
Abstract
Background
The CURE study demonstrated that clopidogrel prevents a range of ischaemic cardiovascular events in patients with Acute Coronary Syndromes (unstable angina or non-ST-segment elevation MI).
Design
We undertook an economic analysis of the use of clopidogrel in the UK, USA, Sweden, France and Canada based on the CURE study.
Methods
The costs of hospitalization, study drug and other medications were calculated, based on resource utilization for all patients in CURE. Unit costs were obtained for all resource items for each country, and are reported in local currencies in 2001 prices.
Results
While hospitalization costs were lower in the clopidogrel group, when the acquisition cost of clopidogrel for 9 months is included, the average cost per patient is higher in the clopidogrel group than the placebo group in all countries [difference in costs (with 95% CI) UK £208 (119, 297), US$451 (58, 845), SKr 2571 (728, 4412), Fr ∊325 (85, 565), C$161 (−185, 506)]. The absolute reduction in the number of total primary events was 2.0%, resulting in an incremental cost-effectiveness ratio (ICER) of £10,366 in the UK, $22,484 in the USA, SKr 127,951 in Sweden, ∊16,186 in France, and C$7973 in Canada per primary event avoided with clopidogrel.
Conclusions
Clopidogrel in CURE reduced hospitalization costs but the acquisition cost of clopidogrel creates an overall increase in direct health care costs over 9 months. Nevertheless, the cost-effectiveness is in a range comparable to other therapies currently utilized for acute coronary syndromes.
Introduction
Clopidogrel, a thienopyridine, is an antiplatelet agent that inhibits platelet aggregation induced by adenosine diphosphate (ADP). In combination with aspirin, which blocks the thromboxane mediated pathway, the two agents have additive effects in inhibiting platelet aggregation. In patients undergoing percutaneous coronary intervention with stenting, a thienopyridine (clopidogrel or ticlopidine) when added to aspirin decreases the incidence of death and myocardial infarction compared with aspirin alone or warfarin [1]. The CURE trial (Clopidogrel in Unstable angina to prevent Recurrent Events) evaluated the efficacy and safety of clopidogrel plus aspirin compared with aspirin alone when initiated early and continued long term (up to 12 months, average of 9 months), in patients with acute coronary syndromes (ACS).
Clopidogrel reduced the risk of the primary outcomes rate of cardiovascular death, myocardial infarction and stroke. Additionally, there was a reduction in refractory ischaemia needing urgent intervention, other ischaemic events and pulmonary oedema. These results have influenced the 2002 ACC/AHA Guidelines for the Management of Patients With Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction [2] and European Society of Cardiology [3] guidelines which recommend the use of the combination of aspirin and clopidogrel. Therefore, it is important to assess the economic consequences of the use of clopidogrel in the treatment of ACS based upon the results of CURE. In this article, we estimate the cost-effectiveness of the use of clopidogrel in ACS in five countries (UK, USA, Sweden, France and in Canada) based upon the CURE study.
Methods
Clinical trial
The CURE study, was a large, multi-centre randomized controlled trial. A total of 12,562 patients were recruited from December 1998 to September 2000 at 482 centres from 28 countries. Seven hundred and thirty-seven patients were recruited in the UK, 462 in the USA, 360 in France, 260 in Sweden, 1761 in Canada and 8982 from other countries. Patients were eligible if they were hospitalized within 24 h of onset of symptoms indicative of ACS, and did not have significant ST segment elevation. Patients were randomized to receive clopidogrel (loading dose of 300 mg followed by 75 mg per day) or a placebo for an average period of 9 months. All patients received acetyl salicylic acid (75–325 mg daily) [4].
All patients received conventional treatments for their condition, regardless of randomization assignment. These treatments include thrombolytic agents, heparin (unfractionated or low molecular weight), diuretics, anti-anginal therapy, antihypertensive medication, and cholesterol-reducing agents, as recommended by their local physicians. Although the use of glycoprotein IIb/IIIa receptor antagonists was discouraged in the trial unless patients developed refractory ischaemia, their use was allowed during PCI. Therefore, all comparisons are based upon clopidogrel versus placebo in addition to the above therapies.
The clopidogrel group demonstrated a lower rate of the first primary outcomes (9.3% vs. 11.4%, relative risk 0.80, P < 0.001) and lower rates of refractory ischaemia in hospital (1.4% vs. 2.0%, relative risk 0.68, P < 0.01), and heart failure (3.7% vs. 4.4%, relative risk 0.82, P = 0.03). All components of the primary outcome showed similar trends in favour of clopidogrel. Major bleeds were significantly more common in the clopidogrel group (3.7% vs. 2.7%, relative risk 1.38, P = 0.001) but the differences in life-threatening bleeds were not statistically significant (2.2% vs. 1.8%, relative risk 1.21, P = 0.13). There was a significant increase in the risk of minor bleeds (5.1% vs. 2.4%, relative risk 2.12, P < 0.001). Utilization of thrombolytic therapy (1.1% vs. 2.0 %, relative risk 0.57, P = 0.001) and glycoprotein IIb/ IIIa receptor inhibitor (5.9% vs. 7.2%, relative risk 0.82, P = 0.003) was significantly reduced in the clopidogrel group.
Overview of the economic analysis
The hypothesis of the CURE economic analysis was that clopidogrel is more expensive but more effective than placebo. An incremental cost-effectiveness analysis was therefore performed, comparing the differences in costs and effectiveness between intervention and no intervention, using the placebo group result as proxy for no intervention. Costs included in the analysis are direct medical care costs for hospitalization and drugs [5, 6]. No data are available from the CURE trial to calculate direct costs associated with outpatient visits and testing or indirect costs due to loss of productivity. Direct costs are evaluated from a societal perspective. Costs in 2001 price level are reported in pounds (£) for UK, in American dollars (US$) for the USA, in kronor (SKr) for Sweden, in Euro (∊) for France, and in Canadian dollars (C$) for Canada. These five countries were selected as good unit cost data and qualified collaborators were available. The economic team from these five countries was selected and the protocol for this analysis was finalized before clinical results were presented. Discounting was not performed, since follow-up was a maximum of one year and the impact on costs or outcomes after the study period was not considered in the analysis. Health care costs consist of two components: (1) health care services or resource utilization as measured in the clinical trial and (2) unit costs for health care services utilized in the different countries. The analysis is done for each country using local unit costs, but utilizes resource use information and clinical outcomes for all 12,562 patients.
Health care utilization
All major cardiovascular health care related resources were collected prospectively. Total length of stay in hospital and all revascularization procedures (including subsequent hospitalizations) were collected as well as medications taken in hospital and at home. Diagnostic testing, therapeutic procedures and drugs taken during interim hospitalizations, were also recorded. Ambulatory care and outpatient diagnostic testing (other than coronary angiography) were not recorded. Since the majority of resource intensive procedures or testing are performed while patients are hospitalized, it is likely that most of the major components of health care resource utilization were collected. Possible exceptions would include same day testing not requiring hospitalization, such as nuclear imaging studies or echocardiograms. Use of open-label clopidogrel and adherence to double-blind treatment were recorded during hospitalizations and at periodic follow-up visits. Using a pre-defined algorithm for all countries except Canada, the initial and subsequent hospitalizations were assigned a Diagnosis Related Group (DRG) similar to those used by Medicare in the USA. During the initial hospitalization, there is a reduction in the number of complex MIs as well as procedures like CABG and PTCA in the clopidogrel group. In the follow-up period, there is a reduction in the incidence of complex MI, stroke and chest pain in the clopidogrel group but also an increase in the number of patients with unstable angina. Noncardiovascular events were also collected but were not included in this final analysis as their frequency was low and they were equally distributed between both groups. In Canada, as no DRG system exists, we relied on a detailed case-costing system developed at our institution to record drugs, procedures, investigations and length of stay. The frequency of each DRG and a detailed description of unit costs for each country could be found on the Population Health Research Institute web site.
Statistical analysis
Unit costs were applied to patient-level utilization data to arrive at a cost per patient, and the average cost within each treatment group (active/placebo) was calculated. Since the cost data were not normally distributed, a bootstrap analysis was used to calculate standard errors and 95% confidence intervals for the difference in average costs. The bias corrected and accelerated (BCa) method was used to obtain confidence intervals [7] for average costs. Incremental cost-effectiveness ratios (ICER) were calculated in terms of incremental cost per CV death, myocardial infarction or stroke prevented. Confidence intervals around the ICERs were also calculated using the BCa method. All analyses were completed using SAS 8.0.
Results
Costs
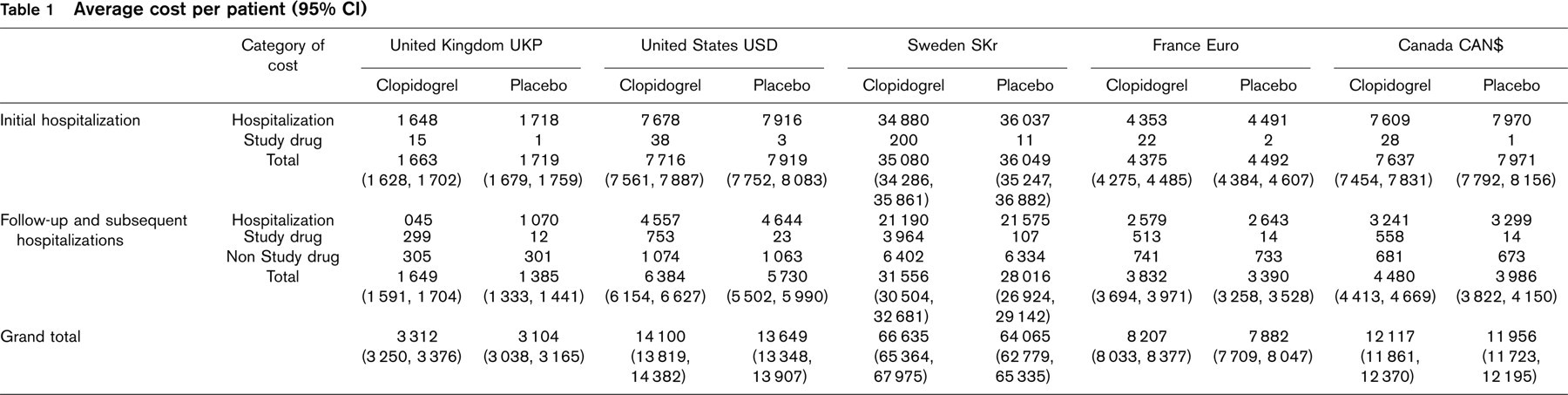
Average costs of the initial hospitalization (including study drug) were reduced for the clopidogrel group compared with the placebo group in all countries (Table 1). The difference is a saving of £56 (−109, −2) (mean ± 95%CI) per patient in UK, US$203 (−439, 34) in the USA, SKr 969 (−2088, 150) in Sweden, h118 (−270, 36) in France, C$334 (−596, −72) in Canada. The mean duration of treatment with clopidogrel was 7.62 days in the clopidogrel group and 0.46 days in the placebo group (open-label).
The average cost of the subsequent hospitalizations was marginally reduced for the clopidogrel group in all countries. The average cost of nonstudy medications was substantial in both groups but comparable. The average acquisition cost for clopidogrel (blinded and open-label) was significantly increased in the clopidogrel group. The mean duration of treatment with clopidogrel was 231 days in the clopidogrel group (less than 2% as open-label) and 4.5 days in the placebo group (open-label). These follow-up costs were added and the average cost during the follow-up period was higher for the clopidogrel group compared with the placebo group in all countries. The difference is £264 (186, 342) per patient in UK, US$654 (319, 989) in the USA, SKr 3540 (1983, 5097) in Sweden, ∊443 (243, 641) in France, C$494 (255, 733) in Canada.
When the initial hospitalization and follow-up period are combined, total costs are significantly higher with clopidogrel compared with placebo in all countries, except Canada. The difference is £208 (119, 297) per patient in UK, US$451 (58, 845) in the USA, SKr 2571 (728, 4412) in Sweden, ∊325 (85, 565) in France, C$161 (− 185, 506) in Canada.
Cost-effectiveness
The absolute risk reduction for the occurrence of any primary outcome (including multiple events) is 2.0%. The ICER is £10,366 (4411, 42,981) per event avoided with clopidogrel in UK, US$22,484 (1826, 97,354) in USA, SKr 127,951 (26,212, 461,424) in Sweden, ∊16,186 (3311, 72,368) in France, C$7973 (− 9401, 54,235) in Canada.
We have elected to use the reductions in all occurrences of the various components of the primary outcome (2.0%) as opposed to the reduction in the first event only of the composite outcome as reported in the CURE [4] manuscript, because of the additional costs incurred when multiple events in the same individual occur. However, if we had used prevention of the first event, the ICER would change only slightly to become £9876 (4632, 23,931) per event avoided with clopidogrel in UK, US$ 21,423 (2285, 59,365) in USA, SKr 121,913 (31,924, 314,281) in Sweden, ∊15,422 (3112, 39,414) in France, C$7597 (− 8046, 37,142) in Canada.
Subgroup analysis and duration of therapy
The benefit of clopidogrel in CURE is consistent among low, intermediate and high-risk patients with ACS stratified by the TIMI risk score [8]. The incremental cost differences and ICERs for these subgroups were assessed, and we found no significant heterogeneity among the three subgroups (data not shown). Results from calculation of average cost-effectiveness ratios for treatment with clopidogrel for 30 days, and 3, 6 and 9 months are presented in Table 2.
Average cost per patient (95% CI)
Discussion
The purpose of this economic analysis was to assess the economic implications of the use of clopidogrel in patients with acute coronary syndromes based on the approach and the results of the CURE study. We found that for all five countries studied, clopidogrel reduced the average cost of the initial hospitalization. These reductions are explained by less need for additional therapy for unstable angina with more patients treated medically (with or without coronary angiography) and a lower initial rate of revascularization procedures (PCI or CABG). Furthermore, there was a reduction in the rate of complex myocardial infarctions (DRG 121) in favour of ‘simple’ MIs (DRG 122), hence a change in the case-mix of patients in the clopidogrel group. The same trend is seen for subsequent hospitalizations. However, the acquisition cost of clopidogrel during the follow-up period resulted in an overall increase in the direct health care costs for the clopidogrel group in all countries.
The recent ACC/AHA 2002 [2] and the ESC Guidelines for the Management of Patients With Unstable Angina and Non-ST-Segment Elevation [3] recommends the use of aspirin, heparin (unfractionated or low molecular weight), clopidogrel and intravenous platelet GP IIb/IIIa antagonists. In particular, clopidogrel is recommended for periods of about 9 months to 12 months. In order to facilitate the comparison of clopidogrel as currently recommended with other medical therapies for acute coronary syndromes, we have tabulated the clinical results and economic analyses of key trials of all proven agents. These data include the ESSENCE [9] trial for enoxaparin, PRISM-PLUS [10] for tirofiban, PURSUIT-US [11] for eptifibatide and PURSUIT-WE [12] (Western Europe) and CURE for clopidogrel. Comparison of various trials and their economic component requires cautious interpretation as each study has a slightly different patient population and the value of the currency has changed over time. We extracted the data directly from the original manuscript and made no attempt to compensate for these differences. All of these economic studies have comparable, but not identical designs. Data relating to hospital costs, professional fees and study drug were extracted directly from the manuscript, in the original currency. The results are limited to direct health care costs up to 6 months and do not consider long-term modelling or extrapolation on life-year gained. In order to facilitate comparison, results and costs from CURE were re-computed to have a similar endpoint to the other studies, that is death and MI at 30 days. Results are depicted in Table 3. The cost-effectiveness of clopidogrel at 1 month and 6 months compares favourably with all other forms of medical therapies for acute coronary syndromes.
Cost-effectiveness ratios (95% CI) according to length of follow-up

∗DS: Dominant Strategy (best possible situation i.e. better clinical results with lower costs).
Comparison of cost difference and ICER between control and active drug for various treatments in ACS
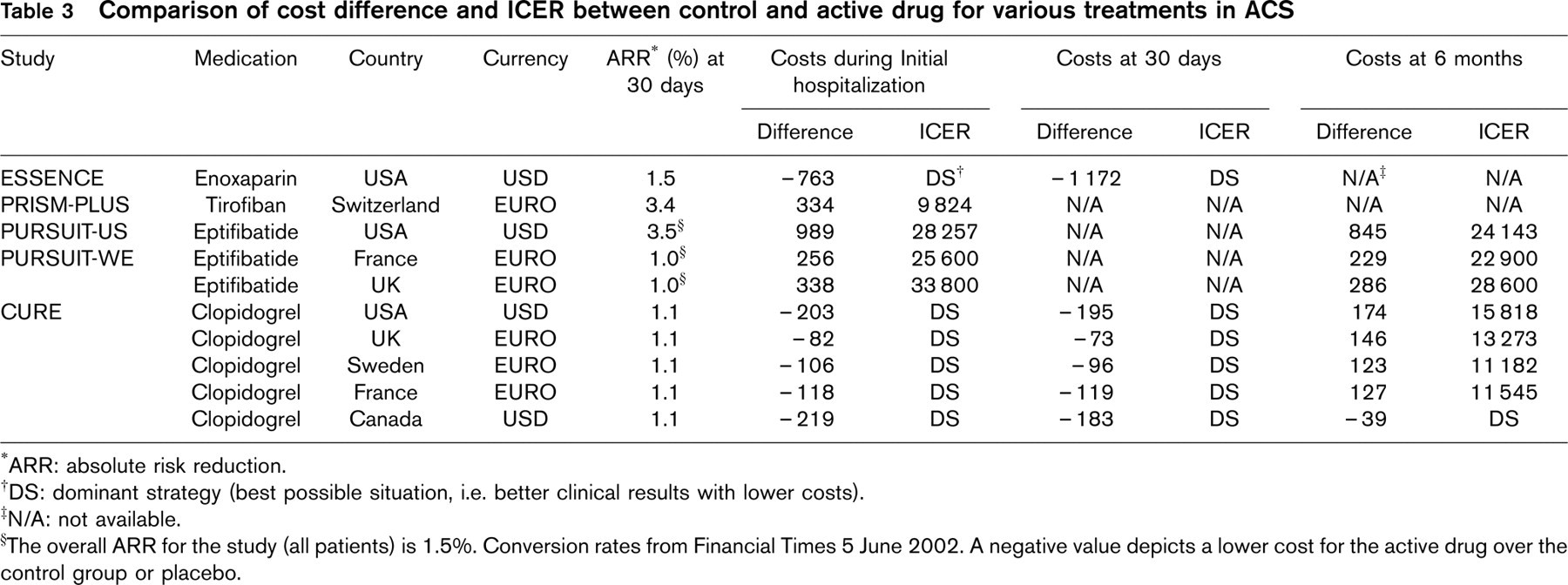
∗ARR: absolute risk reduction.
†DS: dominant strategy (best possible situation, i.e. better clinical results with lower costs).
‡N/A: not available.
§The overall ARR for the study (all patients) is 1.5%. Conversion rates from Financial Times 5 June 2002. A negative value depicts a lower cost for the active drug over the control group or placebo.
Some limitations in the present analysis should be considered. The economic analysis was designed before the study was completed. Although most health care utilizations were prospectively recorded, office visits, out of hospital testing and same day in-hospital testing were not recorded. In addition, nonmedical costs such as loss of productivity and the time provided by family and friends caring for patients was not collected. From our clinical experience, as well as from the experience of the study, it is reasonable to believe that these costs are not going to be higher for the clopidogrel group compared with the placebo group. On the contrary, these costs are likely to be lower due to the reduction in major cardiovascular events. Hence it seems that our analysis can be seen as a reasonable proxy for a societal perspective or even an overestimation of the true societal cost-effectiveness of clopidogrel.
Our approach was to base clinical outcome and resource utilization on the results of the whole trial, with cost calculations based on unit costs in individual countries. This approach is justified, as we assume no statistical heterogeneity in the treatment benefit by country or region, and a separate analysis of individual country results would be underpowered and would therefore be statistically unreliable. Further, by using an event driven costing system (DRG) that is country specific, variations in practice pattern between different countries should be minimized. Although the occurrence of events like myocardial infarction, angina and stroke are not likely to be influenced by the health care system or the country studied, the approach to patient management may vary and using country specific costs allows for some variation in practice styles.
Results for Canada indicate a better cost-effectiveness ratio compared with the other countries. This is in part due to the use of a case-costing system (as no DRG system exists in Canada) that records all procedures during a specific hospitalization and the specific length of stay, avoiding lumping all resources into a single code. The DRG system is a case based method of reimbursement and does not take account of specific issues in CURE such as a small but significant increase in minor and major bleeds (with an excess of 113 blood units) but also a small but significant reduction in the length of stay associated with clopidogrel (10.3 vs. 10.4, P = 0.029) and in the utilization of thrombolytic therapy and glycoprotein IIb/IIIa receptor inhibitor.
The average cost-effectiveness ratios presented in Table 2 must be interpreted with caution as the appropriate analysis for evaluating the relative merits of providing therapy for different lengths of time is one which evaluates the marginal (or incremental) costs relative to the marginal (or incremental) benefits, going from one time point to the next. This study is not designed to evaluate the marginal cost-effectiveness for varying lengths of treatment as the two groups of patients will not balance in a correct way when the marginal cost-effectiveness is calculated. Therefore, taking multiple factors into consideration, clopidogrel given for up 12 months (mean 9 months) as currently recommended by the ACC, AHA and the ESC has an acceptable cost-effectiveness ratio in Western countries. Decisions regarding the duration of therapy need to be individualized based on patient profile, the relative costs of various therapies and the overall economic status of particular societies.
Clopidogrel reduces the costs of initial hospitalization and subsequent hospitalizations but the acquisition cost of clopidogrel during the follow-up period creates an overall increase in direct costs. However overall for 9 months of clopidogrel therapy, the incremental cost-effectiveness ratios compares favourably with other medical therapies used for acute coronary syndromes.
Footnotes
Acknowledgements
We would like to acknowledge the collaboration of Mrs Isabelle Durand-Zaleski for her expertise regarding unit costs in France. Sanofi-Synthelabo and Bristol-Myers-Squibb were the sponsors of the CURE study. They had no role in the study design, data collection, data analysis, data interpretation, or writing this manuscript.