
Abstract
Background
Guidelines for the prevention of coronary artery disease (CAD) have been developed both in Europe and in the USA. However, several surveys have shown that these guidelines are poorly implemented in clinical practice.
Design/methods
The Swedish Quality Control Programme on Secondary Prevention of CAD includes patients after myocardial infarction, or having undergone coronary artery surgery or percutaneous coronary intervention. Fifty of Sweden's 79 hospital districts are currently participating. Patients are asked to send report-cards regarding risk factor management to a central registry after discharge from hospital, at a 3-6 month visit and then yearly for 5 years.
Results
Results based on data from 1 year after the index event show that a majority of patients reach targets for serum cholesterol (70%), and low-density lipoprotein (LDL)-cholesterol (71%). Mean value for total cholesterol is 4.6 (± SD 0.9) mmol/l, LDL-cholesterol 2.7 (± SD 0.8) mmol/l. Blood pressure targets are less often achieved, with 58% reaching the European Society of Cardiology target for systolic (<140 mmHg) and 81% for diastolic (<90 mmHg) blood pressure. A large proportion of patients are prescribed preventive drugs: aspirin (96%), beta-blockers (78%) and lipid-lowering drugs (83%).
Conclusions
The Swedish Quality Control Programme is one of the first attempts to assess implementation of guidelines on a national level based on patient participation. It is hoped that shared care programmes and increased patient involvement with feedback on achieved treatment goals in relation to guidelines will improve outcomes in patients with CAD.
Introduction
Guidelines for the prevention of coronary artery disease (CAD) have been developed both in Europe and in the USA [1, 2]. However, several surveys have shown that these guidelines are poorly implemented in clinical practice [3–5].
The recently published EUROASPIRE II survey showed a significant under-treatment of major risk factors for CAD [6]. The fact that half of all patients in the latter survey were not treated to target for important risk factors such as blood pressure (< 140/90 mmHg) and serum lipids, (58% had a total cholesterol > 5.0 mmol/l), shows that reaching good treatment results even in selected hospitals is difficult. In daily clinical practice among primary health care physicians the results are probably even worse, thus failing to prevent the loss of many lives and many cardiovascular events. This becomes even more important since the responsibility for long-term follow-up of patients with CAD rests in most countries with primary health care physicians who often have many other important priorities besides prevention of CAD [7–10].
In order to overcome these obstacles of adequate secondary prevention, a multitude of suggestions have been made, all aimed at increasing both adherence to guidelines and patient compliance to medication and lifestyle changes [11, 12]. Other suggestions have been to delegate more responsibility for follow-up and risk factor monitoring to specially trained nurses interested in secondary prevention [13].
The adherence to any preventive programme is probably higher if guidelines are transformed into locally developed shared care concepts, where local traditions, interests and resources are taken into consideration in the implementation process. This does not mean that the scientific basis of prevention is changed only that the practical management of the patients is locally discussed and outlined for both the hospital and primary care. The idea of local ownership of the programmes has been promoted in Sweden since the first programme on secondary prevention of atherosclerosis issued by The National Board of Health and Welfare in 1992 [14].
Today all the 79 hospital districts in Sweden have local programmes for secondary prevention of CAD. These programmes are based on the European Society of Cardiology (ESC) guidelines and have in most cases been developed jointly by hospital and primary care physicians.
To improve patient compliance, the use of patient diaries, with information about individual risk factors, have been suggested [11]. In the programme presented here, patients are given diaries, ‘heart booklets’, where intervention goals for different risk factors are noted, together with the results from actual measurements of these risk factors at discharge and subsequent follow-up visits. The main objective is to facilitate the continuous improvement of secondary prevention of CAD through individual feedback on treatment results.
The aim of this report is to present and give an overview of the 1-year results from the Swedish National Programme for Quality Control on Secondary Prevention of CAD. It reflects how well we manage patients with CAD in clinical practice, both in hospitals and primary care, as reported by the patients themselves.
Methods
The programme for quality control of locally developed guidelines for secondary prevention of CAD was launched on 1 January 1998, jointly by The Swedish Society of Cardiology, the Swedish Association of Family Physicians and VIC (Nurses in Cardiology). The programme has been supported both by The National Board for Health and Welfare and The Swedish Heart and Lung Foundation. Each of the 50 participating districts have appointed two contact persons who are responsible for the programme locally, one from the hospital and one from the primary health care.
Patients with a diagnosis of acute myocardial infarction (AMI), coronary artery bypass grafting (CABG) or percutaneous transluminal coronary angioplasty (PTCA) are invited to participate in the programme. At discharge from hospital, eligible patients who consent to participate are provided with a diary, ‘Heart booklet’, where data on risk factors such as smoking, blood pressure, serum lipid levels, blood glucose levels, glycosylated haemoglobin and current medication, together with risk factor intervention targets are noted. The diary also contains seven report cards where the above information is entered (Fig. 1). The first card is to be filled in at the time of hospital discharge. The subsequent six cards, which are all identical, are to be completed at outpatient clinics after 3-6 months and subsequently yearly for 5 years after the index event. The cards are posted by the patient with prepaid postage to the central registry in Malmö where the information is computerized. The database also contains information on the targets for intervention detailed in the secondary prevention programmes of all participating districts.
The intervention offered to the patients is in every case the preventive programme of each participating district. (A district consists of one or more hospitals and the surrounding primary care physicians.) The programme can vary slightly from district to district depending on local traditions but is generally based on one or two visits to the hospital's outpatient clinic followed by referral to the primary health care for subsequent follow-up. Guidelines for risk factor intervention are decided locally and may vary between districts. However, as these guidelines are based on national and ESC guidelines the main target levels for intervention are in accordance with ESC recommendations [1]. This includes cessation of smoking, goals for total cholesterol < 5.0 mmol/l, low-density lipoprotein (LDL)-cholesterol < 3.0 mmol/l and blood pressure < 140/90 mmHg.
An annual report displaying the average results of risk factor intervention and medication compared with the goals set up in the local programme is sent to the contact persons in each district. For the purpose of benchmarking, national averages and treatment to targets in relation to the ESC guidelines [1] are also presented and the districts are independently informed about their performance. Further information is available in English on the project's website (www.hjartkvalitet.nu).
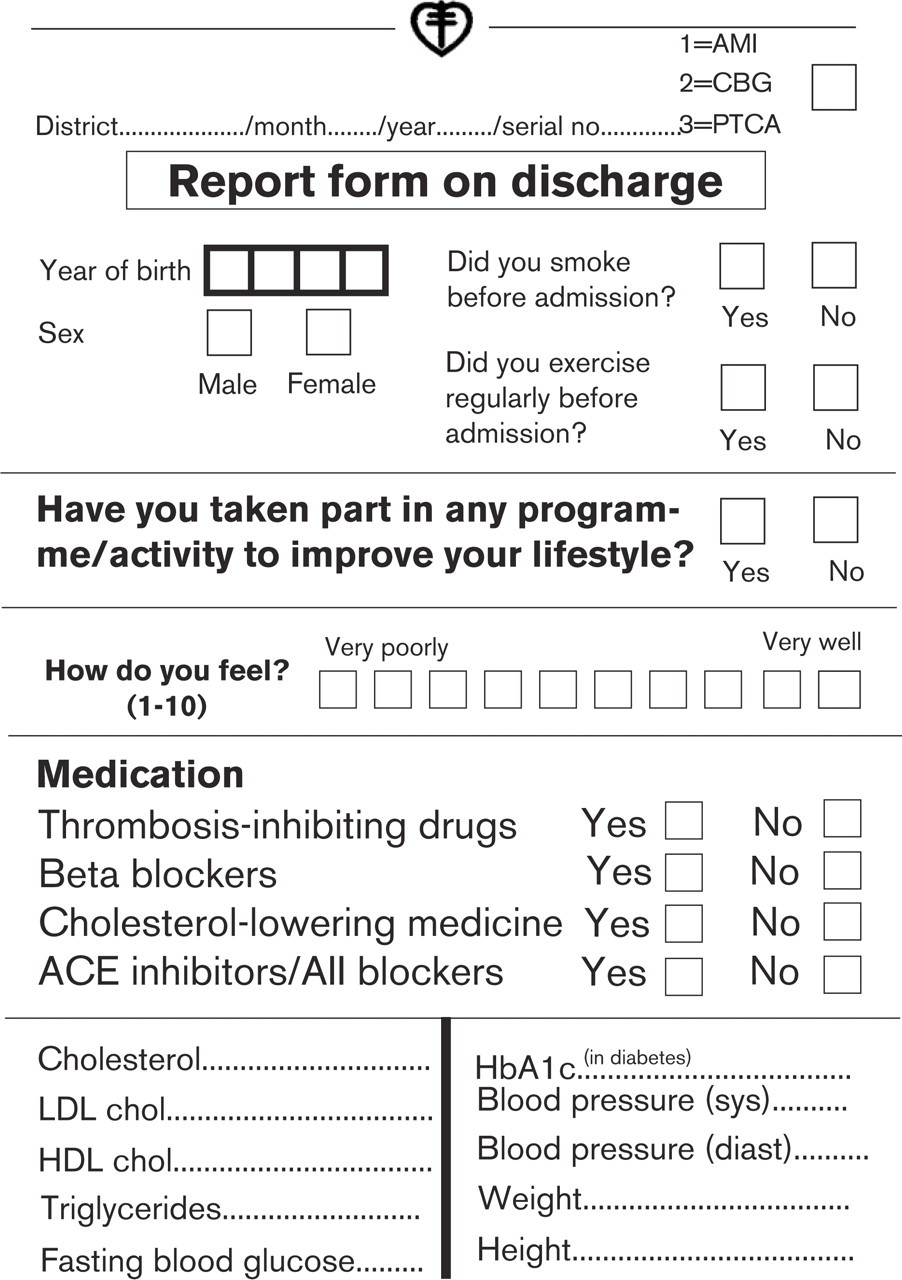
Report form on discharge from the Swedish Quality Control Programme.
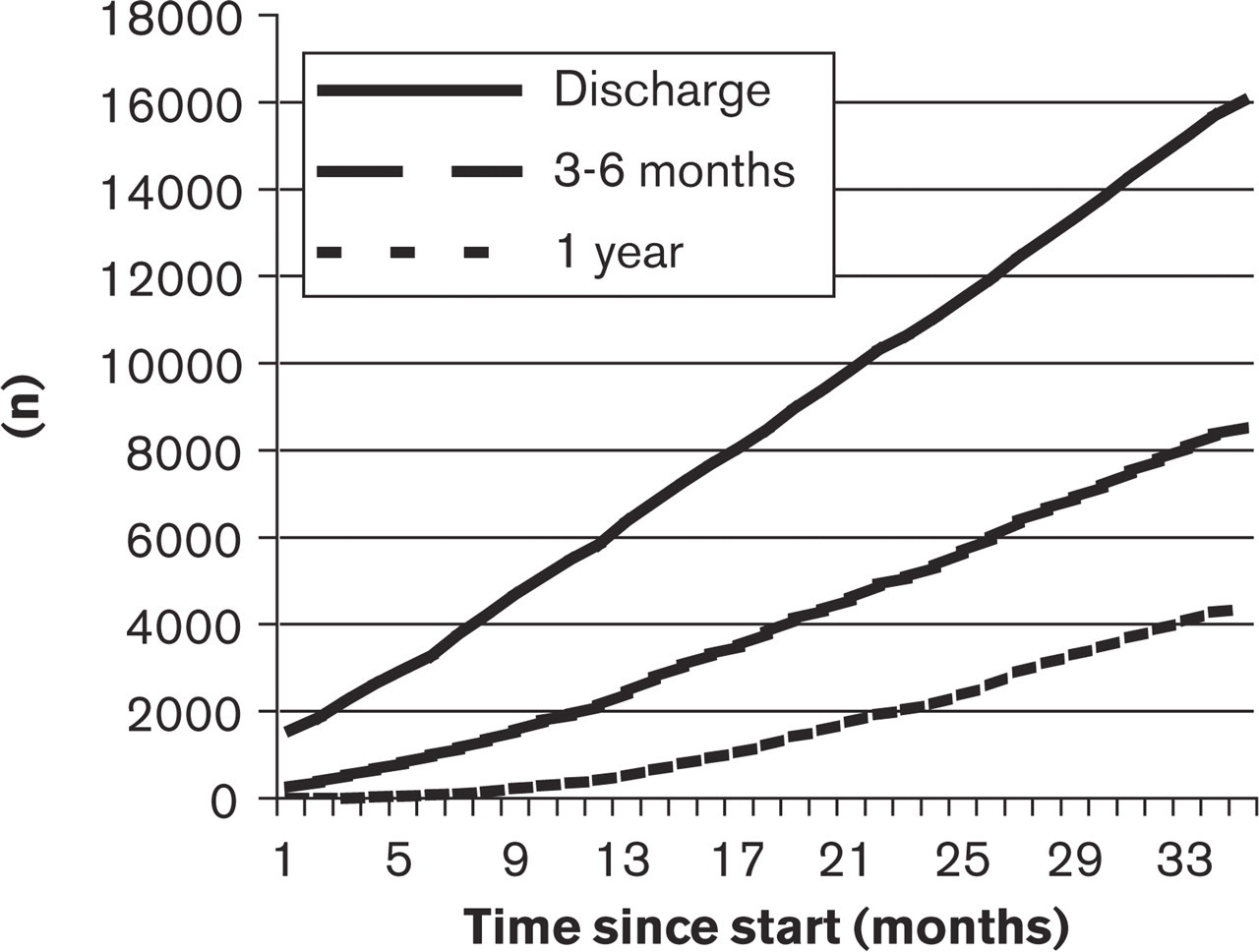
Accumulated number of received reports in the Swedish Quality Control Programme.
Results
As of 31 July 2001, a total of 30 767 report cards have been sent to the registry. There has been a steady increase in the number of reports received over time as shown in Figure 2.
The overall response rate by 28 February 2001, was 59% for the 3-6 month report and 39% for the 1-year report. This represents a significant increase in response rate compared with May 2000 when the 3-6 months and 1-year response rates were 53 and 19% respectively.
Table 1 shows the average national results for risk factor management at discharge, after 3-6 months and 1 year after the index event. A majority of the patients had serum cholesterol, serum LDL-cholesterol and blood glucose levels below the goals of the ESC guidelines after 3-6 months and 1 year, whereas the goal for systolic blood pressure was less often achieved (Fig. 3). As shown in Figure 4, treatment to goal of risk factors for CAD varied significantly between different districts at 1 year. Seventy percent of the patients reached the ESC goal of < 5.0 mmol/l and 71% reached the goal for LDL-cholesterol of < 3.0 mmol/l. Substantially fewer patients (58%) reached the target systolic blood pressure of < 140 mmHg, whereas 81% reached the target for diastolic blood pressure of < 90 mmHg. The percentage of patients reaching ESC goals for serum LDL-cholesterol varied from 42 to 79% at 3-6 months, and 35 to 90% at 1 year after the index event between districts. The same was seen for systolic blood pressure where reaching ESC targets varied from 29 to 98% at 3-6 months and 47 to 93% at 1 year. The frequency of smoking varied between 4 and 26% at 1 year in the different districts.
Risk factors at discharge and at follow-up in coronary artery disease (CAD) patients (mean ± SD)
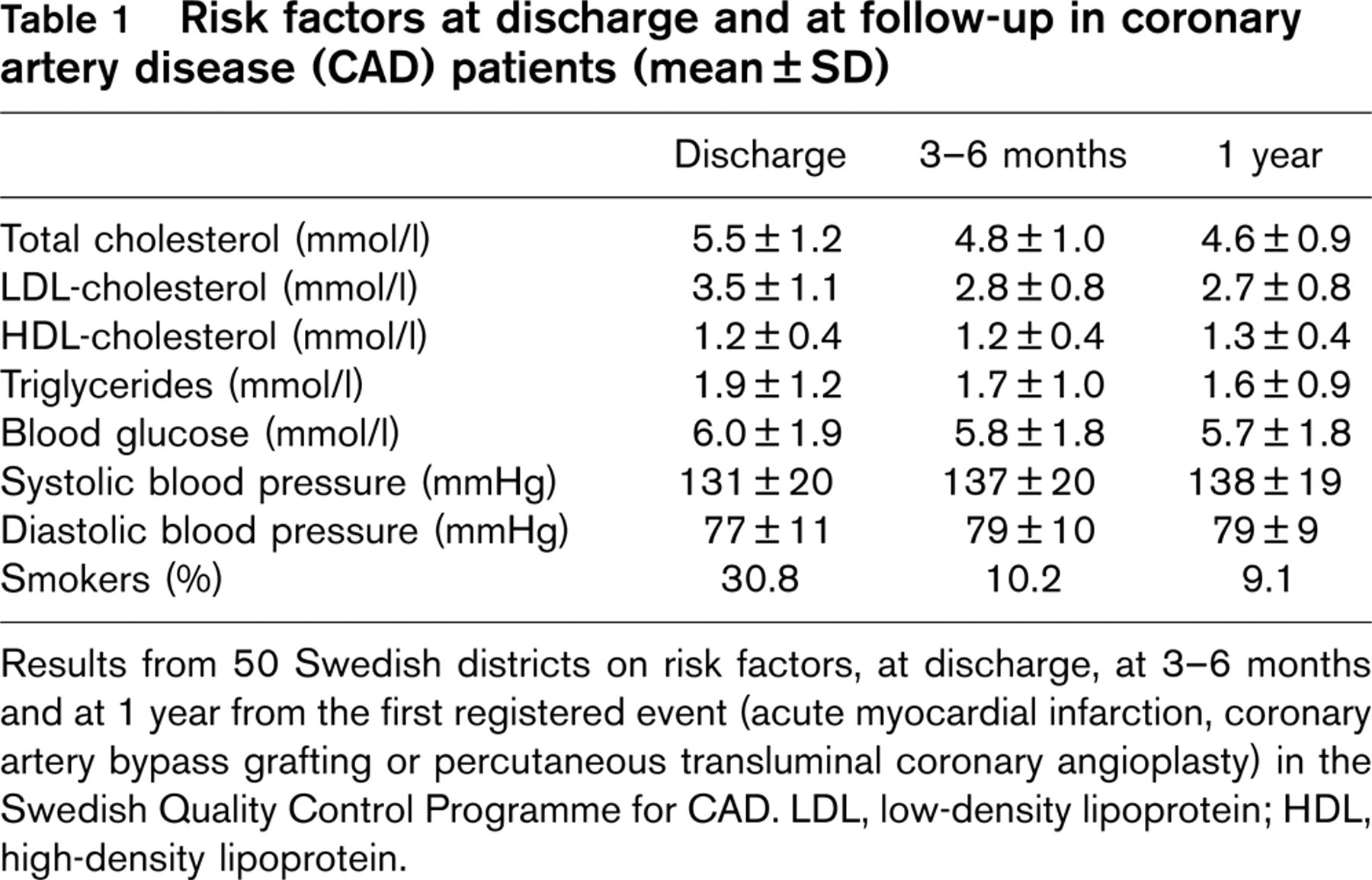
Results from 50 Swedish districts on risk factors, at discharge, at 3-6 months and at 1 year from the first registered event (acute myocardial infarction, coronary artery bypass grafting or percutaneous transluminal coronary angioplasty) in the Swedish Quality Control Programme for CAD. LDL, low-density lipoprotein; HDL, high-density lipoprotein.
The adherence to ESC guidelines concerning pharmacological treatment of CAD was good, with a large majority of patients receiving platelet inhibitors/warfarin, betareceptor blockers and lipid-lowering drugs (Table 2). There were, however, substantial variations in the prescription pattern between different districts as is seen in Figure 4.
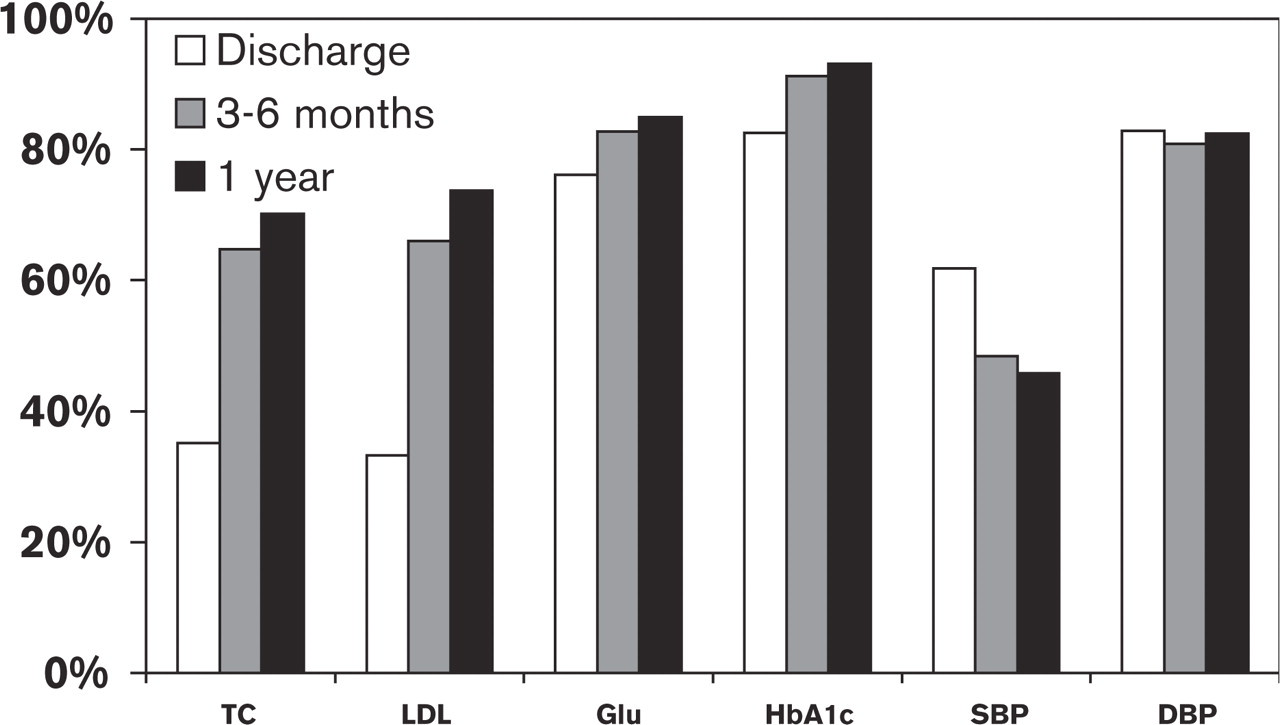
Patient adherence to European Society of Cardiology guidelines for risk factors for coronary artery disease: TC = total cholesterol (<5.0 mmol/l), LDL = low-density lipoprotein-cholesterol (<3.0 mmol/l), Glu = blood glucose (<6.5 mmol/l), HbA1c = glycosylated haemoglobin (<7.5 mmol/l), SBP = systolic blood pressure (<140 mmHg), and DBP = diastolic blood pressure (<90 mmHg).
Drug utilization (%) in patients with coronary artery disease (CAD) at discharge and follow-up
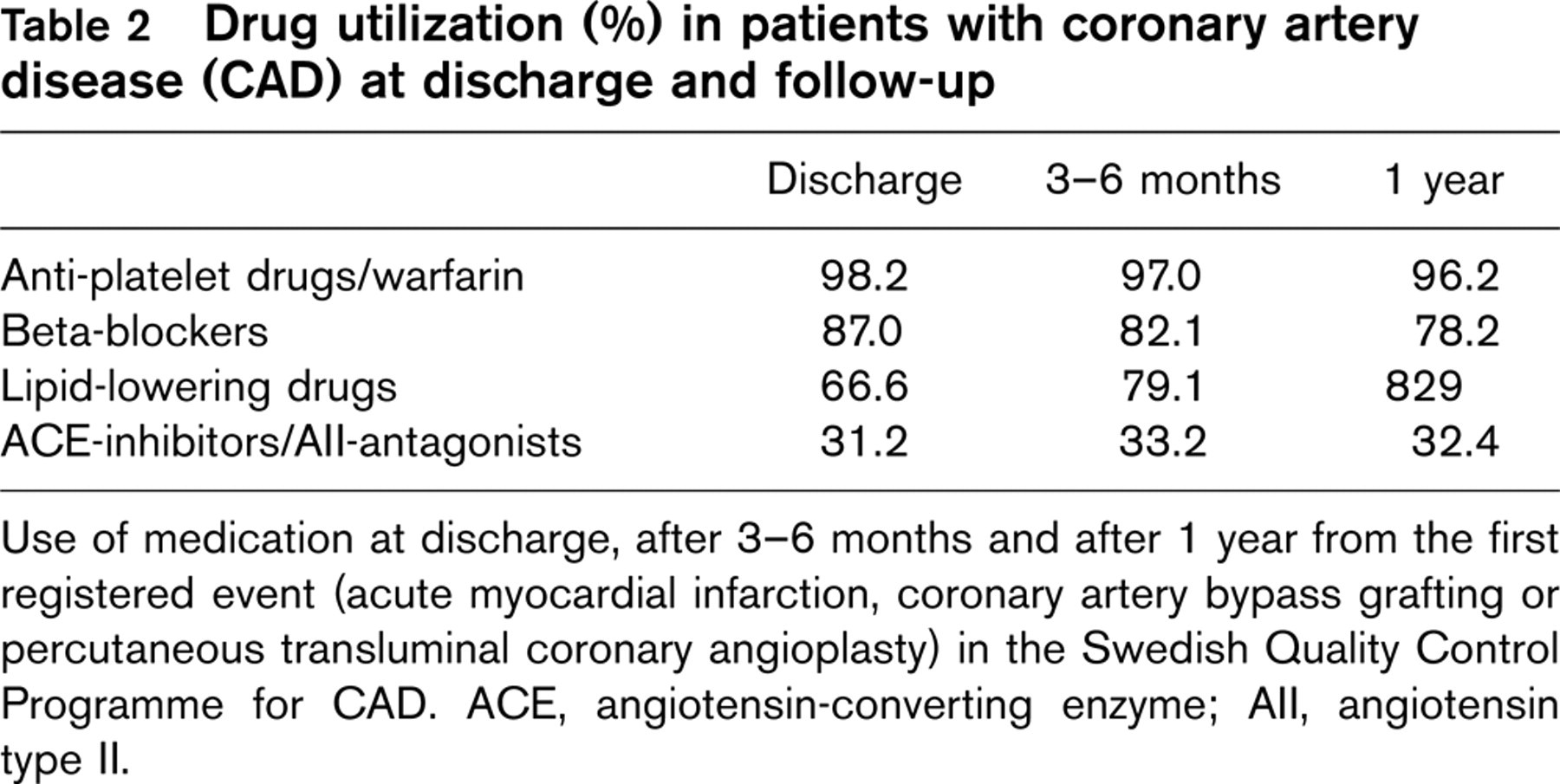
Use of medication at discharge, after 3-6 months and after 1 year from the first registered event (acute myocardial infarction, coronary artery bypass grafting or percutaneous transluminal coronary angioplasty) in the Swedish Quality Control Programme for CAD. ACE, angiotensin-converting enzyme; All, angiotensin type II.
The response rate varied markedly between different districts. In order to assess why report cards were not sent in, a survey was performed in three districts. Questionnaires were sent to 441 patients who had participated in the programme for at least 3 months. The response rate was 89%. The results generally showed that patients, both in principle and on an individual basis, considered the diary to be a very valuable instrument for monitoring risk factors. Since sending in the report cards was voluntary a few patients probably declined to do so. However, the major reason not to send in report cards was that physicians and other health workers had not reminded patients to do so. A similar survey performed among physicians at participating hospitals and primary health care centres showed that the vast majority of staff are very positive to the idea and perceive the project to be an important way to improve the quality of secondary prevention. In an attempt to validate the data from the registry, a pilot study was performed in one district. In this district, a total of 152 patients were entered into the programme in 1999. Of these, 82 (57%) sent in their 1-year report card. Information about 1-year risk factor levels and medication for the dropouts was actively sought in hospital and primary care databases and records. Of these, no data was found for seven patients (5%). As is shown in Table 3 there was remarkable similarities in risk factor levels and medication between responders and dropouts indicating a good validity for data, at least at a response rate of 57%.
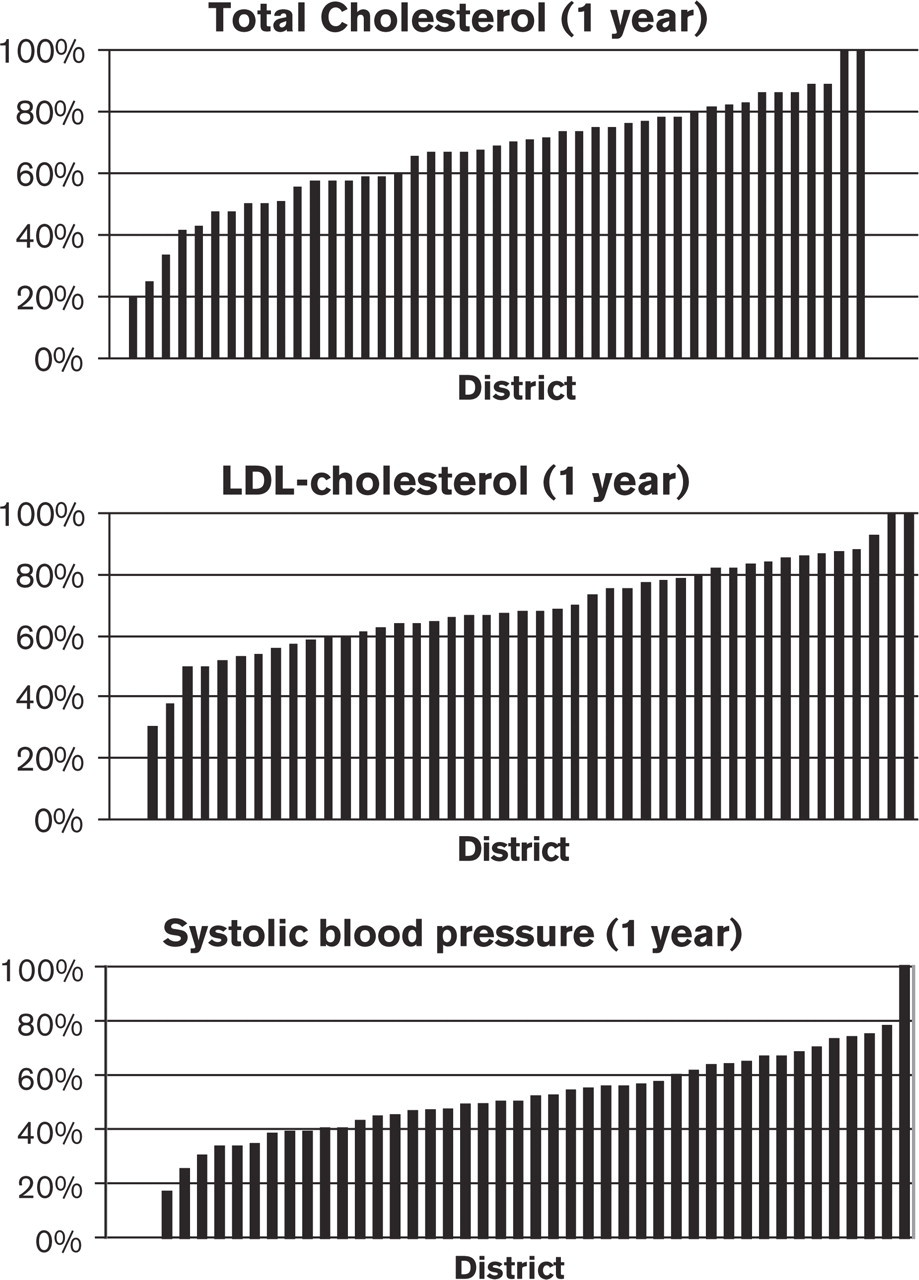
Variations between participating districts/geographical areas in reaching recommendations for various risk factors after 1 year (%). LDL, low-density lipoprotein.
Discussion
The Swedish model for implementation of programmes to improve secondary prevention of CAD is based on local shared care programmes together with an increased patient involvement. The idea is to create a continuum of care from in-hospital stay via outpatient clinics to long-term follow-up in the primary health care. The transfer of information between health care providers regarding risk factors and treatment goals is in this context very important. Patients are encouraged to take a greater responsibility for their own health, and are offered education about both CAD and risk factor management, all in an effort to increase compliance. This has been a deliberate policy by The Swedish Board for Health and Welfare in order to support the idea of long-term responsibility for the patients. These ideas have led to the development of local secondary prevention programmes for CAD in all the 79 health districts in Sweden. The local programmes are based on national and European guidelines and have in most cases been developed by primary and hospital care physicians working together. This has created a sense of ‘ownership’ within each local initiative. However, no information has hitherto existed on how well the different districts have succeeded in adhering to the guidelines and how well patients will reach various targets for intervention in clinical practice.
Comparison between participants and dropouts
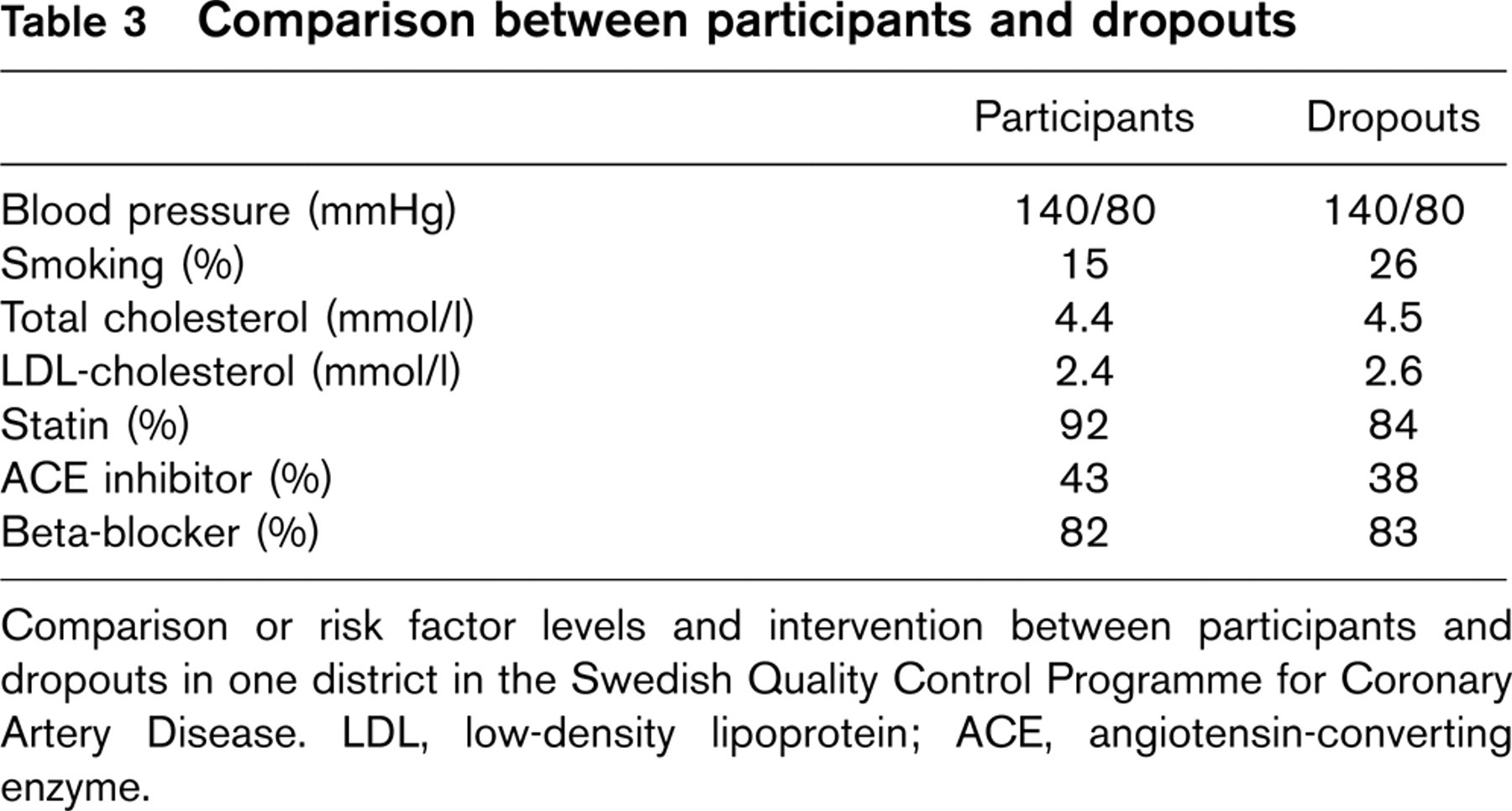
Comparison or risk factor levels and intervention between participants and dropouts in one district in the Swedish Quality Control Programme for Coronary Artery Disease. LDL, low-density lipoprotein; ACE, angiotensin-converting enzyme.
Through The Swedish Quality Control Programme on CAD, benchmarking of secondary prevention programmes has now become possible. The register's owners and the supporting authorities (The Swedish Board for Health and Welfare and The Swedish Heart and Lung Foundation) consider it to be an important tool for long-term improvement of secondary prevention of CAD for several reasons. For one thing, the knowledge of the quality of care in each district may stimulate the physicians to comply with the guidelines they have adopted. It is also a tool for empowering patients to take a greater responsibility for their own health by education and feedback on treatment. Furthermore, the information from the quality control register becomes official annually and enables health authorities to monitor health productivity both quantitatively and qualitatively regarding the management of patients with CAD. An online version of the report has recently become available on the Internet (www.hjartkvalitet.com). The results presented in this paper show that although treatment results and adherence to guidelines are generally well met in Sweden, there are substantial differences between different health care districts and geographical areas in Sweden. These differences cannot be sufficiently explained by regional differences in disease/risk factor panorama, or lack of knowledge among physicians and other health care providers. It is more likely that the differences reflect varying personal interests and focusing among opinion leaders in cardiology in the different districts/geographical areas. A recent study from Finland supports the view that a large number of GPs do not adequately adhere to guidelines due to lack of personal motivation [15]. It is probable that this reflects the many medical tasks faced by GPs in combination with structural problems within the primary health care sector such as under-funding, and shortage of doctors in certain areas. The geographic differences may also reflect lack of support from local health care authorities in secondary prevention of CAD. Although there are geographical differences in treatment, this does not seem to be true for gender. Indeed, a recent study from the registry suggests that lipid control and access to drugs is relatively gender-equal [16].
We are currently undertaking a study to analyse the structure and process of secondary prevention in each participating district and relate that to how well risk factor and intervention targets are met. We are also planning a study to ascertain how well (or badly) dropouts are doing in the same respect. By using the registry in this way we hope to obtain information on how a successful secondary prevention programme should be designed to obtain maximum effect.
The guidelines in different European countries regarding secondary prevention of CAD are very similar and no major discussion or controversy has been noticed since the last publication of The European Guidelines on Secondary Prevention of CAD in 1998 [1]. However, substantial differences were shown between countries when the results from the EUROASPIRE II study was published [6]. The differences among the 15 European countries cannot be attributed to different views on the scientific grounds for the common European guidelines. A number of factors that influence care can be identified: The organization and financing of health care varies markedly over Europe. In some countries such as the United Kingdom and the Scandinavian countries the long-term follow-up of patients with CAD is the responsibility of the primary health care. In other countries this task lies mainly with hospital specialists in outpatient clinics. Reimbursements for medicine costs vary significantly across Europe and can of course directly affect the willingness of patients to accept medication. There is also, especially among cardiologists, a focus on the acute phase of CAD rather than preventive measures. Although acute coronary interventions such as invasive treatment of CAD is important to reduce mortality on a short-term basis, one must not forget that the long-term treatment of coronary risk factors is very important in reducing mortality and morbidity.
The solution to the problem is not to produce more and more guidelines. Doctors must also be persuaded, as well as given the opportunity, to apply existing guidelines in everyday clinical practice. The first step can be to adopt joint quality assurance systems in order to enable comparisons of results both between regions, and to compare results in the same region over time. Education and motivation of patients regarding both the nature of coronary disease and the action and importance of medication and lifestyle changes need to be improved.
Independently of which methods for improving secondary prevention in CAD we adopt, continuous monitoring of how well we are doing must be considered mandatory. At the end of the day, it is not possible to suggest improvements for the future if we don't know what we are doing today! We propose that the Swedish Quality Control Programme is a useful tool which involves all parts of the health care system, including the patients themselves, in the continuous improvement of secondary prevention in CAD.
Limitations of the study
Several considerations have to be made when interpreting the results. No registry based on the concept of voluntary participation can be expected to produce an altogether representative picture. It could be argued that it is probably the patients who are most deeply committed to adhering to treatment programmes and complying with medication who have sent in their report cards and that therefore there is a selection bias of relatively healthier participants. This may well be true and consequently our results show possible ‘best practice’ in the participating districts. Even so, there is much room for improvement and the differences between districts are important to identify. Only by knowing the performance can we influence doctors and patients to do a better job in secondary prevention. However, a pilot study performed in one district shows remarkably good comparability between responders and non-responders, at least at a response rate of about 60%.
It is also possible that the hospital regions that have decided to participate are those where secondary prevention is considered a priority. Again, our data may be too positive with respect to actual management. It should also be underlined that we are unable to find out why report cards are missing. Some patients will die and others will for various reasons fail to remember or refuse to send the cards. Since the objective of our programme is to improve the management of patients with CAD and to compare how different districts reach targets in every day clinical practice, our view is that, despite their limitations, the results are of great relevance to the overall question of how we implement guidelines.
The lack of a control group makes it impossible to assess the impact of the programme itself. However, compared with historical data and the EUROASPIRE II data our findings indicate that we have succeeded to bring more patients to target particularly regarding lipid management and the use of drugs for prevention.
Conclusions
The Swedish Quality Control Programme on CAD is one of the first attempts to assess the implementation of secondary prevention guidelines on a national level. Our data support the view that the clinical practice of secondary prevention of CAD still needs to be improved and that patients are treated differently in various parts of Sweden.
Whether the programme itself improves management is not clear but compared with other surveys the management is better with respect to lipid management and prescription of drugs for prevention. Limitations of our study due to missing report cards are clear and the data may give a better picture than the reality. Regardless, the programme shows one important way to implement guidelines much needed in clinical practice.
Footnotes
Acknowledgements
This work is supported and funded by the National Board of Health and Welfare, the Swedish Heart and Lung foundation and the Swedish Societies for Cardiology and Family Medicine.
We thank the staff of the registry, Anne-Marie Nilsson and Eva Holmström, and all participating districts.