
Abstract
Background Plasma fibrinogen may be an independent risk factor for cardiovascular disease. Cigarette smoking is a well-recognized determinant of plasma fibrinogen however it remains unclear how fibrinogen levels relate to the degree and duration of smoking, or to time since smoking cessation.
Methods In a population-based study of 11 059 men and women aged 45–74 years, we examined the cross-sectional relationship between plasma fibrinogen and cigarette smoking habit.
Results Mean fibrinogen concentrations were higher in current smokers compared to non-current smokers (men: 3.13±0.77 versus 2.80±0.71 g/l, P<0.0001; women: 3.03±0.72 versus 2.95±0.71 g/l, P=0.01), independent of age, body mass index and hormone replacement therapy in women In men, fibrinogen concentrations declined with years since stopping smoking but remained higher than in life-long non-smokers for 15 years. No relationship between fibrinogen and duration of smoking cessation was observed in women. On multivariate analysis, age, body mass index, use of hormone-replacement therapy, smoking status and pack-years of smoking were independent predictors of plasma fibrinogen.
Conclusions Plasma fibrinogen is strongly associated with cigarette smoking with a dose–response relationship with total pack-years of smoking. In men who stop smoking plasma fibrinogen may remain elevated for several years after cessation. Eur J Cardiovasc Prev Rehabil 12: 144–150 © 2005 The European Society of Cardiology
Introduction
Plasma fibrinogen has been reported to be an independent risk factor for ischaemic heart disease and stroke in several prospective studies [1–3]. However the role of fibrinogen in the causal pathway of these disease processes remains unclear. Fibrinogen is itself associated with most of the established vascular risk factors [4–8], and elevated plasma levels in those who develop coronary heart disease (CHD) and stroke may reflect an adverse risk factor profile or be a marker of chronic inflammation secondary to sub-clinical atherosclerosis.
Previous population-based cross-sectional studies have identified age, female gender, current cigarette smoking, obesity and use of female hormone replacement therapy as important determinants of the plasma fibrinogen level in healthy persons [9]. Of these, current cigarette smoking appears to be the strongest modifiable determinant, with mean levels in smokers being consistently 0.3–0.5 g/l higher than in life-long non-smokers [9]. Though some studies have suggested that plasma fibrinogen levels are related to the degree of smoking measured either by cigarettes smoked per day [4, 10, 11] or total pack-years of exposure [12] there appear to be some differences between men and women [6, 12]. It is also unclear how long it takes for plasma fibrinogen levels to fall after cessation of smoking. Previous cross-sectional studies have estimated that plasma fibrinogen levels in former smokers remain elevated compared to life-long non-smokers for 5–14 years since stopping smoking [5, 13–16] while prospective smoking cessation studies have observed a fall in plasma fibrinogen to a level comparable with non-smokers within 8 weeks [17, 18]. These conflicting results may be explained by differences in the effects of smoking in men and women and between older and younger age groups.
We investigated the relationship between plasma fibrinogen and cigarette smoking in a large population-based cohort of men and women.
Methods
Study population
Study participants came from a general population-based cohort of approximately 25 000 men and women aged 45–74 participating in the Norfolk arm of the multi-centre European Prospective Investigation into Cancer (EPIC). Methods of recruitment and measurement in EPIC have been described elsewhere [19] and are summarized briefly below.
Between 1993 and 1997, all individuals aged 45–74 years registered with 35 participating general practices in the Norfolk area were invited to participate by post. Participants completed a health and lifestyle questionnaire (HLQ), and attended a health check where anthropometric variables and blood pressure were measured.
Survey methods
The EPIC ‘health and lifestyle questionnaire’ included questions on age, smoking, alcohol, occupation, previous medical history and physical activity. ‘Current smokers’ were defined as those who answered ‘yes’ to the question ‘Do you smoke cigarettes now'. ‘Never smokers’ were defined as those who answered ‘no’ to the question ‘Have you ever smoked as much as one cigarette a day for as long as a year'. All others were classed as ‘former smokers'. The number of cigarettes smoked each day at recruitment and at ages 20, 30, 40 and 50 years were recorded and the cumulative cigarette consumption in pack-years was derived from these data. One pack-year was defined as 20 cigarettes a day for 1 year. For former smokers information was also collected on age at stopping smoking, from which the number of years since smoking cessation was calculated.
Prevalent disease was measured by the question ‘Has your doctor ever told you that you havey', followed by a list of options including: angina, heart attack, stroke, cancer. Prevalent cancer was also determined by searching the East Anglia Cancer Registry and by linkage with the Office of National Statistics database. Recorded cancer at any site, including skin, was included. Use of medication was assessed by asking participants to name ‘any drugs or medicines, taken in the last week, either prescribed by your doctor or bought from the chemist'. Women were additionally asked ‘Have you ever received any hormone replacement therapy’ and ‘Are you currently taking this treatment'.
Anthropometric measurements were performed according to a standard protocol. Height was measured to the nearest millimetre, without shoes. Weight was measured to the nearest 0.2 kg without socks and shoes in light clothing. Body mass index (BMI) was derived as weight in kilograms/(height in metres)2.
Laboratory methods
Blood (42 ml) was collected in the non-fasting state. Samples later used for fibrinogen analysis were collected in citrated bottles, stored in a refrigerator at 4°C overnight and transferred the following morning to the EPIC laboratory for processing. Plasma not required for immediate analysis was frozen in aliquots in liquid nitrogen at −196°C. Between 2000 and 2002 aliquots of plasma were retrieved from liquid nitrogen and thawed for fibrinogen analysis. Fibrinogen was measured by a functional assay based on the method of Clauss [20] using the commercial kit Fibriquik (bioMerieux, Lyon, France) on an MDA180 automated analyser (bioMerieux).
Statistical methods
Statistical analyses were performed using STATA version 7 (Stata Corporation, College Station, Texas, USA). All analyses were performed for men and women separately. A value of P < 0.05 was used to define statistical significance and all tests were two-tailed.
Mean plasma fibrinogen was calculated by 10 year age-group, by body mass index category using clinically recognised cut-points and by postmenopausal hormone replacement therapy (HRT) use in women. Mean fibrinogen adjusted for age, BMI and current HRT use in women was calculated for current, former and non-smokers. Current and former smokers were then separately divided into four groups according to their total pack-years of smoking and mean fibrinogen adjusted for age, BMI and percentage of current HRT users was calculated for each group. For former smokers, years since stopping smoking were categorized into four groups and adjusted mean fibrinogen calculated for each group. Adjustment for age, BMI and percentage of current HRT users was performed using analysis of covariance. Differences in adjusted mean fibrinogen across strata were tested with F tests. Finally multiple linear regression was performed. Predictors of plasma fibrinogen were modelled separately for all men and all women, male and female current and former smokers and male and female former smokers only. All likely measured predictors of plasma fibrinogen were entered into these models, including age, BMI, current smoking status, total pack-years of smoking, current or former HRT use for women and length of time since stopping in former smokers.
In the current analyses, plasma fibrinogen measurements were available on 13 029 individuals aged 45–74 years from the cohort. Twenty-three individuals with fibrinogen measurements higher than four standard deviations from the mean were excluded from the analysis as these extreme outliers probably represented an acute phase response due to intercurrent illness. We also excluded participants with medical conditions at baseline that may be associated with changes in plasma fibrinogen levels including self-reported history of heart attack (394 persons), stroke (136 persons) or cancer at any site (929 persons). Those reporting taking corticosteroids at baseline (367 persons) were also excluded from the analysis. After exclusion of a further 121 individuals with missing data on sex, BMI or smoking history, the final study population comprised 11 059 individuals.
Results
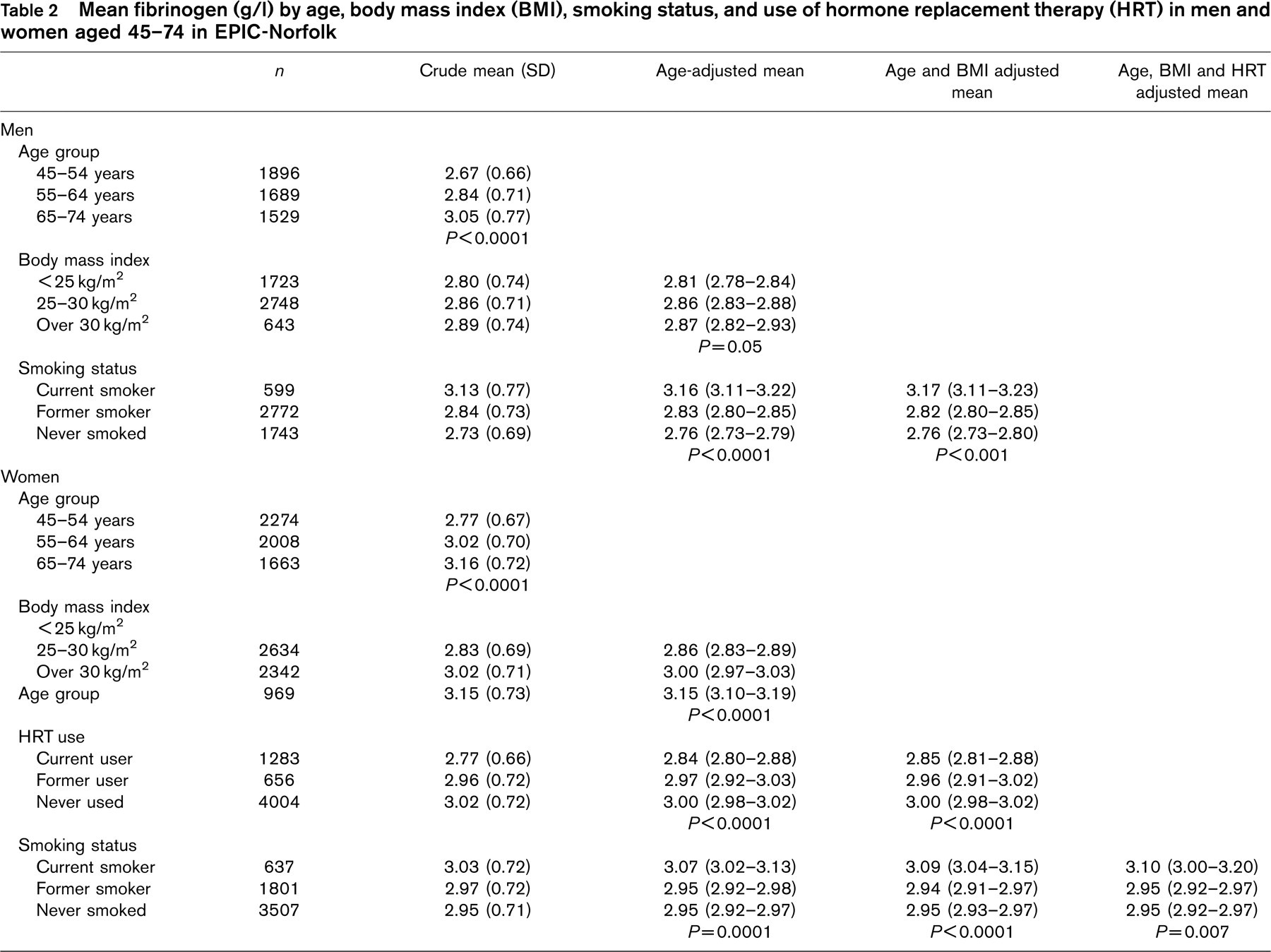
Descriptive characteristics of the study population are shown in Table 1. Mean fibrinogen was 0.12 g/l higher in women than in men and increased with age in both sexes (Table 2), rising by 0.02 g/l [95% confidence interval (CI), 0.018–0.022] per year in both men and women. Mean fibrinogen increased with increasing BMI in both sexes particularly in women, and was lower in women using HRT than in women not currently using this therapy.
Age and BMI-adjusted mean fibrinogen was significantly higher in current smokers than in former or never smokers in men and in women regardless of HRT use. The difference in adjusted mean fibrinogen between former and never smokers was of borderline significance in men and non-significant in women.
Adjusted mean fibrinogen was significantly higher in female current smokers and male current and former smokers with over 30 pack-years of cigarette smoking exposure than in those with a less than 10 pack-year smoking history (Table 3). However no relationship between mean fibrinogen and cumulative smoking exposure was observed in female former smokers, even after adjustment for HRT use.
Descriptive characteristics of men and women in EPIC-Norfolk
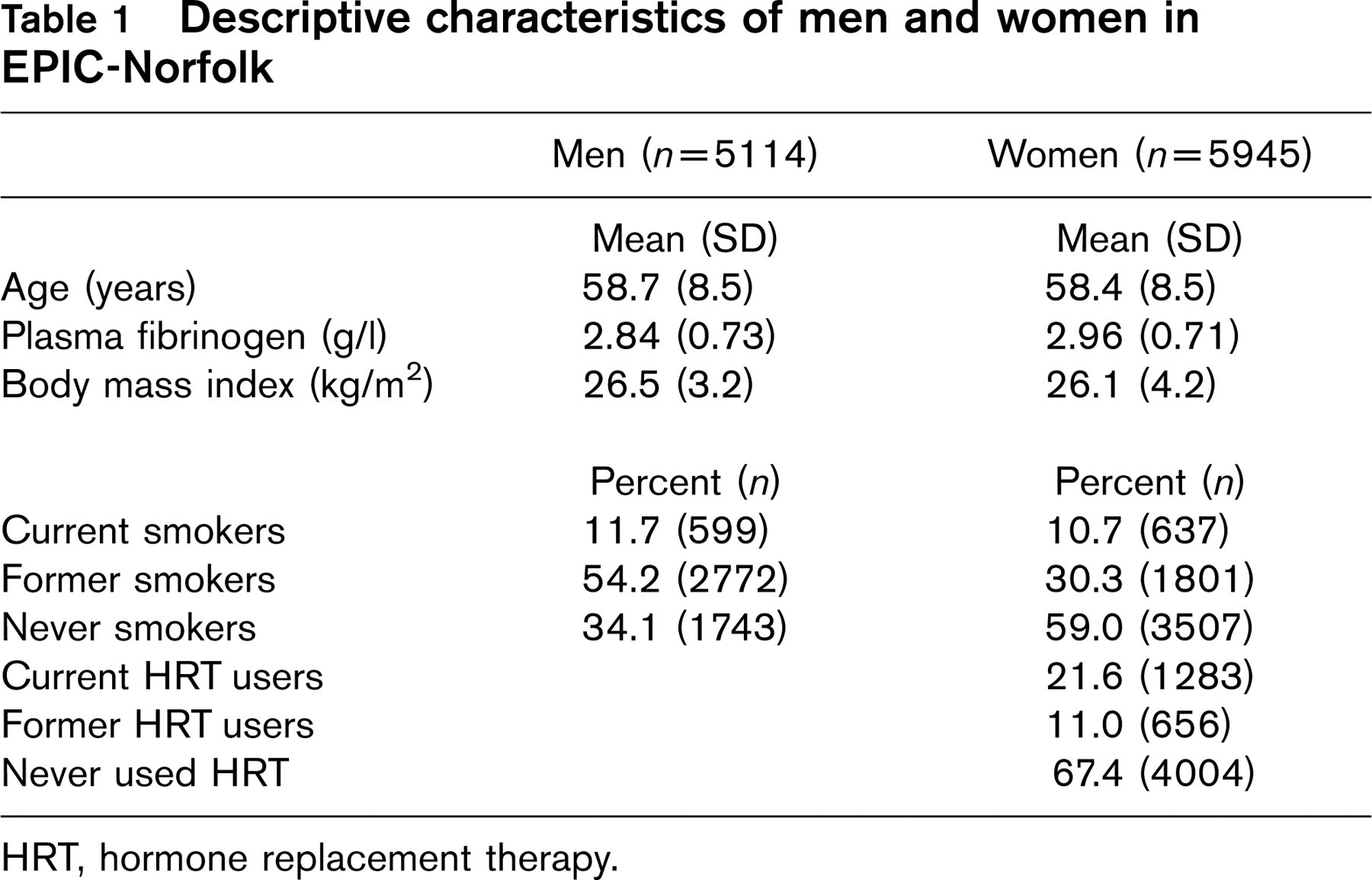
HRT, hormone replacement therapy.
Amongst male former smokers, mean plasma fibrinogen fell with years since smoking cessation (Table 4) and remained higher than the age and BMI-adjusted mean in male never smokers (2.76; 95% CI, 2.73–2.80) for up to 15 years. No relationship between mean fibrinogen and duration of smoking cessation was observed in female former smokers, and the adjusted mean fibrinogen level in women who had stopped smoking within the previous 5 years was not significantly different to that in women who had never smoked (2.95; 95% CI, 2.93–2.97).
On multivariate analysis, age, BMI, current smoking (compared to life-long non-smokers) and total pack-years of smoking emerged as significant predictors of plasma fibrinogen in both men and women (Table 5). In addition, current HRT use was a significant predictor of plasma fibrinogen in women. Restricting the analysis to former smokers did not reveal any relationship between length of time since stopping smoking and plasma fibrinogen in either men or women. Total pack-years of smoking was a significant predictor of plasma fibrinogen in men regardless of smoking status, however it was not a predictor of fibrinogen in female former smokers.
Discussion
In this population-based cohort of middle-aged and older men and women, we confirmed the major determinants of plasma fibrinogen level identified in previous cross-sectional studies. Differences in mean fibrinogen between men and women and with increasing age were of similar magnitude to those previously found [4–6, 10, 11], while BMI and HRT use were confirmed as important determinants of plasma fibrinogen in women.
Our results suggest that current smoking habit and cumulative exposure to cigarette smoking are both strong determinants of plasma fibrinogen in men and women. Current cigarette smokers had mean fibrinogen levels 0.15–0.40 g/l higher than life-long non-smokers, however in contrast to other work [4, 13], we did not observe a significant difference in fibrinogen levels between former smokers and non-smokers. This may be due to the heterogeneity of the ‘former smokers’ group. Our finding that adjusted mean fibrinogen was related to total pack-years of smoking in male and female current smokers is at odds with a recent European study which observed a dose–response relationship between fibrinogen and pack-years of smoking only in men [12]. However, that study was smaller than ours, did not exclude individuals with prevalent disease, and did not adjust for HRT use.
Mean fibrinogen (g/l) by age, body mass index (BMI), smoking status, and use of hormone replacement therapy (HRT) in men and women aged 45–74 in EPIC-Norfolk
In common with other cross-sectional studies our results suggest that plasma fibrinogen levels in men remain elevated for several years after smoking cessation. Cross-sectional studies in middle-aged men have previously noted elevated plasma fibrinogen levels in former smokers compared to life-long non-smokers for at least 10 years since stopping smoking [5, 13]. Longitudinal studies, however, have not consistently observed a fall in fibrinogen in male quitters [16, 21] while small, short-term studies of smoking cessation in younger men have observed a fall in plasma fibrinogen to a level comparable with non-smokers within 8 weeks [17, 22]. This suggests that smoking exerts both acute and chronic effects on the plasma fibrinogen level and that smoking cessation may be followed by rapid initial decline in fibrinogen followed by a more gradual fall to levels seen in non-smokers. Unfortunately low numbers did not allow reliable estimates of mean fibrinogen levels in individuals who had stopped smoking within the previous year.
There are few studies of the effect of smoking cessation on fibrinogen levels in women. Our finding of a lack of relationship between fibrinogen and duration of abstinence in women are in accord with another recently published European study [12]. The lack of a significant relationship in female former smokers in EPIC could be explained by the lower numbers of former smokers and lower range of smoking exposure in women compared to men.
The limitations of this study include the cross-sectional design and the use of a cohort who might be expected to be healthier than the general population as they were responders willing to participate in a long-term study. Comparison of the EPIC cohort with a national sample in the Health Survey of England shows that two cohorts are similar in terms of anthropometric variables and blood pressure but that current smokers are under-represented in the EPIC cohort. However this is one of the largest population-based cohorts to be studied with respect to fibrinogen with good representation of previously understudied groups such as women and those over 65 years.
Mean fibrinogen (g/l) (95% confidence interval) by total pack-years of smoking in current and former smokers in men and women aged 45–74 years in EPIC-Norfolk
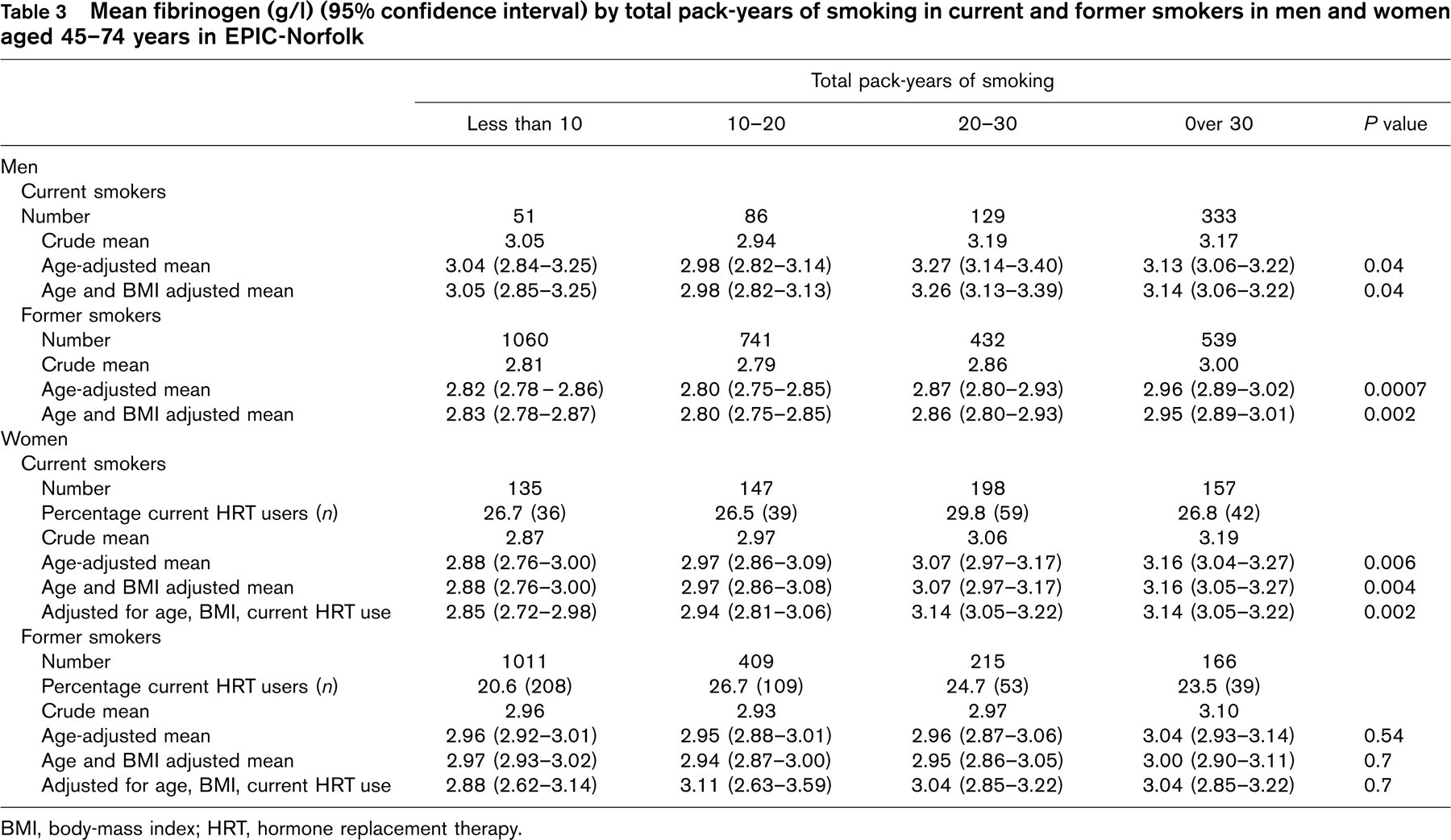
BMI, body-mass index; HRT, hormone replacement therapy.
Mean fibrinogen (g/l) (95% confidence interval) by years since stopping smoking in former smokers in men and women aged 45–74 years in EPIC-Norfolk
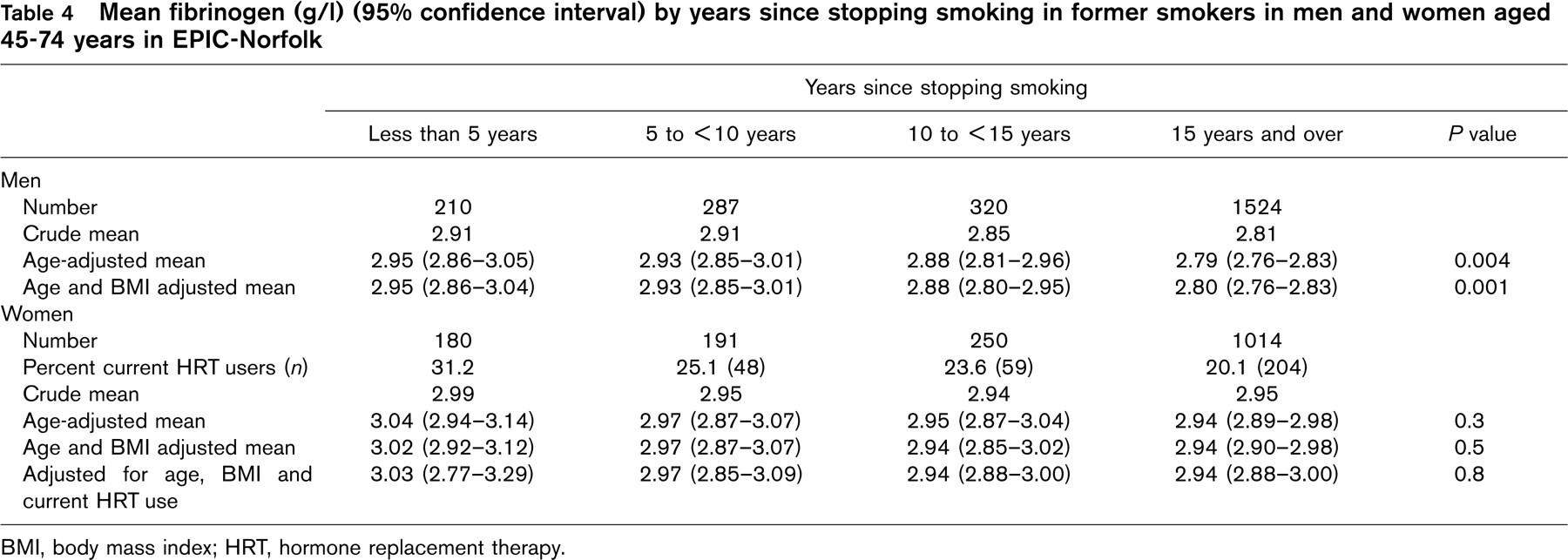
BMI, body mass index; HRT, hormone replacement therapy.
Our measures of smoking were based on self-report. We did not undertake biochemical validation of smoking status. However misclassification of smoking status would lead to an underestimate of the relationship between smoking status and fibrinogen and could not therefore account for our results. In contrast to previous work we have adjusted for both age and BMI, both of which were strongly related to plasma fibrinogen in our data. We have also minimized confounding due to prevalent vascular disease and cancer by excluding individuals with these conditions.
The mechanism by which smoking influences plasma fibrinogen levels remains unclear. Fibrinogen synthesis has been shown to be higher in smokers than in non-smokers [23]. Fibrinogen synthesis is largely under the control of inflammatory cytokines such as interleukin 6 [24] and it has been hypothesized that smoking provokes a chronic inflammatory response leading to increased fibrinogen production [25]. In addition, smoking has been shown to stimulate catecholamine release [26], which in turn has been shown to increase fibrinogen synthesis in animal models [27]. However neither of these mechanisms can explain the continued long-term elevations in plasma fibrinogen seen in ex-smokers in cross-sectional studies, and it may be that this effect reflects the level of inflammation due to atherosclerosis itself.
Predictors of plasma fibrinogen on multivariate analysis in men and women aged 45–74 years in EPIC-Norfolk
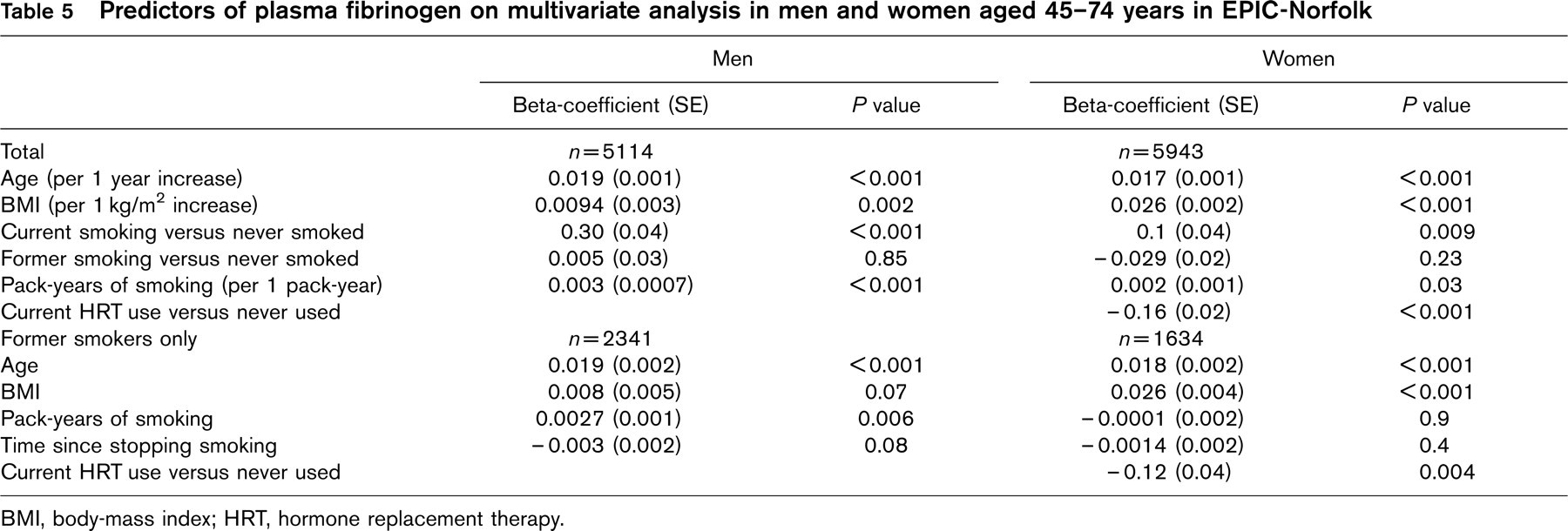
BMI, body-mass index; HRT, hormone replacement therapy.
Our data suggest that within the first 15 years since smoking cessation plasma fibrinogen falls by 0.1–0.3 g/l in men and up to 0.4 g/l in women. Data from the Northwick Park Heart Study suggest that this would correspond to a fibrinogen-mediated reduction in the risk of a major CHD event of around 15–20% in men [16]. Data from the British Doctors Study [28] suggest that the relative risk of a CHD death falls by 50% within 10 years of smoking cessation. The beneficial effect of smoking cessation on CHD mortality may be partly mediated by a fall in plasma fibrinogen.