
Abstract
Background
Guidelines on the prevention of cardiovascular disease recommend screening in close relatives of patients with premature coronary heart disease (CHD). This family history puts them at increased risk for CHD, independent of other major risk factors, but screening for CHD risk factors in these relatives is not widely practiced in Europe. This demonstration project examined how to improve screening of close relatives of patients with premature CHD in daily practice.
Methods
A controlled study design was used. Four hospitals were compared in a pre-test as to the actual screening of relatives of patients with premature CHD. Then they were arranged in pairs and randomly assigned to the Usual care (U) or Intervention group (I). An information and health education program - involving patients, relatives and family doctors - was developed in I to improve screening by the family doctor.
Results
The pre-test confirmed that screening of relatives of patients with premature CHD is poorly practiced in the four regions; no significant differences between I and U were observed. The screening of relatives during the study period reached 63.9% in I compared to 25.4% in U. This difference between I and U was present in siblings and offspring. The cardiovascular risk profile of the relatives of I was not optimal and needed improvement.
Conclusion
Screening of first-degree relatives of patients with premature CHD can be significantly improved through a health education program. This is the first and necessary step to improve the management of risk factors in these people, who are at increased risk for CHD.
Introduction
Coronary heart disease (CHD) is one of the major causes of morbidity and premature mortality in most European countries. The variance of the incidence of CHD within and between populations can not be explained solely by the traditional risk factors. CHD clusters within families, illustrating the importance of genetics, of shared environmental factors and of the interaction between genetic predisposition and shared lifestyle factors. Results from recent studies show that a positive family history is an independent risk factor besides the conventional risk factors [1–3].
Close relatives of patients with premature CHD are therefore at an increased risk of CHD [4, 5]. Many of them also have several modifiable risk factors [6–8]. Guidelines on the prevention of cardiovascular diseases (CVD) recommend screening in this high-risk population [9–11]. However, screening for CHD risk factors in close relatives of patients with premature CHD is not widely practiced in Europe [12, 13], or in the United States [14].
This project was developed in order to stimulate interest in the familial occurrence of CHD among practitioners and the public. We sought to determine whether a health education program can increase the active screening of the first-degree relatives of patients with premature CHD. Besides this main objective, the perception of the participants and the factors associated with (non)participation were explored.
Methods
Design and study population
This project was an exploratory investigation in the field of primary prevention of CHD.
A clustered study design was used including four hospitals, randomly divided into a usual care and an intervention pair. The study consisted of three phases: (1) a pre-test; (2) an intervention (in the intervention group); and (3) a post-test.
In the pre-test a consecutive series of patients, hospitalized because of an acute coronary event at a premature age, was identified retrospectively in each of the four participating hospitals. With the consent of the patient, obtained by mail, their close relatives were asked to complete a questionnaire on risk factor screening. Based on these results, the four hospitals were arranged in two pairs that were randomly assigned to a usual care group (U) or an intervention group (I). The post-test compared the two groups after the implementation of the health education program in I.
The four regions were geographically distinct from each other but the populations that they were serving were comparable in terms of socio-economic level. An identical health care system is operational in the whole of the country.
The patients were documented as having premature coronary heart disease, in particular coronary bypass grafting (CABG), percutaneous transluminal coronary angioplasty (PTCA), acute myocardial infarction (AMI) or myocardial ischemia. Premature CHD was defined as an event occurring before the age of 55 years among men and before 65 years among women. Only hospitalized patients, who survived an acute event were considered.
The study design was approved by the ethical committee of the University Hospital of Ghent.
Procedure and data collection
In the pre-test all consecutive patients with a discharge diagnosis involving a premature coronary event were considered eligible. The records from all patients hospitalized before 15 March 2003 were retrospectively inspected. We went back for 72 weeks to collect a sufficient number of possible candidates. Once the diagnosis was confirmed in the medical record, the patients were sent a letter, in which the permission was asked to send a postal questionnaire to their first-degree relatives (siblings and children ≥18 years of age). A minimal period of 6 months was allowed for the dissemination of information from patient to first-degree relatives and for the latter to take initiatives for screening of their coronary risk.
If permission was given by the patient, a questionnaire with an accompanying letter was sent to the close relatives who could return the form in a self-addressed, stamped envelope. The questionnaire's main focus was to determine whether the cardiac condition of the index-patient had resulted in a screening of CHD risk factors among first-degree relatives by their family doctor. In this way it was possible to compare the level of screening of the family members in I and U.
In the intervention phase an information and health education program was implemented for the patients and family members of the two hospitals of I over 14 months.
The intervention program consisted of information given by the cardiologist and by a social nurse to all eligible patients. When the patients agreed to participate in the study, they provided the addresses of their family members and a letter and brochure were sent to them. The specific brochure, developed by the research team, contained information about the importance of a family history of premature CHD, prevention of CVD, how to estimate total cardiovascular risk and a strong invitation to visit their family doctor for further information and screening for the major risk factors. The last page of the brochure was a reply form that had to be completed by the family doctor.
All the messages were positively formulated: the positive consequences of early screening and lifestyle change were stressed.
The primary objective of the intervention package was to encourage first-degree relatives to visit the family doctor with their brochure in order to be screened for CHD risk factors. On the basis of age, sex, smoking status, total cholesterol and systolic blood pressure, the family doctor estimated the total risk for developing a fatal cardiovascular event using the SCORE model [15], recently adapted to the Belgian situation [16]. These SCORE-Belgium charts allow the estimation of total cardiovascular risk. In younger subjects, such as offspring, total risk is generally low because of the strong protection of young age. In these subjects the total cardiovascular risk can be estimated by extrapolating their risk status to age 60 which gives an estimation of their total risk if no change is made in their smoking habits, systolic blood pressure and total cholesterol level. This can be useful in advising younger subjects.
Decisions in terms of risk factor management were left at the discretion of the family doctor. The reply form, completed by the family doctor during the visit, had to be returned in a self-addressed, stamped envelop to the study nurse.
The outcome of the intervention was measured on the basis of the return of the reply form when the family doctor had seen the person for risk factor screening.
Within the context of this campaign, a number of information meetings were organized with existing local family doctor networks from the intervention region. In addition, a free-of-charge telephone number was available for any questions or remarks concerning the project.
The post-test in the usual care group was carried out in the same way as the pre-test: all patients who had been hospitalized in U because of a premature coronary event during the 14 months during which the intervention program was developed in I, were identified through the medical records. The patients were asked by mail for permission to contact their close relatives and, with their agreement, letters were sent to first-degree relatives. The most important question was whether they had been screened as a consequence of the premature event of their family member. The reasons for not being screened were asked, as well as some questions focusing on perception. Afterwards the screening rates of the relatives in I and U were compared.
Statistical analysis
All statistical analyses were undertaken using SPSS statistical software (SPSS Inc., Chicago, Illinois, USA). Based on results from the EuroAspire II survey [12] and assuming an average of 2.5 blood relatives per patient, we calculated that 62 patients were needed to demonstrate a threefold increase in screening rate among first-degree blood relatives with 80% power at the 5% significance level. For comparison between patients or first-degree relatives groups chi-squared tests were used and a P-value of <0.05 considered as indicating statistical significance.
Results
Pre-test
The purpose of the pre-test was to compare the level of screening of the family members of the patients from the four hospitals. Table 1 shows that both groups were comparable in participation rates. The results of the pre-test indicate that only 22.1% of the first-degree relatives in what became the usual care group, and 15.0% of the relatives in what became the intervention group, had been examined for their cardiovascular risk as a direct result of the premature coronary event in their family member. Differences between U and I were not significant.
Participation of patients and relatives, and screening of relatives, in the pre-test
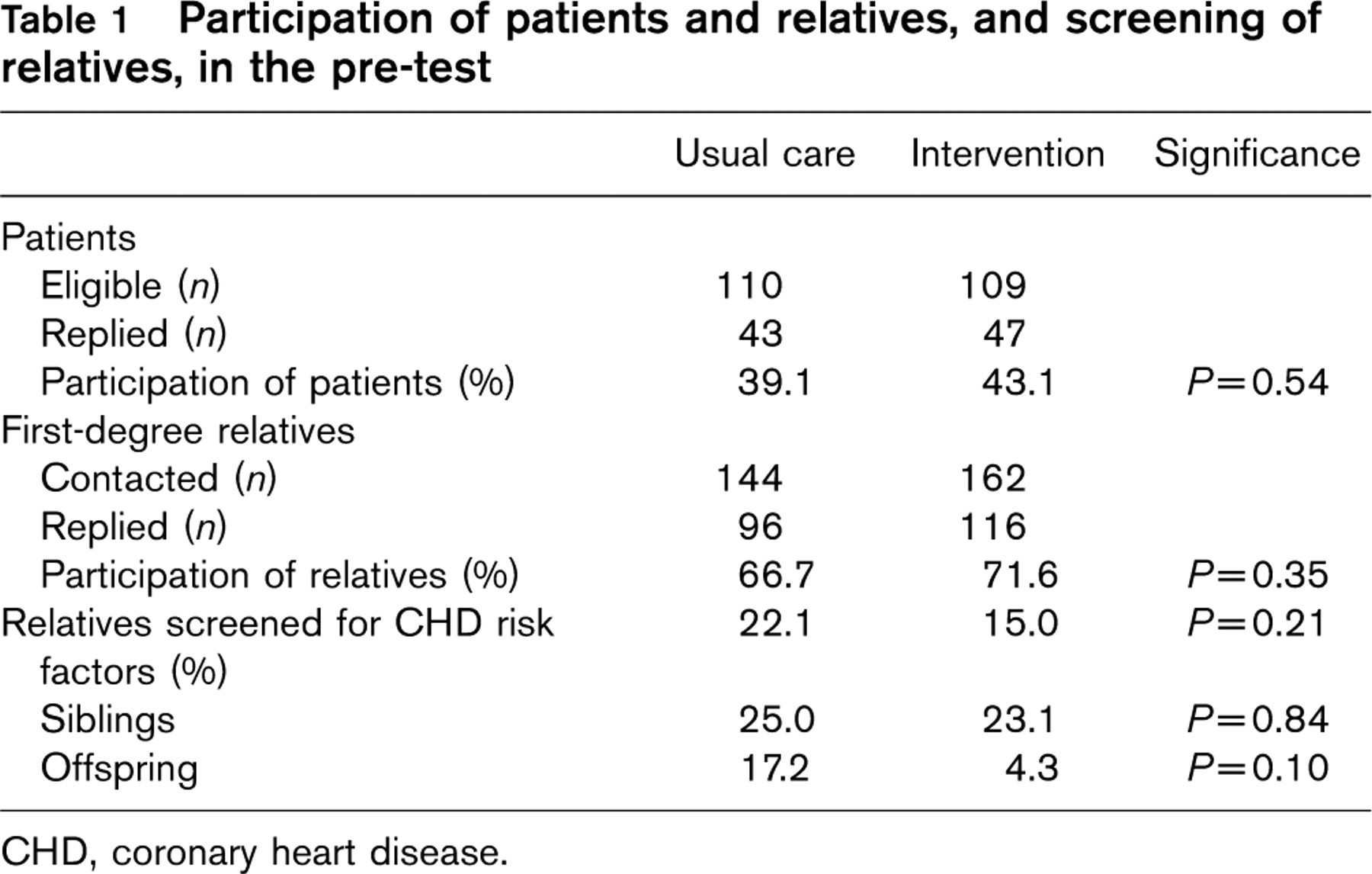
CHD, coronary heart disease.
Intervention
In I, 64 patients with premature CHD were consecutively and prospectively invited to participate in the project. Sixty-one patients did accept and only three refused. The participation rate of the patients in the intervention group was 95.3% (Table 2). Among the eligible patients, 71.4% were men and the average age was 50.3 years. Self-reported data showed that 19.6% were obese, 48.2% were smokers before hospitalization and 15.1% had known CHD. Of this patient group, 21.6, 58.8 and 19.6% received their highest education in a primary, secondary or high school/university, respectively. In total, 66.1% were currently employed.
The patients of I gave permission to send the specific brochure and information to 223 first-degree relatives. Four relatives could not be reached because they were living abroad. From the 219 first-degree relatives that could be reached, 35 refused to participate in the study, including two persons who had already suffered a coronary event. The reasons for refusal were various: 10 persons already had regular check-ups, three persons claimed financial reasons, three persons had time constraints, two persons were too anxious, two persons could not participate because of health problems and 15 persons did not give a reason. Among the 184 who intended to visit their family doctor, 140 relatives did so and returned the form that had been completed in collaboration with the family doctor; this represents a response rate of 63.9% of the original 219 relatives. The group of respondents consisted of 77 men (55.0%); 93 siblings and 47 offspring. The average age of the siblings and offspring were 51.4 and 27.7 years, respectively. Coronary risk factors of the relatives, as reported by the GP, are shown in Table 3. The results are compared with the goals set in the guidelines of the Joint Task Forces of European and other Societies on Cardiovascular Disease Prevention [10, 11]. Total cardiovascular risk, estimated through the SCORE chart adapted for Belgium [16], was 5% or more (now or projected to the age of 60 years in younger subjects) in 38.4 and 19.5% of the siblings and the offspring, respectively, or in 29.1% of all close relatives, but in this risk estimation the effect of the positive family history is not yet considered.
Participation in the intervention and usual care groups
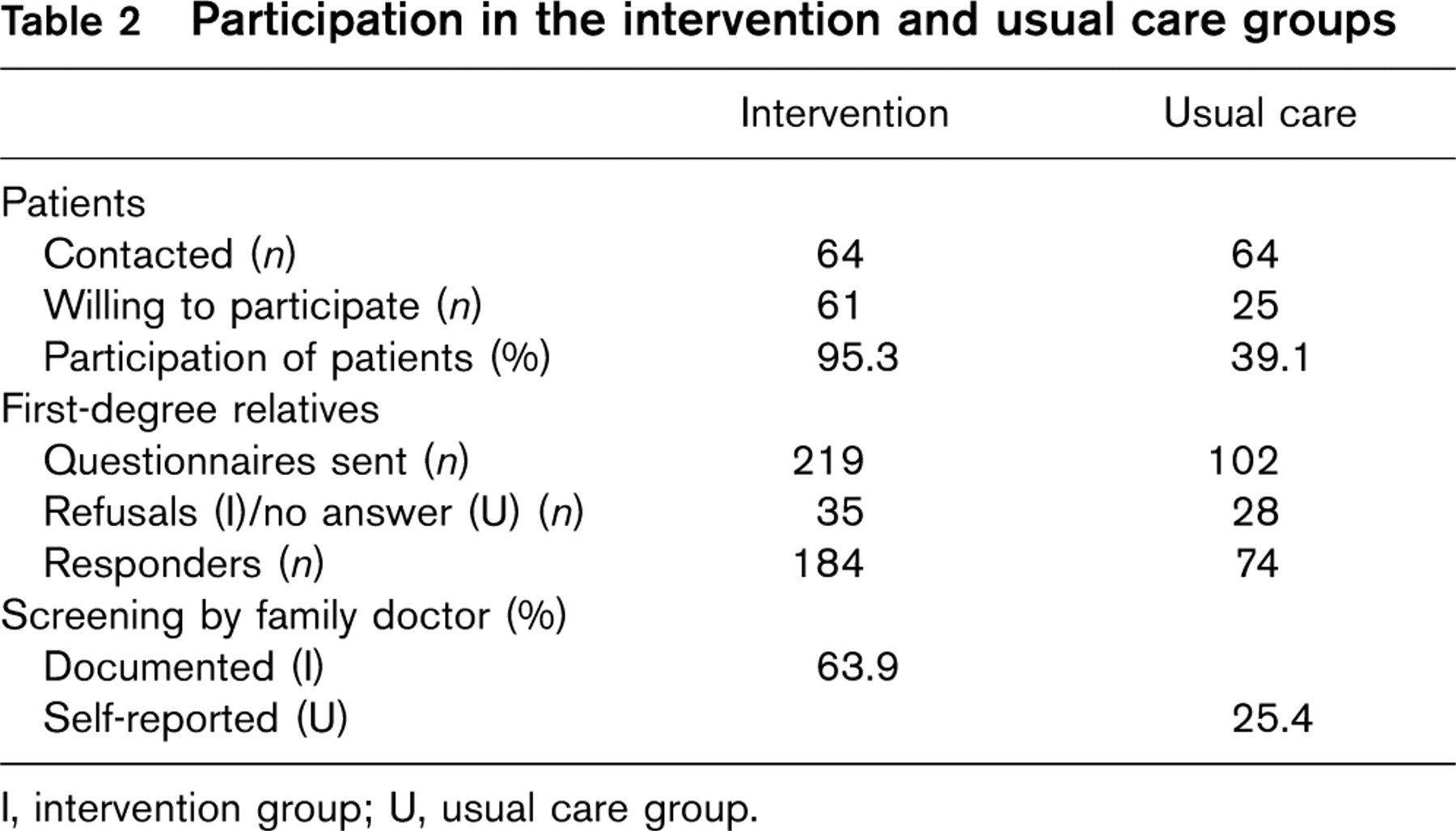
I, intervention group; U, usual care group.
Prevalence of coronary risk factors in the relatives who participated in the intervention group
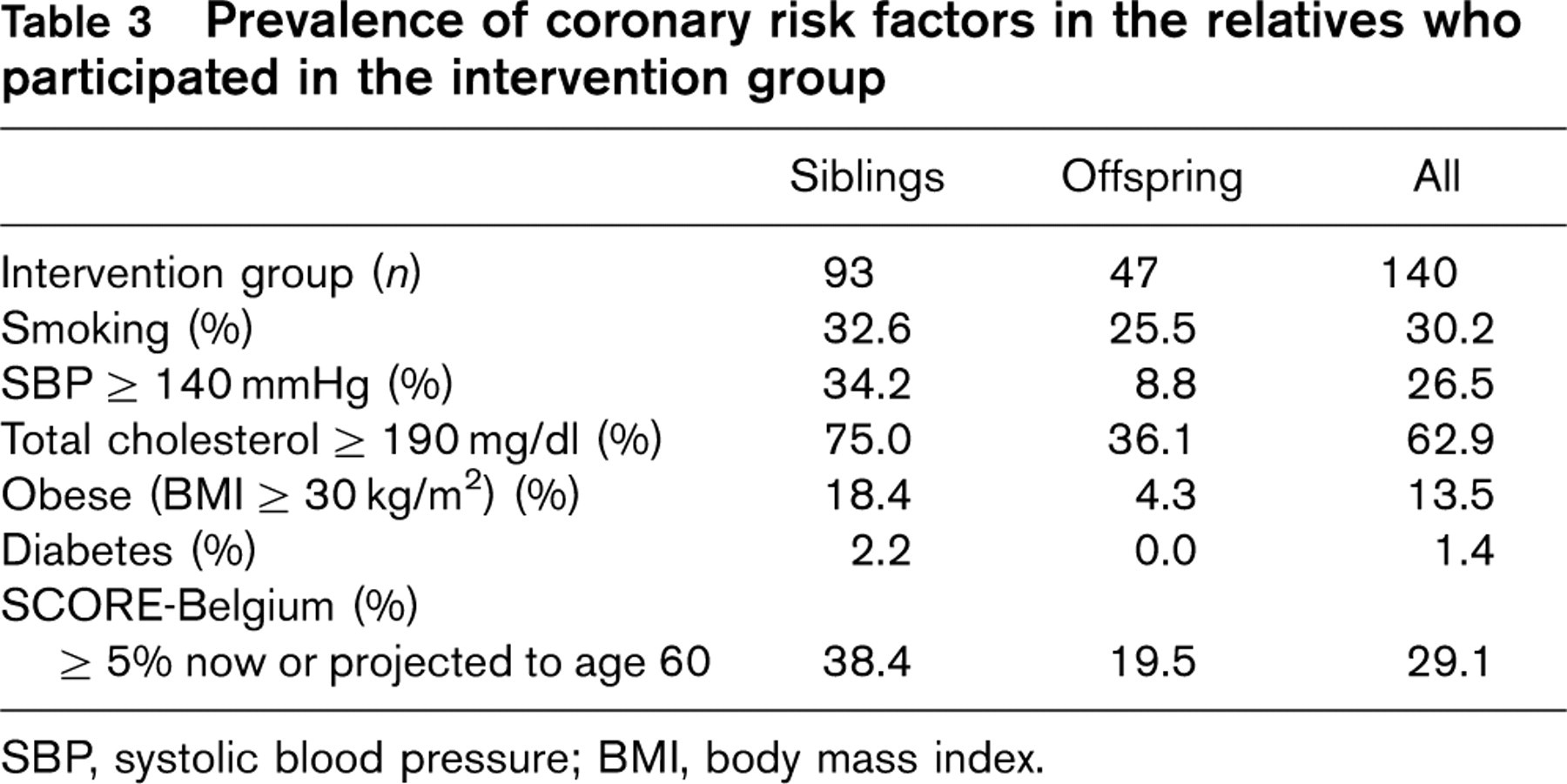
SBP, systolic blood pressure; BMI, body mass index.
In U, 64 patients were hospitalized because of a premature coronary event during the same time period that the intervention program had been developed in I. They were contacted by mail after the intervention period and 25 were willing to participate. Therefore the participation rate of the patients in U was 39.1% (Table 2). This patient group consisted of 16 men (64%) and the average age was 51.1 years. Self-reported data showed that 21.0% were obese, 45.8% were smokers, 13.0% had experienced previous CHD and 87.5% were currently employed. There were no significant differences between the characteristics of the participating patients in I and U.
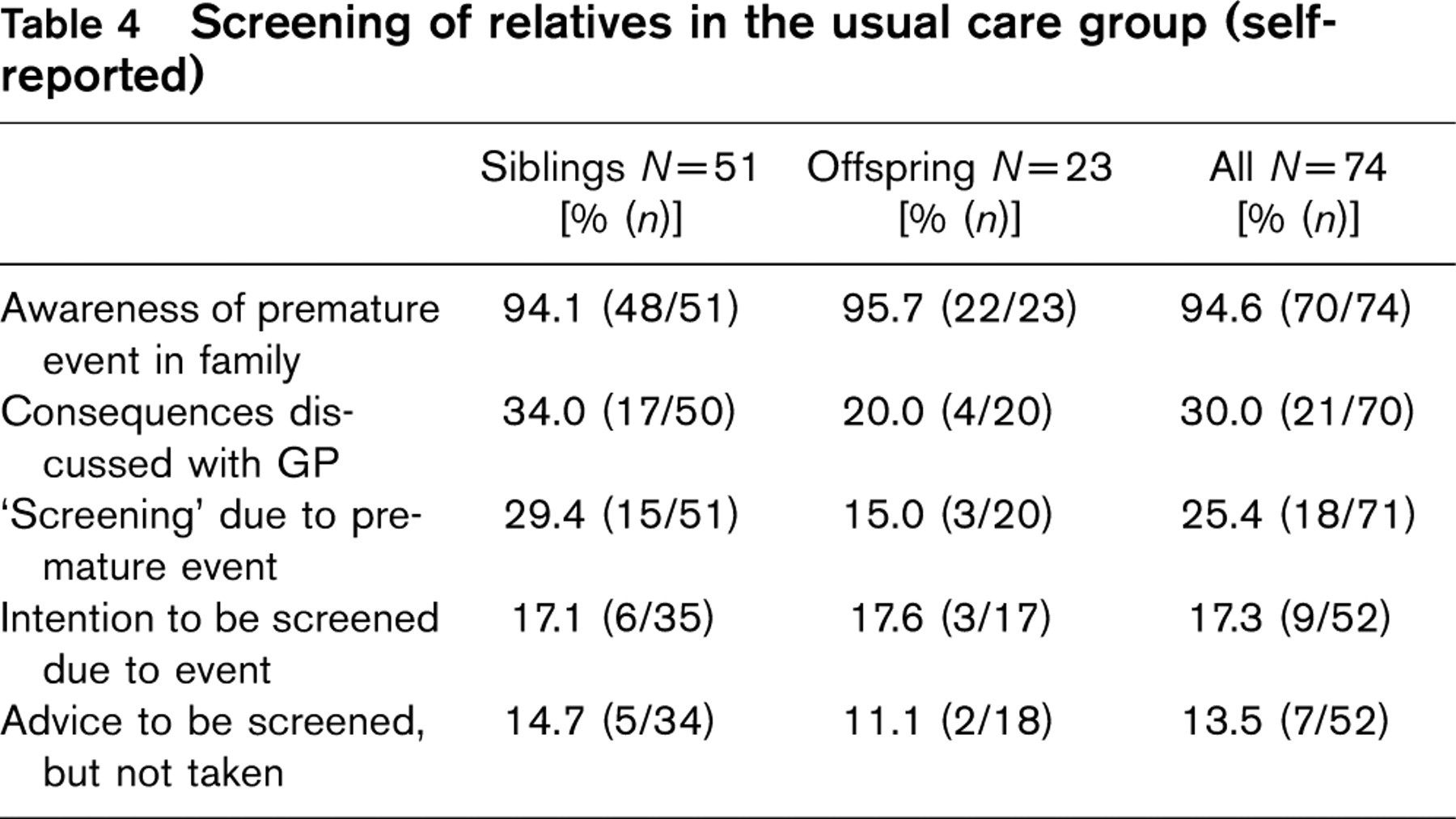
Questionnaires were sent to 102 first-degree relatives of the 25 patients of U; 74 questionnaires were returned. The participation rate among these first-degree relatives was 72.5% (Table 2). The group of responding relatives consisted of 51 siblings and 23 offspring; 36 (48.6%) were men. The average ages of the siblings and offspring were 53.2 and 28.8 years, respectively. In the questionnaire to the first-degree relatives in U it was asked if they had been screened as a consequence of the premature coronary event of their family member. Results are shown in Table 4; 25.4% of the relatives reported being ‘screened’ for CHD risk factors by their family doctor due to the premature event of their family member (29.4% of the siblings and 15.0% of the offspring).
Screening of relatives in the usual care group (self-reported)
Screening of close relatives due to the event in usual care and intervention groups in the pre-test and during the study period
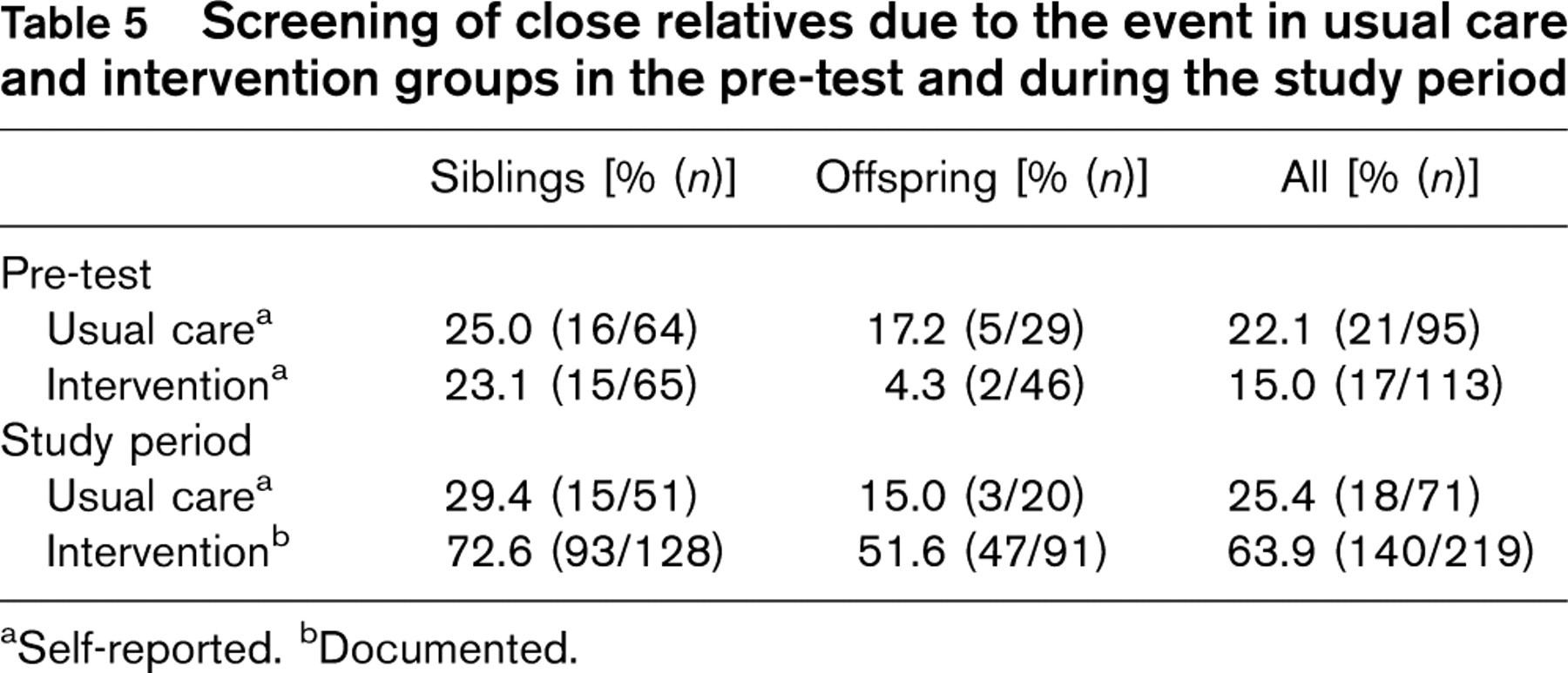
aSelf-reported.
bDocumented.
In Table 5 the main results of the study are summarized. The results from the pre-test indicate that screening of close relatives of patients with premature CHD is poorly practiced; it was reported by only 15.0 and 22.1% of the subjects in the I and U groups, respectively, or, more specifically, in only one in four of the siblings and in less than one in five of the offspring. This was confirmed in the post-test in U.
In I, 63.9% of the close relatives went to see their family doctor specifically because of their family history. This was documented by a reply form from the family doctor. This is a significant improvement when compared to the screening rate of only 25.4% reported by the subjects in U. This difference was present in both the offspring and the siblings.
Discussion
In most European countries the implementation of the guidelines on prevention of CHD in clinical practice is poorly developed in patients with CHD [12, 13]. The situation in asymptomatic high-risk subjects is probably as poor; as a third priority it is recommended to pay attention to close relatives of patients with premature CHD. In EUROASPIRE II [12] it was shown that in this subgroup screening for cardiovascular risk factors was poorly practiced.
Results from recent studies show that screening of first-degree relatives may identify modifiable coronary risk factors and as a consequence it may offer an important and cost-effective preventive potential [17]. Starting risk factor management at an earlier age may cost more but will prevent the occurrence of premature events and therefore reduce indirect costs, reduce Disability Adjusted Life years and improve life expectancy in good health.
In Belgium there is no systematic tracing and screening of these close relatives of patients with premature CHD. This project was aimed at exploring the possibilities in this field, studying the surroundings of such a systematic screening and mapping the difficulties.
The pre-test of the project gave evidence of the fact that first-degree relatives of patients with premature CHD are rarely screened for coronary risk factors, although they bear an excess risk of CHD. There are many opportunities for improvement possible in this area. The level of screening of the relatives in U and I were comparable in the pre-test. The comparability of the two groups at baseline was necessary for the evaluation of the intervention package.
The results showed a very high participation rate (95.3%) of the patients in I. This corresponds to the results reported by Tonstad and Westheim [18] who found that most patients with premature CHD were willing to contact their relatives for screening (78% agreed to contact their siblings and 93% agreed to contact their children). In our project the high participation rate can be explained by the face-to-face contact with the study nurse, who motivated the patients to participate in the study, with the support of the attending cardiologist. This resulted in a group representative of all patients hospitalized because of premature CHD in these hospitals.
The interest of the first-degree relatives of I was also high: only 35 out of 219 refused to participate. Furthermore two-thirds of the relatives visited their family doctor for risk factor screening, the main objective of the intervention program.
The high participation rate means that the health education program of the intervention group is well accepted by the patients and the relatives. The hospitalization period of the patient is an excellent opportunity for informing them of the importance of a family history of premature CHD for the first-degree relatives and, with their consent, a large majority of the relatives can be identified and informed.
The first-degree relatives in I who were seen by their family doctor had risk factors comparable to those seen in the population of their age. But in addition to the conventional CHD risk factors, they are at a doubled risk because of their family history of premature CHD [4]. Their total CHD risk was consequently much higher. They therefore form a suitable target population for primary prevention of CHD and are to be considered as a particular risk group.
Using the SCORE risk charts for Belgium, 38.4% of the siblings of I had a risk score higher or equal to 5%, which means that in 38.4% the risk of dying from cardiovascular disease in the coming 10 years is high. However, when the family history is also considered, we may assume that more than two-thirds of all siblings are at high risk. In the offspring, total cardiovascular risk is still low given their young age; however when the extrapolation is made to age 60, and considering the additional effect of their family history, we may also consider that almost half of them are or will be at high risk.
The participation rate of the patients in U was 39.1%, much lower than in I. This could be due to the fact that they were only invited to give permission to contact their close relatives; no personal and individualized contact was made. No significant differences were seen between the characteristics of the participating patients in I and U.
The first-degree relatives of U replied to the questionnaire in 72.5%; 25.4% of them said they had been ‘screened’ for CHD risk factors by their family doctor as a consequence of the premature coronary event of their family member. Because this was self-reported, it could be an overestimation of the ‘real’ screening for CHD risk factors. Possibly the word ‘screening’ or ‘as a consequence of the coronary event’ was interpreted in different ways. If the family doctor of the relatives by coincidence measured their blood pressure, they may have thought that they had been screened for CHD risk factors. Recent literature shows that there are differences in perceptions of familial risk, and there are potential areas of misunderstanding between the health professional and the patient about the presence and the relevance of a familial history of CHD [19].
This project benefits from several methodological strengths. The information and health education program has been well accepted by the patients and their relatives in I, leading to a high response rate and a high satisfaction rate. The health education program has been developed anticipating, as much as possible, the applicability in daily practice. The implementation of the intervention program should therefore be possible in most health care systems without major additional costs.
There are also some study limitations that need to be considered. The results of the study are only applicable to relatives who had a family member with premature CHD who agreed to participate, and who themselves also agreed to participate.
Only hospitalized patients who survived an acute attack were included. It could be that close relatives of patients who suffer a fatal heart attack are more alerted by this event; also the family doctors may react differently in this respect.
Although there were 35 family members that refused to participate in the intervention phase of the study, the main reasons for non-participating were not due to the study process itself. The most important reasons for non-responding were that several relatives frequently visited the family doctor for a general check-up or had their risk factors screened at other occasions.
We have to be careful in interpreting the screening rates of the two groups of relatives as in I there is hard evidence that the screening took actually place, but in U the information was only obtained through self-reported questionnaires.
Conclusion
In the pre-test the screening for CHD risk factors in first degree relatives of patients with premature CHD was equally as uncommon in I as in U. During the study period a significant difference in screening rates were observed between I and U, both in the siblings and offspring of the patients with premature CHD.
The study has demonstrated that through the introduction of an information and health education program, screening of first-degree relatives of patients with premature CHD may be improved. This is the necessary condition to start an adequate risk management strategy in those people at high risk. Health education interventions, such as those used in this project, can help to close the gap between the guidelines on CHD prevention and what is realized in daily practice. A more systematic screening of these high-risk individuals will not only have a favourable effect on their life expectancy but can also yield health economic benefits for society.
Implications
The preventive screening of first-degree relatives, as recommended by international scientific expert committees, still deserves more attention. Our results should help to inform patients, families and their physicians about the familial occurrence of CHD. Healthcare providers have to be attentive to the screening for CHD risk factors of first-degree relatives of patients with premature CHD.
The results presented here demonstrate the potential for preventive cardiology in first-degree relatives of patients with premature CHD.
Footnotes
Acknowledgements
The Family Screening Project is grateful to the four hospitals in which the study was carried out: the Jan Yperman Hospital (Ieper), the Saint-Elisabeth Hospital (Zottegem), the Heilig Hart Clinic (Eeklo) and the Ghent University Hospital. We thank particularly the cardiologists and nurses of the hospitals, who gave us the opportunity to collect information needed for the project. We are also grateful to all the participants of the study: the patients and their first-degree relatives, and in particular the family doctors who screened the relatives as part of their important role in preventive medicine.