were thought to represent the core rural areas. In six of these, determinations were missing, which left 2131 samples distributed over 365 communes. The samples were analysed for 25 constituents including fluoride, magnesium and calcium. An average of six determinations (range 1-17) were performed in each commune, and means and medians for fluoride, magnesium and calcium concentrations were taken to represent the average concentrations in the area.
One hundred of the original wells were re-examined in 1989 in conjunction of another study focusing on acidification of ground waters in Finland [12]. The sample in the latter study had been selected with attention on the deposition of sulphur compounds in well water. The re-examined wells were located in the five areas of Finland where airborne sulphur deposition is obvious, which made it possible to study the acidification of well waters. Among these 100 wells, we retrospectively identified 76 that were located in rural areas in 1958, and compared the fluoride, magnesium and calcium contents between the two years to detect any changes over time.
Data on income
Mean monthly income based on taxation was available by commune for the years 1970 and 1993 (unpublished information from Statistics Finland), the average of which was taken to represent the whole of the study period.
Deaths and population
Data on deaths from CHD in persons aged 35 years or more that occurred during the period 1961-1995 in any of the 365 rural communes were obtained from the Central Statistical Office of Finland. This information was based on the underlying cause of death entered on medical death certificates and had been coded according to the seventh version of the International Classification of Diseases [13] for 1961-1968 (code 420), the eighth version [14] for 1969-1986 (codes 410-414) and the ninth version [15] for 1987-1995 (codes 410-414). The causes of death, and selection of the underlying cause, if several causes were mentioned, were checked centrally by an expert physician and statistician in the Central Statistical Office. The diagnosis of CHD was based on autopsy in an average of 27% cases for 1961-1995, the percentage of autopsies varying from 10% for 1961-1965 to 32% for 1981-1985 and 26% for 1991-1995. Additional information included sex, age, year of death and place of residence at the time of death. The total number of deaths was 188888 (of which 62% were males), the average over the communes being 509 (range 19-1697).
The composition of the populations for respective years and areas regarding sex and age were obtained from vital statistics. In 1961, the population in the rural communes averaged 5800 (range 250-24500), while in 1995 the figure was 5400 (range 120-30400).
Determination of fluoride, magnesium and calcium
The determinations of drinking water fluoride, magnesium and calcium were performed in 1958 by the laboratory of water chemistry in the Engineering Department of the Board of Agriculture [8, 16]. The fluorides were determined colorimetrically by the use of zirconium-alizarin from 100 ml samples, which had been allowed to stand for 24 h. The detection level of fluoride was 0.02 mg/l. The methods for the determination of calcium and magnesium hardness are not described in detail in the original publication [16].
Statistical analyses
Age-specific mortality rates were first standardized for age by the direct method and expressed as indices where the national average was denoted by 1.00. The national population aged 35 and older in 1980 was used as the standard. The deaths and populations were then arranged to form multi-way tables according to sex, age (35-39, 40-44, … 80-84, 85 + years), resident commune and period (1961-70, 1971-80, 1981-90 and 1991-95), and the data on income, drinking water fluoride, magnesium and calcium were linked to each commune. The counts of deaths were subjected to a negative binomial regression [17, 18], in which sex, age, period, fluoride, magnesium and calcium were used as explanatory factors and the respective populations as an offset term. The analyses were performed by first including one variable at time (crude analysis), then including all variables (adjusted analysis). Binomial regression assumes the data to be generated by a Poisson process but allows for extra variation (over-dispersion) possibly caused by non-independence of observations or uncontrolled explanatory variables. To allow for non-linear relationships, all explanatory factors were treated as categorical (fluoride, magnesium, calcium and income in quintiles). The results were expressed as risk ratios and their 95% confidence intervals in each class relative to the lowest category.
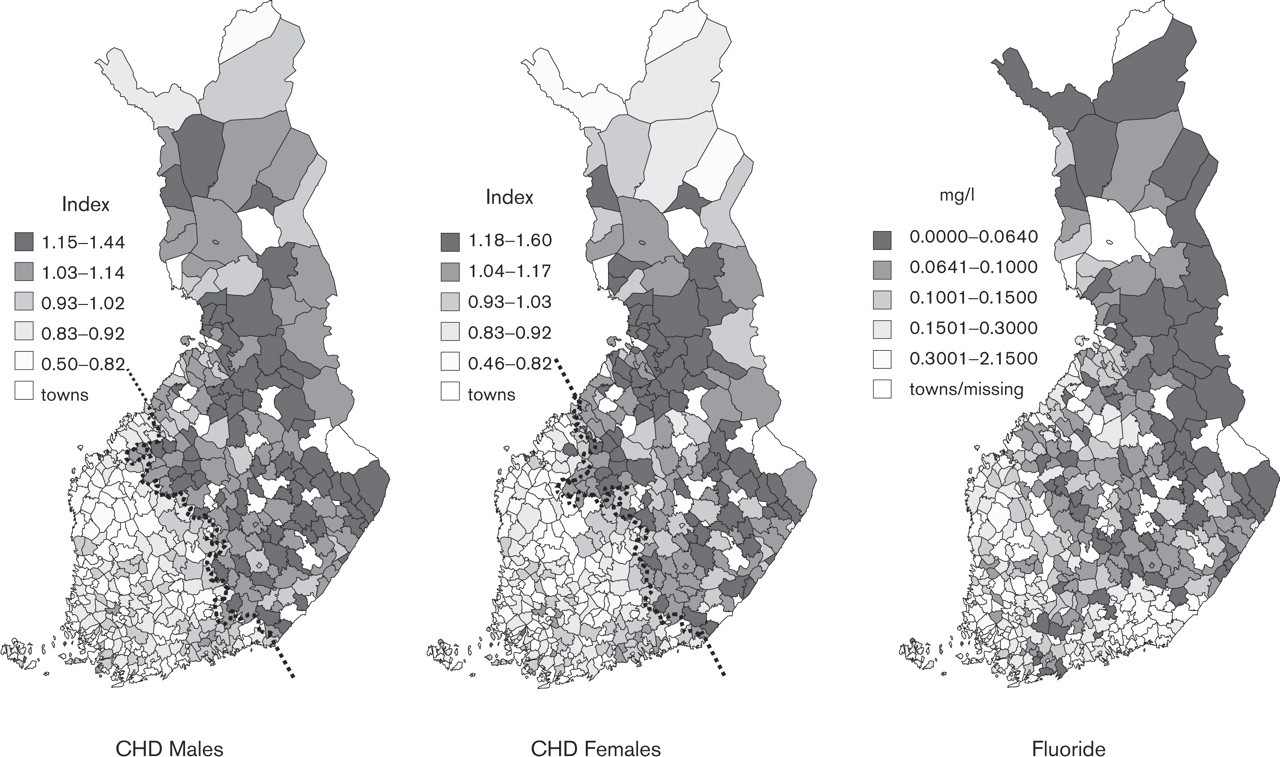
Mortality from coronary heart disease (CHD) in 1961-1995 and fluoride content of drinking water in 1958 in rural communes of Finland. Mortality expressed as an age-adjusted index (Finland = 1.00). Broken lines indicate the frontier between the south-west and the north-east used in the analyses.
Results
Regional trends in CHD and drinking water fluoride
Figure 1 shows the variation of CHD mortality in Finland by rural communes. The pattern is marked by high mortality in the north-east and low mortality in the southwest and a remarkably sharp frontier separating the two parts of the country. The regional trend of CHD is largely similar in men and women. The variation of drinking water fluoride shows some similarity to the pattern found for CHD, with very low concentrations (0.06 mg/l or less) in the high mortality areas and somewhat higher concentrations in the low mortality areas. There is also a sharp frontier between the lower and higher fluoride areas.
Age-adjusted mortality from coronary heart disease per 1000 among males and females aged 35 years and over, by period, separately in the north-east and the south-west∗
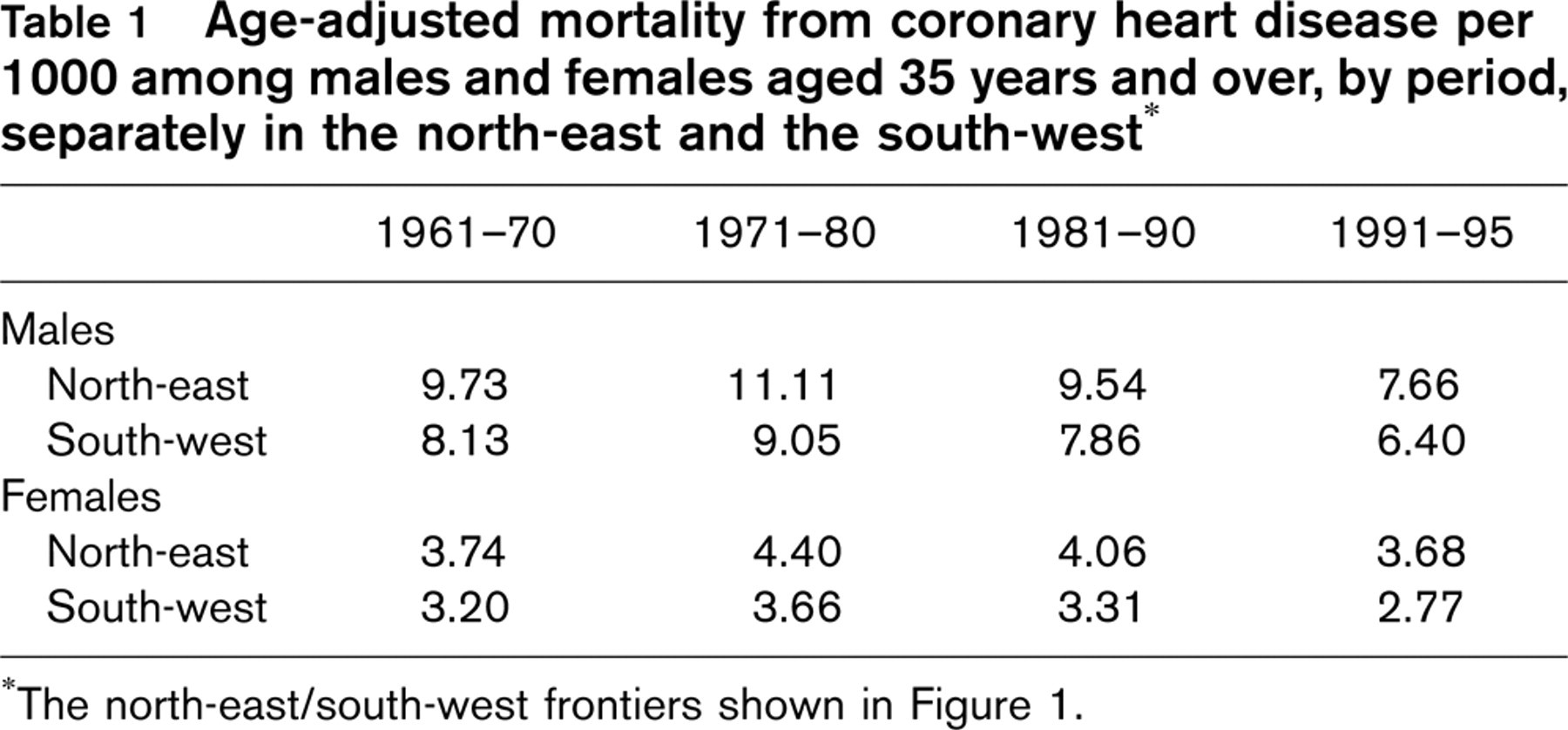
∗The north-east/south-west frontiers shown in Figure 1.
Mortality from CHD has declined since the 1970s both in the north-east and in the south-west, by a factor of one-third in males and somewhat less in females (Table 1). However, the relative excess in the north-east has remained the same in males (approximately 1/5) but has increased in females, from 17% in the 1960s to 33% in the 1990s.
Means, medians and ranges of the explanatory variables
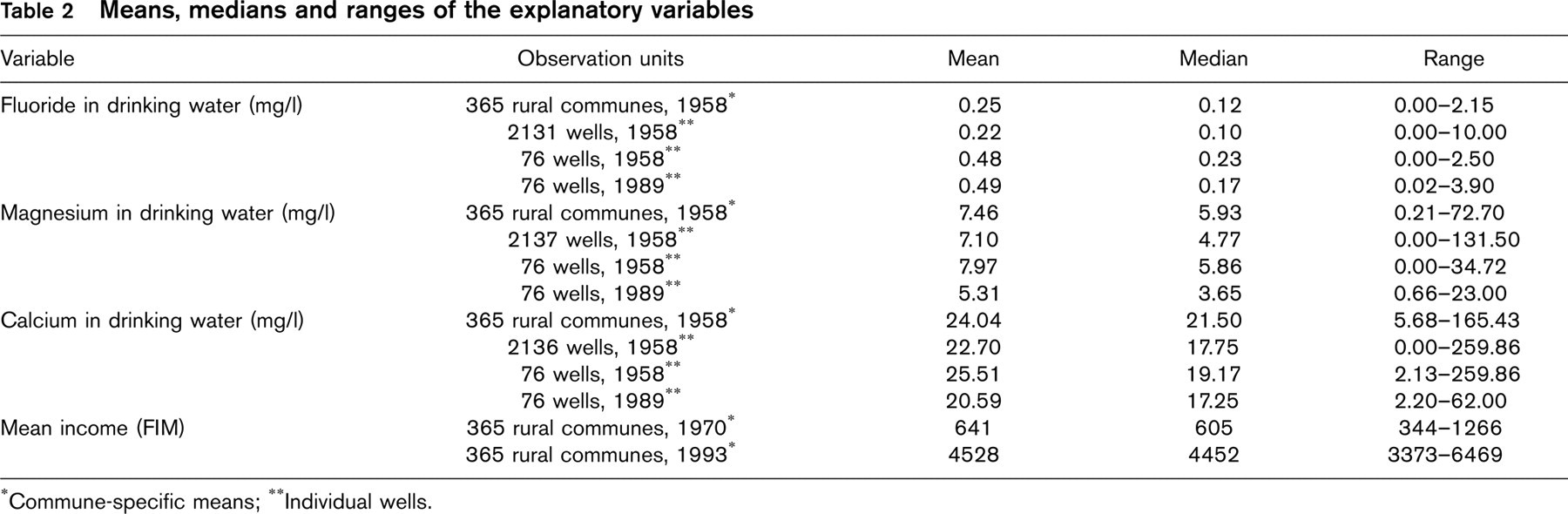
∗Commune-specific means;
∗∗Individual wells.
The explanatory factors
In 1958, the mean fluoride content in the 365 rural areas was 0.25 mg/l (range 0-2.15 mg/l) (Table 2), 95% of the area-specific means being less than 1.00 mg/l. The concentrations of magnesium and calcium indicated the softness of drinking water, although high values of magnesium and calcium were found in individual communes. The median concentration of fluoride is half of its mean, indicating a right-skew distribution, and a trend of a similar kind is seen in magnesium, but not in calcium. Due to differing sampling schemes, the concentrations of fluoride were much higher in the sub-sample examined in 1989 than in the original sample. However, there was practically no change in the fluoride content over the years, while the trend was more or less a declining one for magnesium and calcium. The difference between the pair-wise measurements in 1989 and 1958 for each well averaged 0.01 mg/l (95% confidence interval −0.09 to 0.11 mg/l) for fluoride, −2.66 mg/l (−3.99 to −1.33 mg/l) for magnesium and −4.92 mg/l (−11.94 to 2.10 mg/l) for calcium.
Association of CHD and fluoride
Table 3 examines the association of drinking water fluoride and CHD using negative binomial regression. The adjusted mortality from CHD was 2.57 times higher in males than in females, increased steeply with advancing age and it showed a wave-like course over time, with highest mortality in the early 1970s and a decline thereafter. The risk ratios for drinking water fluoride showed an inverse J-shaped association with CHD, with the lowest mortality (15% below the baseline) in the second highest quintile of fluoride (0.15-0.30 mg/l) and some rise in the highest quintile, the 95% confidence intervals for the risk ratios remaining below the baseline in all quintiles. Mortality from CHD declined with increasing magnesium content in drinking water, but showed some increase with calcium content. The association of CHD with mean income was nearly linear, CHD declining with rising income. The over-dispersion parameter was significant (χ2 (df= 1) = 7642.1, P ∼ 0.000). The crude and adjusted risk ratios give largely similar results although differences exist in the magnitude of the effects.
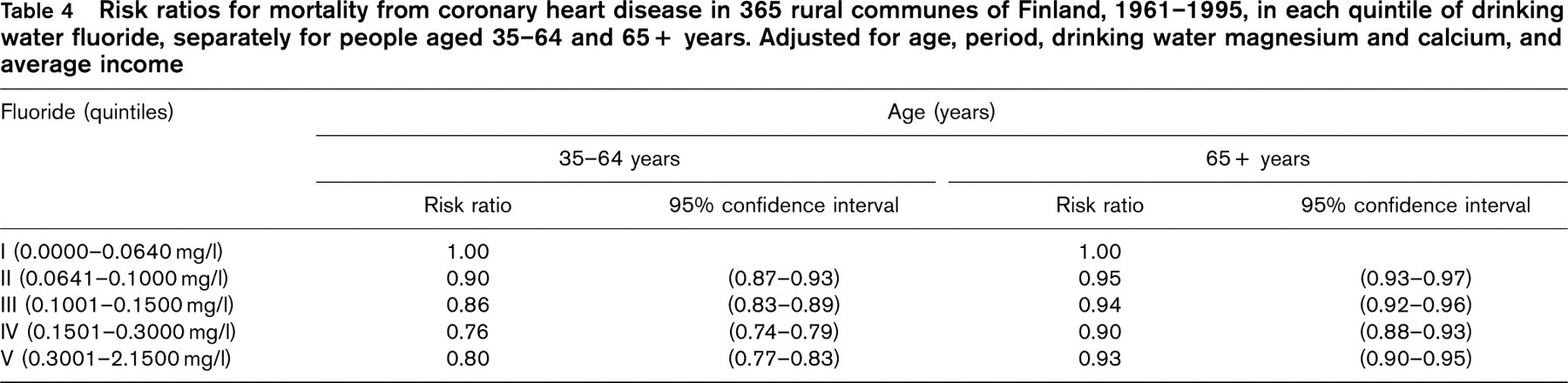
Separate analyses performed among people aged 35-64 years and those aged 65 years and over showed a markedly stronger association of fluoride and CHD in the younger group (Table 4).
The above analysis presupposes homogeneity of the effects (e.g., similar associations of fluoride and CHD in different periods). A further analysis was therefore carried out adjusting for interaction between fluoride and period. Figure 2 shows the transformation of the fluoride-CHD relationship over time. While the overall shape of the association remained similar, the effect of fluoride attenuated during the 35-year period. In 1961-1970, the adjusted mortality from CHD was 22% lower (95% confidence interval 18-27%) in the fourth quintile of fluoride (0.15-0.30 mg/l) than in the first quintile (0.00-0.06 mg/l) but this deficit reduced to 13% (7-18%) for 1991-1995. There was still significant over-dispersion (χ2 (df= 1) = 8012.3, P ∼ 0.000) but the adjusted confidence intervals of the risk ratios were usually below 1.00 except for the last period, which showed significant effect only in the two highest quintiles.
Discussion
The few epidemiological studies performed on the association of drinking water fluoride and cardiovascular diseases have used different methodologies and have given conflicting results. A case-control study [5] performed in south-eastern Finland found risk ratios of 3.0-4.4 for suffering a myocardial infarction in patients whose drinking water had fluoride levels less than 0.1 mg/l, compared with those who had more, but the sample size was too small for any definitive conclusions to be drawn. In a locality with a mean concentration of fluoride in well water of 2.5 mg/l the prevalence of CHD was 1/8 compared to that in another locality with a concentration of 0.05 mg/l [4]. In Texas, USA, Miller [19] found no difference in CHD mortality between cities with different levels of natural fluoride in their water supplies, but his sample did not contain cities with a fluoride content of less than 0.1 mg/l. On the other hand, mortality from CHD in the USA had declined more rapidly in cities where drinking water had been fluoridated than in other cities [20].
Negative binomial regression (main effects) of mortality from coronary heart disease in 365 rural communes in Finland, 1961-1995
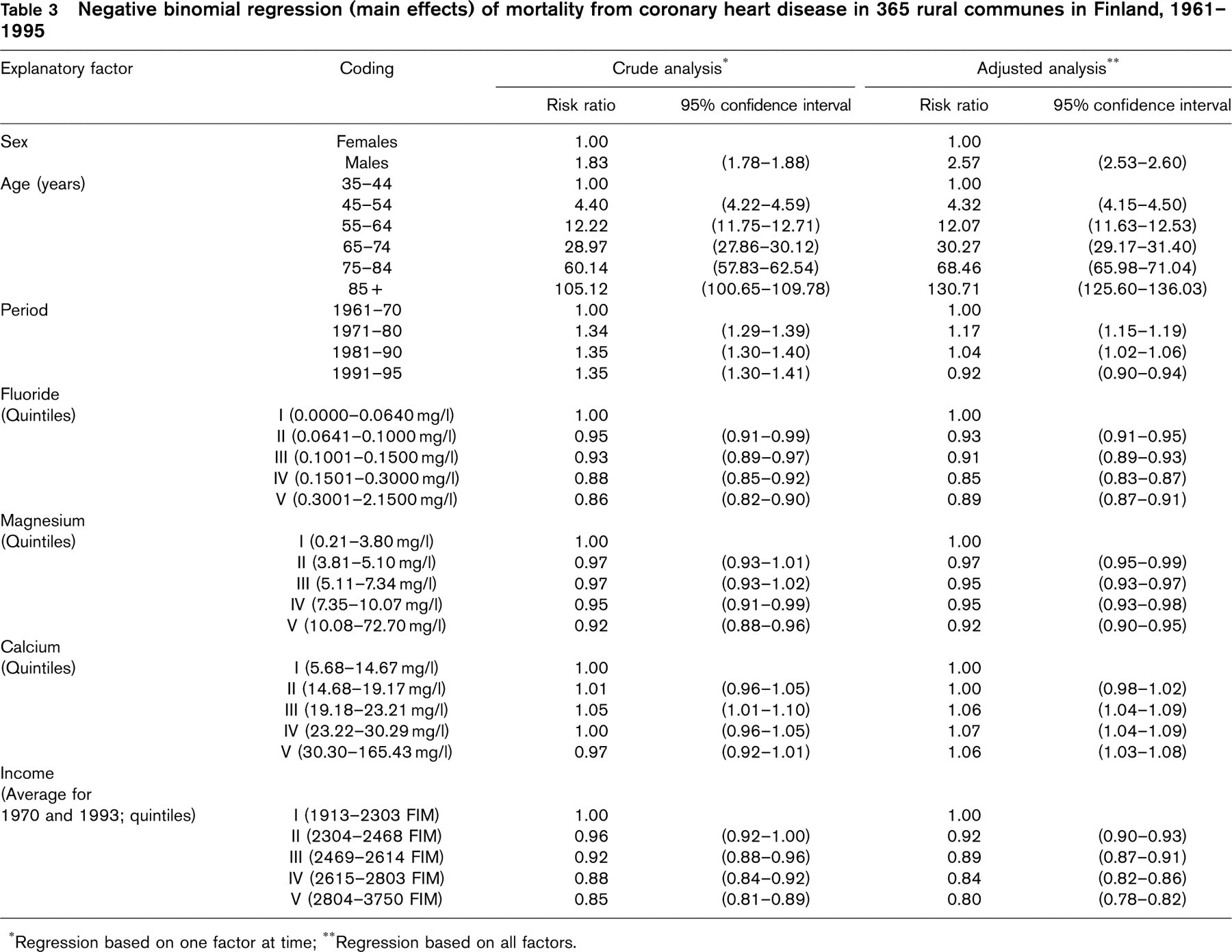
∗Regression based on one factor at time;
∗∗Regression based on all factors.
Risk ratios for mortality from coronary heart disease in 365 rural communes of Finland, 1961-1995, in each quintile of drinking water fluoride, separately for people aged 35-64 and 65+ years. Adjusted for age, period, drinking water magnesium and calcium, and average income
The present study makes a stronger case than any of the previous studies. Our data are based on a national population and cover a relatively long period. The data on deaths and the explanatory factors can be considered to be reliable for the present purpose. The statistical analysis allowed for deviations from the standard assumption that counts of deaths follow a Poisson distribution. Extra variation could have been due to correlations between adjacent areas, or omission of unknown explanatory factors such as smoking, elevated serum lipids or blood pressure. In fact, previous studies have noted a higher prevalence of the latter factors in eastern than western Finland, but the differences have been relatively small, i.e., 0.1 to 0.3 mmol/l for serum cholesterol, and usually less than 5 mmHg for systolic and 3 mmHg for diastolic pressure, which together could explain one half of the east-west difference in CHD mortality at most. Among the male population, smoking was 5 to 10 percentage points more prevalent in the east than in the west in the 1970s but this excess has reversed later on, and eastern women have usually smoked less than their western counterparts [2]. In any case, in the absence of detailed geographical distribution of the latter factors we cannot assert a causal link between fluoride and the regional pattern of CHD. Consistency of the association still suggests that a true effect is a possibility.

Risk ratios for mortality from coronary heart disease in Finland by period, 1961-1995, based on model: sex + age + period + income+ magnesium + calcium + fluoride + fluoride ∗ period.
The most likely explanation would be indirect. Fluoride in drinking water prevents dental caries [21] and possibly also periodontal disease [22]. As dental infections may promote the development of CHD [6], there should be more CHD in areas with less fluoride in drinking water. Population surveys actually show that dental caries is more common in eastern than western Finland [10]. We saw the decrease in CHD starting from fluoride levels of 0.06 mg/l and reaching the optimum level at 0.15-0.30 mg/l, which are well below the 1 mg/l recommended for prevention of dental caries [23]. This may indicate either that the recommended level of 1 mg/l to prevent dental caries is too high, or other mechanisms would be operative when considering possible association of dental infection and CHD. Molecular fluoride may, for example, inhibit the initiation or progress of atherosclerosis preceding clinical CHD, although the evidence is based on animal experiments only [24].
Dental caries is a bacterial infective disease that progresses when acid produced by bacterial action on dietary fermentable carbohydrates diffuses into the tooth and dissolves the mineral [25]. The key feature in caries is dietary carbohydrate-induced enrichment of the plaque flora with organisms such as mutans streptococci and lactobacilli which decrease the plaque's pH and cause an increase in its cariogenic potential [26]. Fluoride prevents caries primarily via topical mechanisms which include: (1) inhibition of demineralization at the crystal surfaces inside the tooth, (2) enhancement of demineralization at the crystal surfaces, and (3) inhibition of bacterial enzymes [25].
In their study of Australian 6-15-year-old children with different residential histories, Singh et al. [27] stated that a pre-eruption exposure to fluoridated water is required for the prevention of dental caries, while a post-eruption exposure had no significant effect. This is in line with our argument that drinking water fluoride is beneficial in early life and should prevent CHD especially in the younger age groups.
The fluoride content of natural waters often correlates with its magnesium and calcium content [4] and this was the case in the present study, too. Magnesium and calcium also showed an association with CHD but this did not confound the association between fluoride and CHD. This could be explained in part by the fact that drinking water is not the most important source of magnesium and calcium in Finland. The total daily intake of magnesium in Finland is estimated to be 440 mg, of which only 3-6 mg comes from drinking water. The average intake of calcium is 1.5 g per day and the significance of drinking water as a source of calcium is very small [28].
Drinking water is the principal source of fluoride in man. In the early 1960s, an estimated 60-80% of the daily intake of fluoride came from drinking water [9] and a Finnish report published in 1980 ended up with a figure of 40% [29]. Other important sources are fish, especially sea fish, and shrimps and tea, which were not commonly used in Finland in the 1960s. The normal Finnish diet contains only 0.56 mg of fluoride per day, an amount which is very small by comparison internationally [30]. The association of fluoride and CHD was particularly strong in the 1960s. More recently, the intake of fluoride has been more affected by consumption of industrially prepared food items, soft drinks and also by the use of fluoridated toothpastes (some of which is swallowed). This may have diluted the effect of drinking water fluoride on dental infections and possibly, on CHD, despite the fluoride content of well waters remaining very stable over the period studied. Another factor possibly diluting the association is migration, the effect of which is difficult to evaluate. On the other hand, selective out-migration of healthy and educated women from the eastern country districts could also emphasize the regional contrast in CHD, as is now happening in Finland. An additional factor in this development would be the poor dental health among the eastern women [10] which would slow the recent decline of CHD.
In conclusion, there is an ecological association between drinking water fluoride in the late 1950s and mortality from CHD during the subsequent decades in Finland, the association that is alleviating over time, possibly due to the lessening significance of drinking water as a source of fluoride. Our finding could also explain part of the regional variation of CHD mortality in this country and especially the conspicuously sharp frontier between the high and low mortality zones.