
Abstract
Background
The benefits of inspiratory muscle training (IMT) in patients with chronic heart failure (CHF) have been inadequately studied.
Design and methods
Using a prospective, age and sex-matched controlled study, we investigated 35 patients with moderate to severe CHF (NYHA class II–III and left ventricular ejection fraction 24.4 ± 1.3% [mean ± SEM]). An incremental respiratory endurance test using a fixed respiratory workload was provided by software with an electronic mouth pressure manometer interfaced with a computer. The training group (n = 20) exercised at 60% of individual sustained maximal inspiratory pressure (SMIP) and the control group (n = 15) at 15% of SMIP. All patients exercised three times weekly for 10 weeks. Pulmonary function, exercise capacity, dyspnea and quality of life were assessed, pre- and post-training.
Results
The training group significantly increased both maximum inspiratory pressure (Pimax), (111 ± 6.8 versus 83 ± 5.7cmH2O, P<0.001), and SMIP (527822 ± 51358 versus 367360 ± 41111 cmH2O/sec × 10-1, P < 0.001). Peak VO2 increased after training (17.8 ± 1.2 versus 15.4 ± 0.9 ml/kg/min, P< 0.005), as did the six-minute walking distance (433 ± 16 versus 367 ± 22 meters, P < 0.001). Perceived dyspnea assessed using the Borg scale was reduced for both the treadmill (12.7 ± 0.57 versus 14.2 ± 0.48, P < 0.005) and the walking (9 ± 0.48 versus 10.5 ± 0.67, P< 0.005) exercise tests and the quality of life score was also improved (21.1 ± 3.5 versus 25.2 ± 4, P < 0.01). Resting heart rate was significantly reduced with training (77 ± 3.3 versus 80 ± 3beats/min, P < 0.05). The control group significantly increased Pimax (86.6 ± 6.3 versus 78.4 ± 6.9cmH2O, P < 0.05), but decreased SMIP (274972 ± 32399 versus 204661 ± 37184cmH2O/sec × 101, P < 0.005). No other significant effect on exercise capacity, heart rate, dyspnea, or quality of life was observed in this group.
Conclusion
Inspiratory muscle training using an incremental endurance test, successfully increases both inspiratory strength and endurance, alleviates dyspnea and improves functional status in CHF.
Introduction
Exertional fatigue and dyspnea limit the activities of daily living in patients with chronic heart failure (CHF). Mechanisms include limb muscle atrophy, an increase in easily fatiguable type IIb fibres, a decrease in oxidative enzymes with an earlier shift to glycolytic mechanisms and a decrease in size and number of mitochondria [1, 2]. Dysfunction of the respiratory muscles has also been reported in patients with CHF. Consistent findings of reduced inspiratory pressure-generating capacity indicate a decrease in inspiratory muscle strength while a reduction in expiratory muscle strength has not been confirmed [3–5. Decreases in inspiratory muscle strength may be attributed to histological and biochemical changes. Biopsies of the diaphragm in patients with CHF show structural abnormalities suggesting the occurrence of fibre regeneration and/or transformation [6]. Type IIb fibres, which have been proposed to produce greater force, are fewer in these patients whereas fatigue-resistant type I fibres seem to be dominant with increased oxidative capacity of the diaphragm [7]. Other mechanisms may include over-activation of pro-inflammatory cytokines and decrease in regional blood flow associated with endothelial dysfunction characterizing the syndrome of CHF [8, 9]. Respiratory muscle endurance is also reduced to nearly half compared to healthy subjects. This decrease may be attributed to the increased work of breathing with increased ventilation leading to respiratory fatigue [10]. Respiratory muscles seem to exhibit the profile of an oxidative muscle adapting to a different pathophysiology than limb muscle.
Mancini and co-workers [11] established that perceived dyspnea is significantly correlated to the pressure generating capacity of the respiratory muscles. However, the benefits of respiratory muscle training concerning exercise capacity and dyspnea in patients with CHF remain controversial. Most of the studies consist of a small number of patients, occasional lack of control groups whilst the methodology of training the respiratory muscles vary and may not guarantee a training effect [12–14. Reviews of respiratory muscle training have highlighted the need for a fixed respiratory workload during training [15, 16].
In the present study, we aimed to train the respiratory muscles according to skeletal muscle training principles providing a fixed workload throughout respiratory effort (residual volume to total lung capacity) in direct relation to individual capacity. We used an incremental inspiratory training regime, since inspiratory muscles suffer more severe weakness than expiratory muscles. Incremental respiratory loading has been successfully used in normal and cystic fibrosis patients [17–19. To the best of our knowledge we are the first to introduce this method of training in patients with CHF. We postulated that if inspiratory muscles are trained throughout a range corresponding to skeletal muscle training principles, an increase in inspiratory muscle endurance and strength might modify the threshold of perceived dyspnea, increase exercise capacity and improve quality of life in patients with CHF.
Methods
Patient population
A total of 37 patients with CHF were recruited from the out-patient heart failure clinic for this study. Eligible patients were classified as II and III functional class according to New York Heart Association (NYHA) classification, with left ventricular ejection fraction (LVEF) less than or equal to 40%. Patients were assigned to either a training (n = 20) or control (n = 17) group whilst patients in the control group were age and sex-matched to the patients in the training group. Table 1 lists selected characteristics pertaining to each group completing the study.
Baseline characteristics of training group (TG) versus control group (CG)
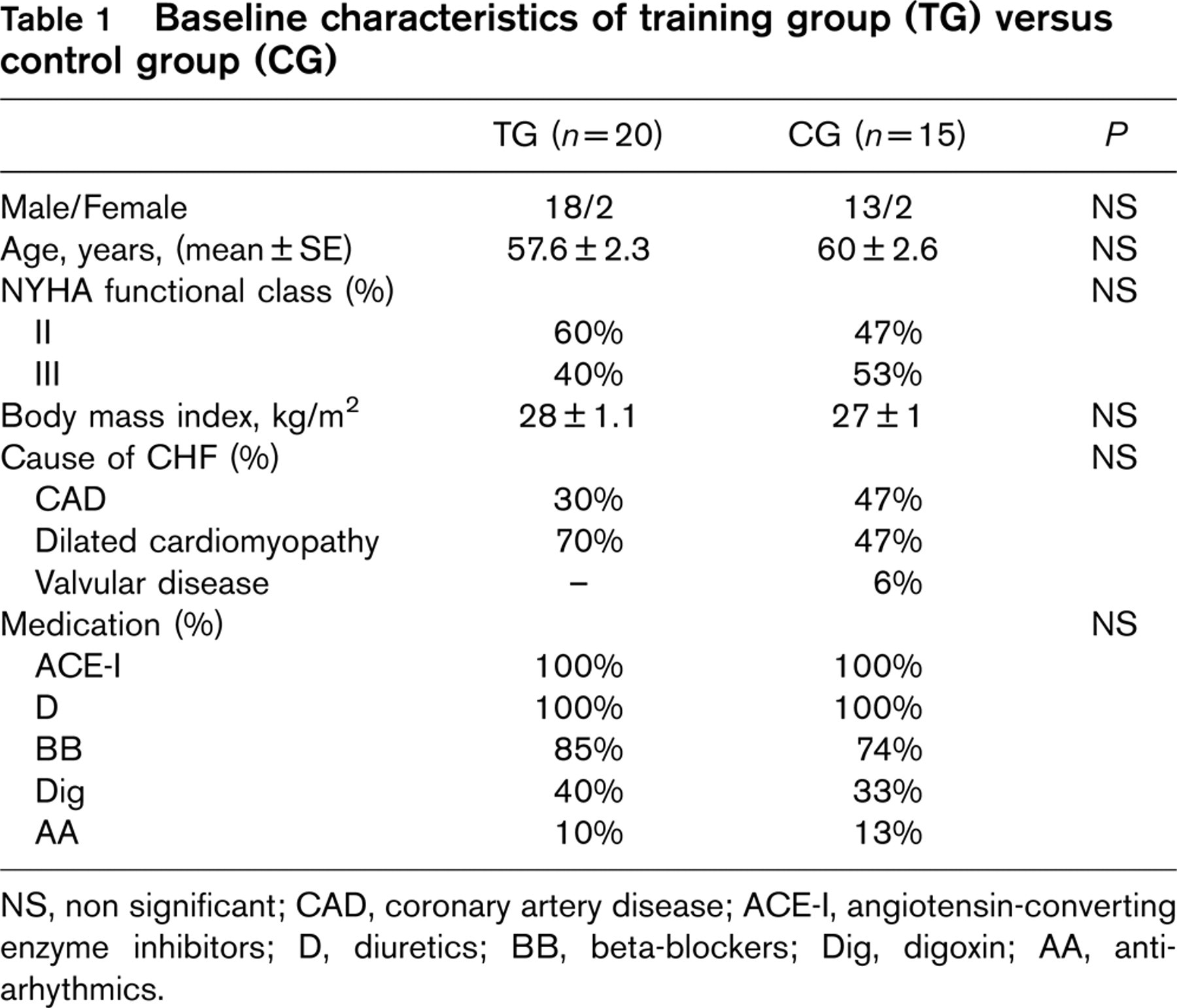
NS, non significant; CAD, coronary artery disease; ACE-I, angiotensin-converting enzyme inhibitors; D, diuretics; BB, beta-blockers; Dig, digoxin; AA, antiarhythmics.
Exclusion criteria were pulmonary disease, cognitive impairment and current smoking. The Hospital Institutional Review Committee approved the present study, and written informed consent was obtained from all subjects.
Baseline studies
Prior to participation in the study protocol, all patients underwent echocardiography, pulmonary function tests, and assessment of exercise capacity, dyspnea, and quality of life. The same tests were performed after the completion of the study.
Pulmonary function tests
All patients were assessed using spirometry. Measurements were performed with a Jaeger system (Masterlab, Jaeger, Wuerzberg, Germany). Spirometric indices were calculated as the best of three satisfactory efforts, defined as the effects associated with the highest sum of forced vital capacity (FVC) and forced expiratory volume in one second (FEV1).
Inspiratory muscle strength was assessed by measuring maximum static inspiratory capacity (Pimax) at residual volume. Inspiratory muscle endurance was assessed by asking the subject to maintain Pimax over time, from residual volume to total lung capacity, i.e., sustained maximal inspiratory pressure (SMIP)/time [19], (Fig. 1). Measurements were taken in the seated position and all patients were verbally encouraged during respiratory effort. Three repeated efforts in two different days were made, with several minutes of rest allowed between each effort. Measurements were taken using software with an electronic pressure manometer with a 2mm leak to avoid glottis closure, (TRAINAIR; Project Electronics Ltd, Kent, UK), interfaced with a computer. The highest values achieved in the first second and maintained over time were used as Pimax and SMIP respectively, in the analysis. Inspiratory volume (IV) was also measured during the best SMIP achieved.
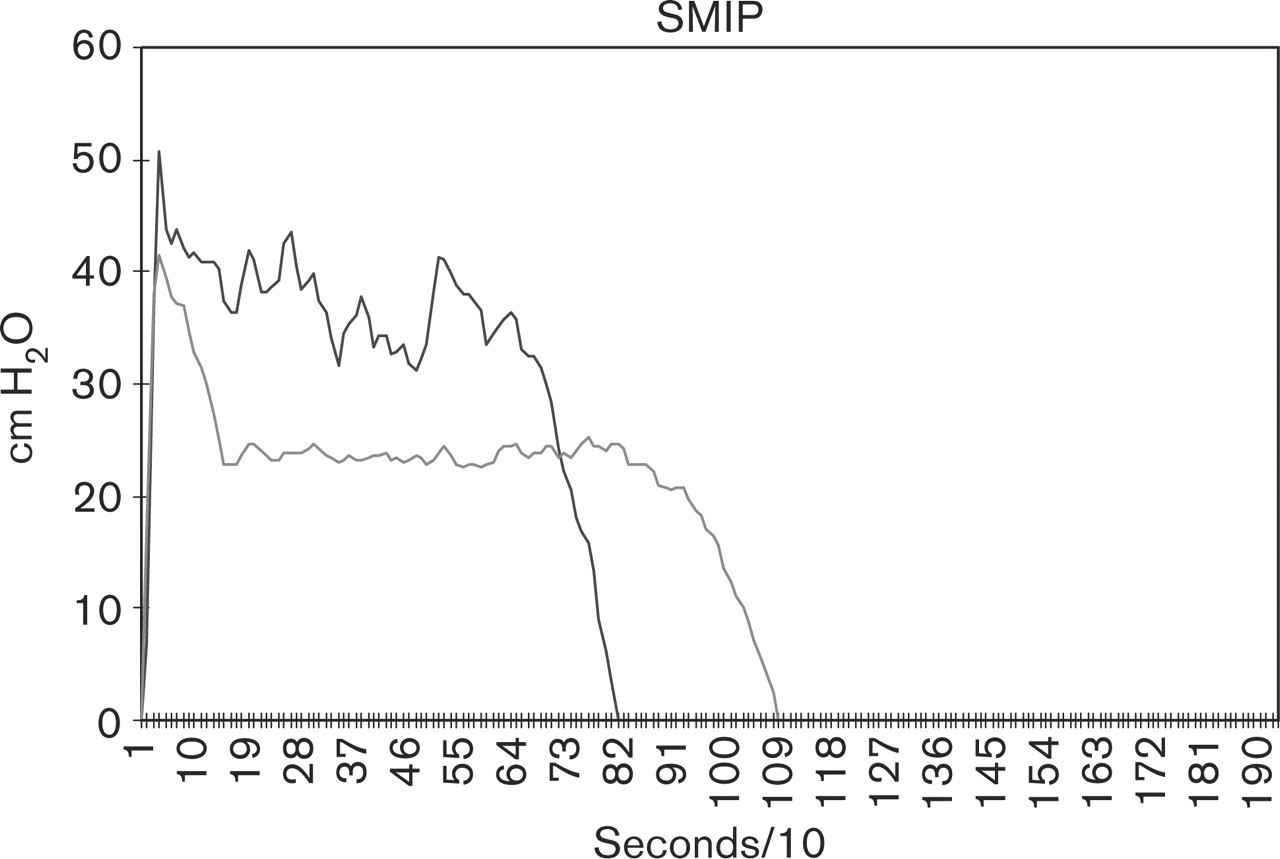
Two inspiratory efforts by one subject to indicate SMIP/time, expressed as the area under the pressure-time curve. Ten pressure (cmH2O) measurements were taken every one second. SMIP, sustained maximal inspiratory pressure.
Cardiopulmonary exercise testing
Patients performed a cardiopulmonary exercise stress test to evaluate their exercise capacity by measuring VO2max (ml/kg/min). Exercise testing with respiratory gas exchange measurements were performed by using the Medgraphics CPX/MAX (Medical Graphics Corp., St. Paul, Minnesota) measuring system, while patients exercised on a treadmill according to the Dargie protocol [20]. Peak oxygen consumption (peak VO2) during exercise was recorded as the mean value during the last minute of exercise. The level of perceived dyspnea was recorded according to the Borg scale at the end of the test.
The six-minute walk test
The six-minute walk test was carried out in a 64 metre unobstructed corridor with rest points provided. Patients were told the time remaining, when two and four minutes had elapsed. Dyspnea was assessed at the end of the walk by the Borg scale.
Quality of life
The Minnesota Living with Heart Failure (LIhFE) questionnaire was used to assess quality of life [21].
Exercise training and control training programs
All patients were supervised in the hospital during training, which occurred three times weekly for 10 weeks.
An incremental respiratory endurance regime was used to train the inspiratory muscles. Both groups were exercised at a percentage of individual SMIP measured at each training session, following the same procedure as the baseline measurements. This was achieved using TRAINAIR® and serial presentations of computer templates were re-drawn at percentage SMIP. Patients in the training group were exercised at 60% of individual SMIP and patients in the control group at only 15% of their SMIP. If patients failed to achieve 90% of the predetermined training template for three consecutive efforts, the exercise session was stopped. The test had different levels of training with six inspiratory efforts at each level. Initially, the first level presented templates at 60 second rest intervals over its six inspiratory efforts, but at the second level through to the sixth level, this rest period was reduced to 45, 30, 15, 10, and 5 seconds respectively. After the sixth level, the rest period was kept at 5 seconds. The training group was trained to respiratory fatigue whilst patients in the control group were asked to stop after the first six levels of training. Visual feedback was used through the software to enhance the training response, (Fig. 2). All patients wore a nose-clip during training. Written instructions on the screen asked subjects to await a visible signal to start their inspiratory efforts and an on-screen clock facilitated the timing of each sustained inspiratory effort. Verbal encouragement was given to all subjects during training.
Arterial blood pressure was measured at the beginning, middle and peak of each training session by a cuff sphygmomanometer and heart rate was monitored continuously with a three-lead ECG, both connected to a screen monitor (Sirecust 342 R, Siemens).
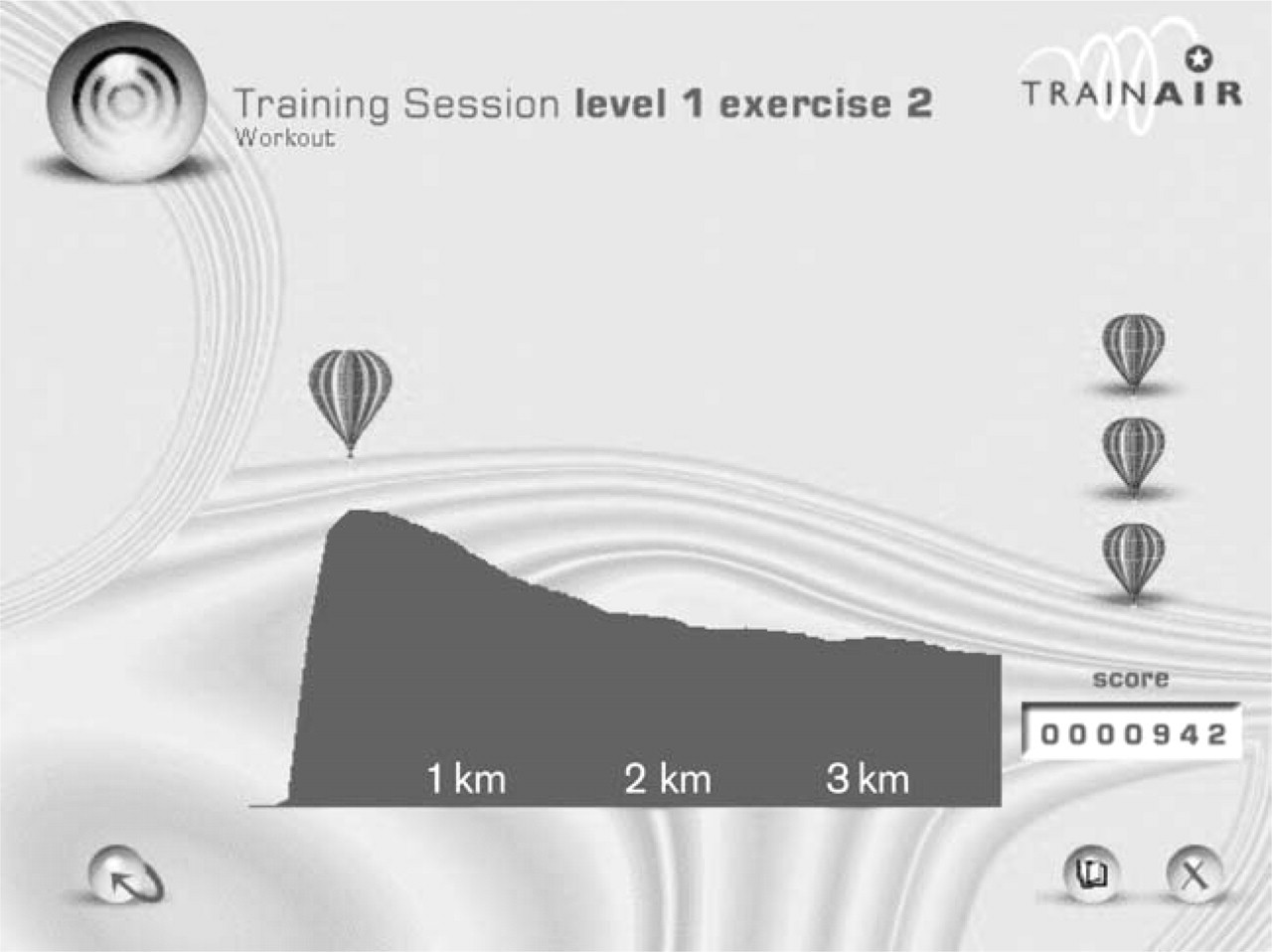
Created template by the software as a percentage (60%) of individual sustained maximal inspiratory pressure of a patient in the training group. Score is in arbitrary units to indicate progress.
The patients were asked to avoid physical activity above their normal routine during the study period.
Statistical analysis
The two-tailed Student paired or unpaired t-tests were used as appropriate. The relations between variables were examined by linear regression analysis to confirm that any change was only influenced by the intervention and not by other baseline parameters (gender, age, body mass index, cause of heart failure, medication).
Correlations were assessed using the non-parametric Spearman's test. A probability value < 0.05 was considered to be significant. All data were calculated as mean ± SE.
Results
Both groups were comparable with regard to baseline characteristics. Thirty-five patients completed the study. Two patients from the control group failed to complete the study due to long-distance travelling and were excluded from the results (Table 1). No significant alteration in drug therapy occurred in either group.
Pulmonary function tests
In the training group, significant increases occurred in inspiratory muscle strength (Pimax), endurance (SMIP) and inspiratory volume (IV). In the control group a smaller but significant increase occurred in inspiratory strength, but both inspiratory endurance and IV were significantly reduced, (Fig. 3). A strong correlation between percentage changes in inspiratory strength and endurance was shown in the training group (Fig. 4). Additional results of spirometry showed a sufficient increase in FVC in the training group so that FEV1/ FVC decreased significantly. However, individual values of FVC and FEV1 did not change significantly. In the control group no significant change in baseline spirometry occurred with training at 15% of SMIP (Table 2).
Cardiopulmonary exercise testing
Inspiratory muscle training produced a significant increase in peak VO2, exercise time duration and minute ventilation (VE) in the training group. The mean percentage increase in peak VO2, was 16% (P = 0.002). No change was obtained in VO2 at anaerobic threshold (AT) or ventilation response to exercise (VE/VCO2). No significant change occurred in peak VO2 or other exercise parameters, in the control group, (Fig. 5). Dyspnea rated on the Borg scale was significantly reduced after ergospirometry compared to baseline value in the training group while no change was observed in the control group, (Table 3). Resting heart rate measurements were significantly reduced only in the training group measured both at treadmill and pulmonary testing. Peak heart rate at treadmill testing tended to decrease only for the training group but not significantly (Table 3).
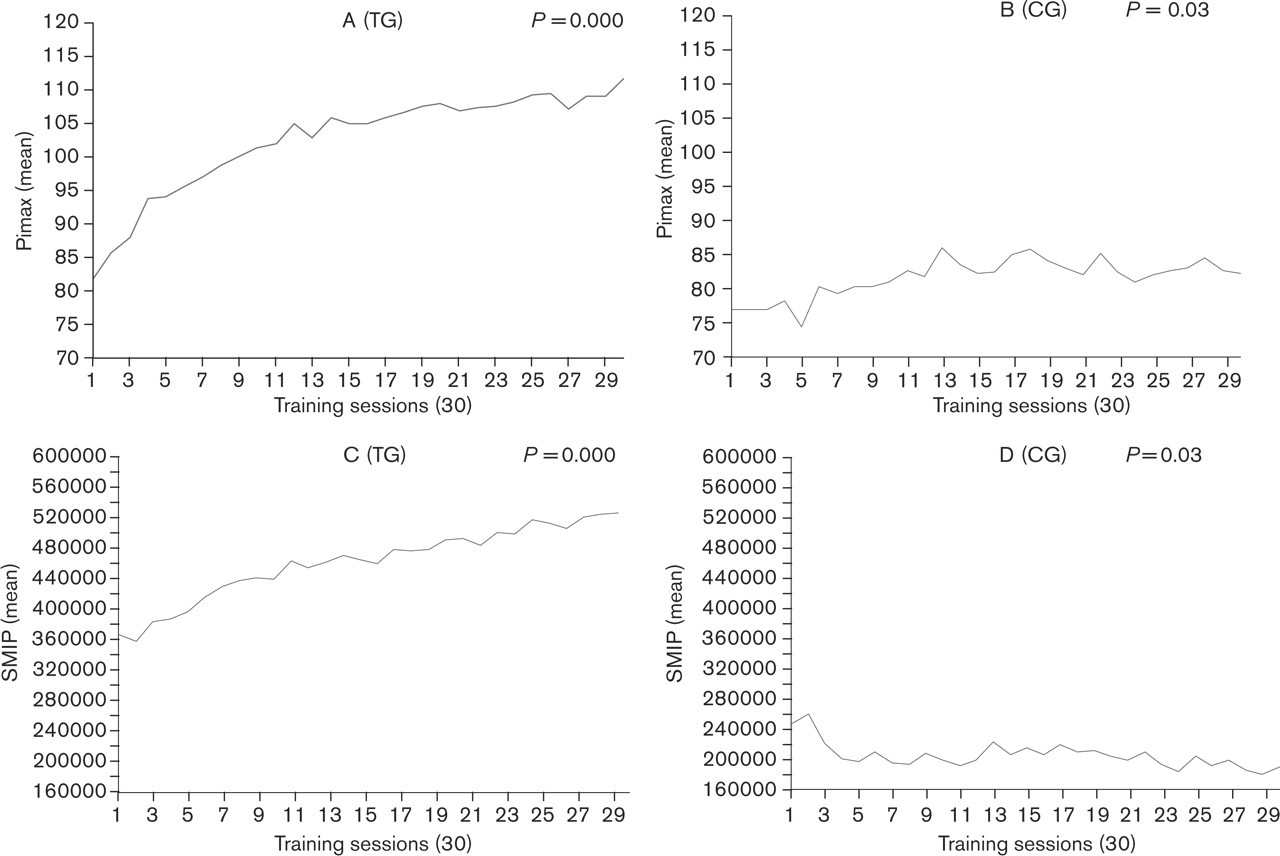
Mean values of Pimax (A, B), and SMIP, (C, D), for the training (TG) and control groups (CG) at each training session. Pimax, maximum inspiratory pressure; SMIP, sustained maximal inspiratory pressure.
The six-minute walk test
Patients in the training group increased significantly the distance covered in the six-minute walk test. In contrast, there was no significant change in the control group. Borg scale rating of perceived dyspnea decreased significantly after the walk only for the training group, (Table 3).
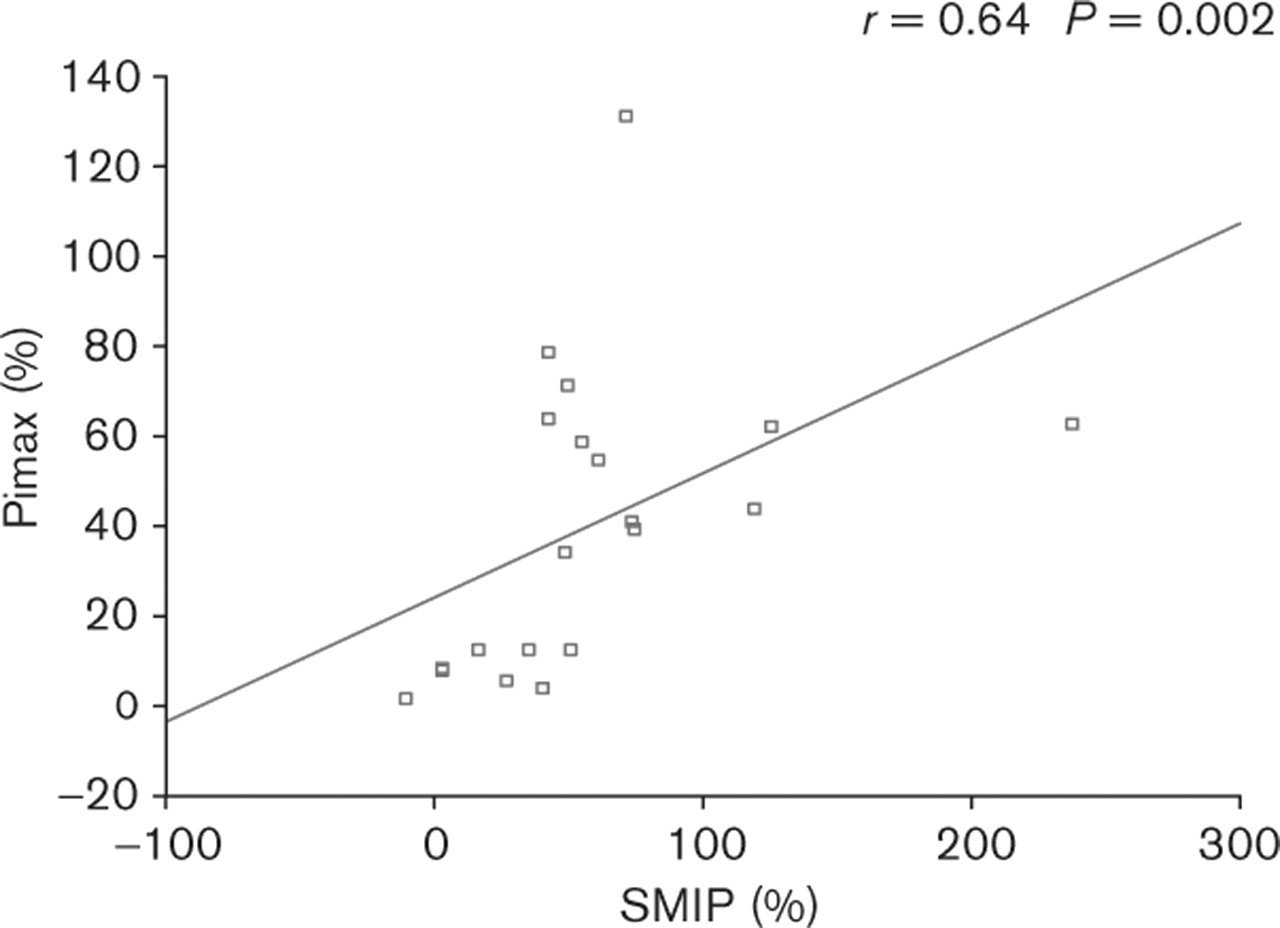
Significant correlation, between percent change of Pimax and SMIP in the training group. Pimax, maximum inspiratory pressure; SMIP, sustained maximal inspiratory pressure.
Echocardiography
No significant change in LVEF or left ventricular diastolic diameter (LVDD) occurred in the training nor in the control groups (Table 4).
Quality of life
A significant improvement in quality of life score was recorded only for the training group, (Fig. 6).
Discussion
This program used skeletal muscle training principles to train the inspiratory muscles throughout respiratory effort. Incremental loading involved reducing the rest intervals between muscle contractions, thus increasing the efficiency of the aerobic response to loading [22]. Patients were exercised at a percentage of their individual inspiratory capacity at each training session. A significant increase in both inspiratory muscle strength and endurance was produced in the training group. More importantly, an improvement in exercise capacity occurred as assessed by peak VO2 during treadmill exercise and the six-minute walk test. Perceived dyspnea was reduced for both maximal and submaximal exercise tests and quality of life was improved with inspiratory muscle training.
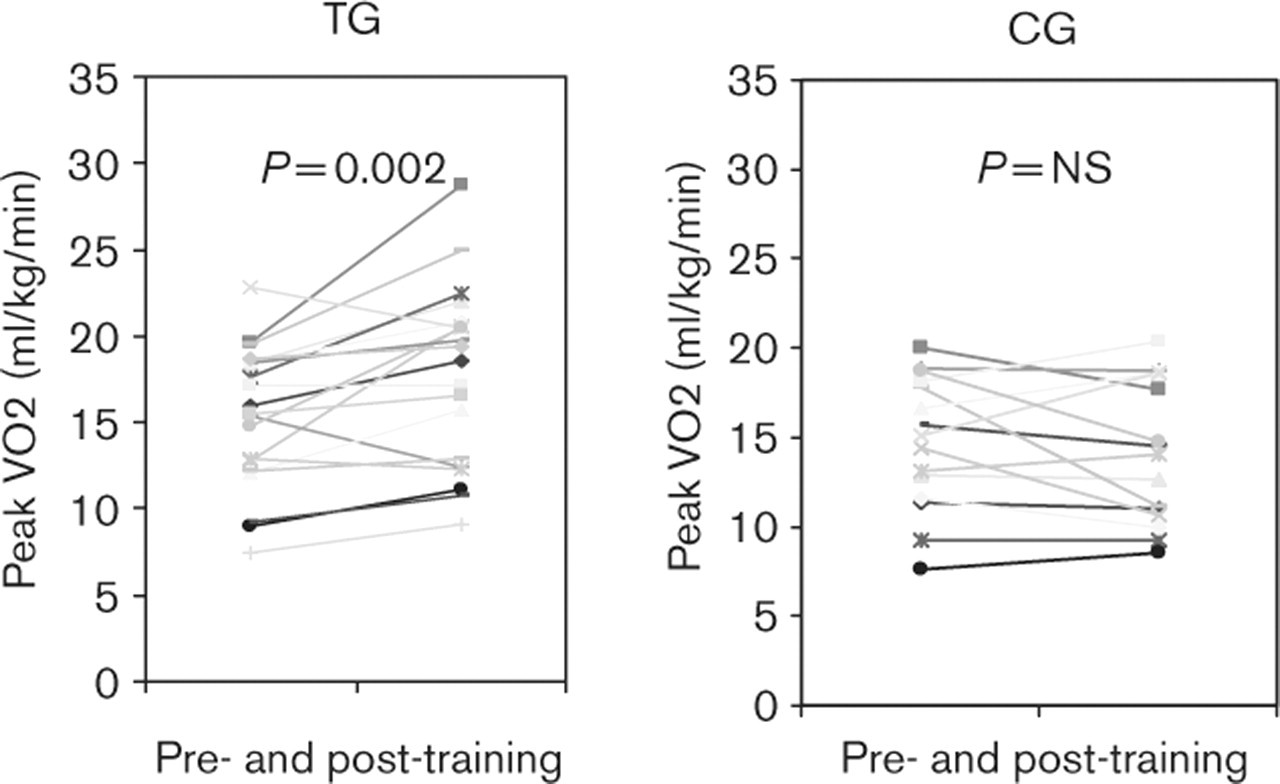
Peak VO2 for individual patients of the training (TG) and control groups (CG), pre- and post-training.
Results of pulmonary function tests for training (TG) and control groups (CG), pre- and post-training
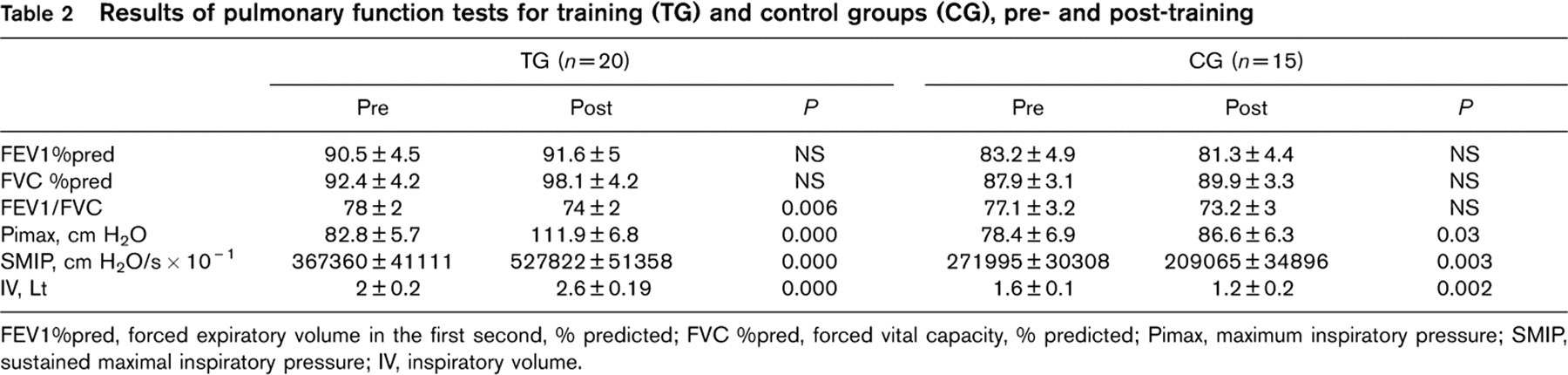
FEV1%pred, forced expiratory volume in the first second, % predicted; FVC %pred, forced vital capacity, % predicted; Pimax, maximum inspiratory pressure; SMIP, sustained maximal inspiratory pressure; IV, inspiratory volume.
Results of exercise testing and dyspnea recordings for training (TG) and control (CG) groups, pre- and post-training
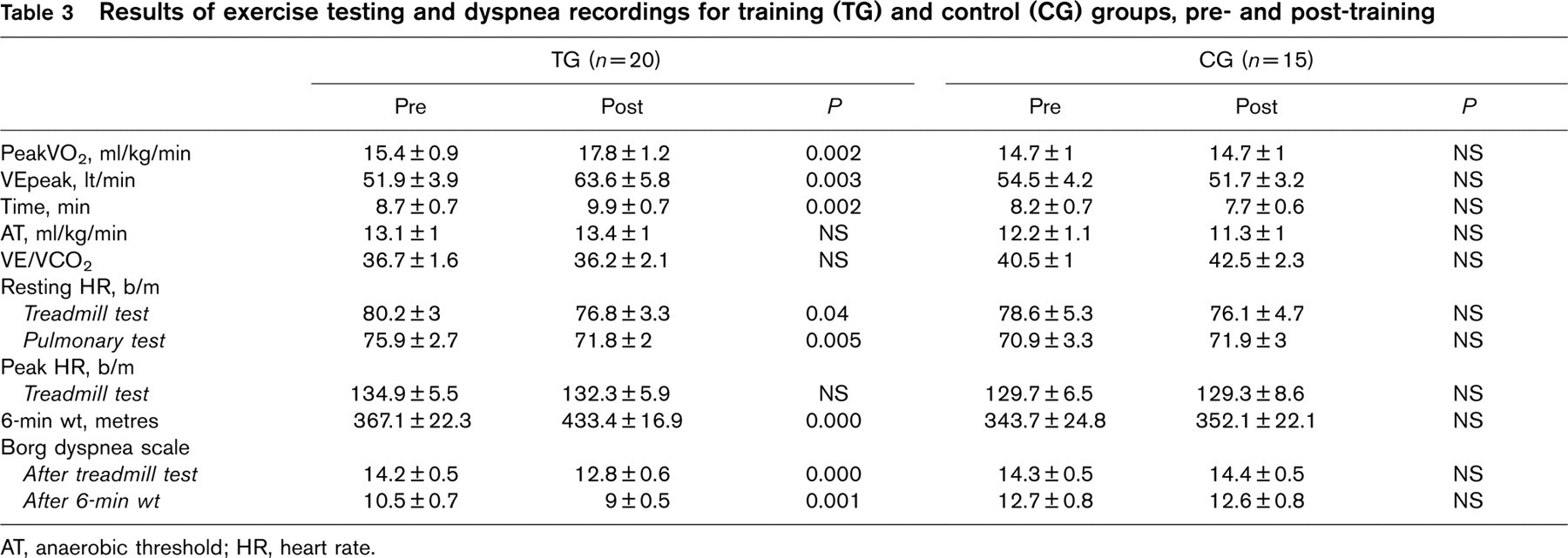
AT, anaerobic threshold; HR, heart rate.
Results of echocardiography for training (TG) and control (CG) groups, pre- and post-training

LVEF, left ventricular ejection fraction; LVDD, left ventricular diastolic diameter.
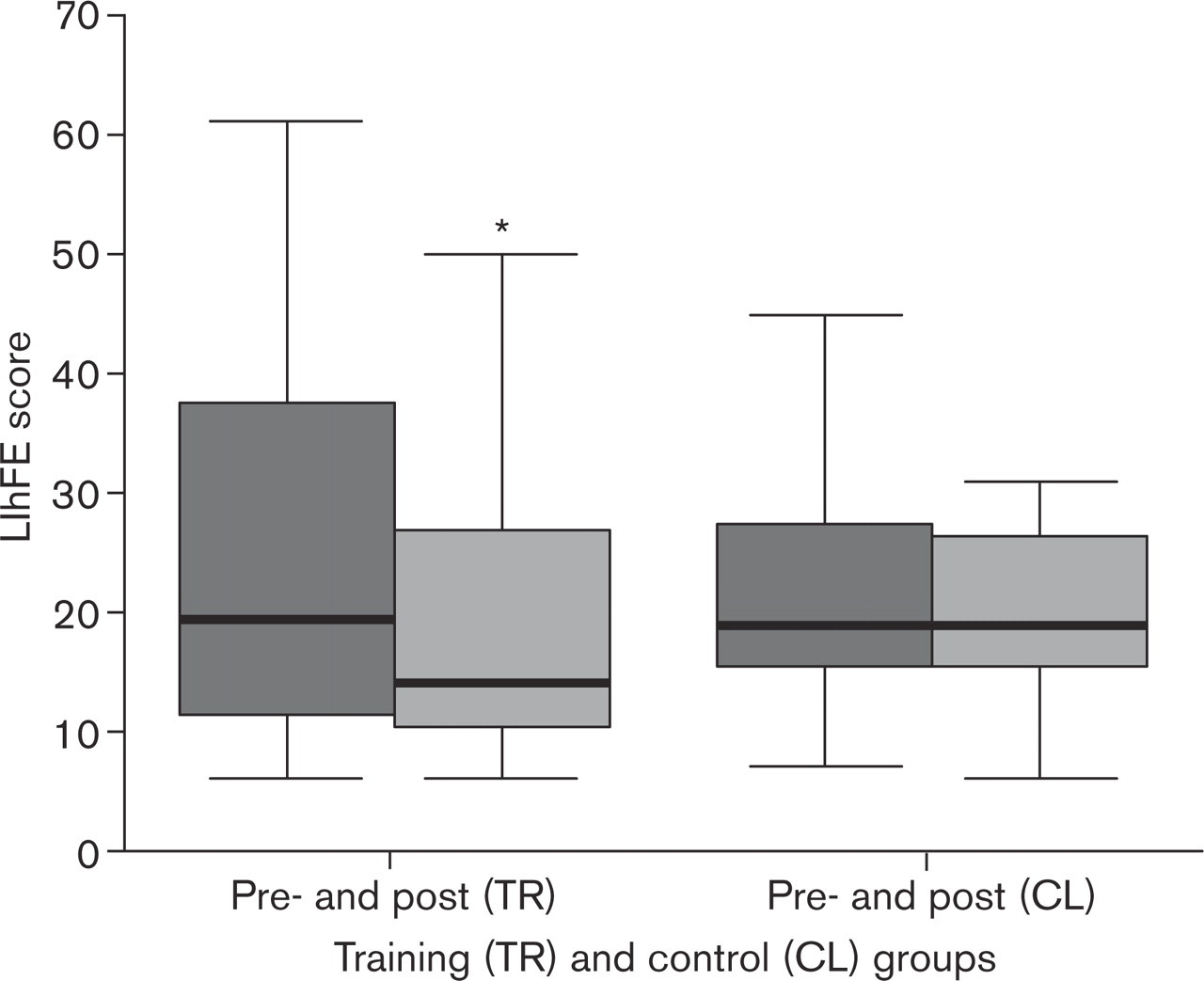
Comparison of Minnesota living with heart failure questionnaire score (LihFE score) in the training (21.1 ± 3.5 vs. 25.2 ± 4, ∗P = 0.004) and control groups (22.6 ± 2.5 vs. 22.9 ± 2.6, P = NS), pre- and post training.
Efficacy of inspiratory training
The significant improvement in both inspiratory muscle strength and endurance and also the correlation between percent change in Pimax and SMIP in the training group demonstrate the efficacy of our training program. A lower intensity inspiratory training program in the control group, showed a smaller increase in inspiratory muscle strength but a decrease in inspiratory endurance. Hence, it is possible that the element of endurance training rather than strength training contributed to the beneficial effects observed in the training group. The improvement in inspiratory muscle function may have achieved respiratory unloading with restoration of the imbalance between the ability of the inspiratory muscles to sustain activity against inspiratory loads. Spirometry and inspiratory lung volume measurements showed a tendency of improvement in lung volumes only in the training group.
Exercise capacity, dyspnea and quality of life
Peak oxygen consumption significantly increased in the training group but not in the control group suggesting that motivational factors did not contribute to this improvement.
Possible mechanisms include a higher consumption of oxygen by the respiratory muscles. However, there was no change in VO2 at anaerobic threshold and a systemic aerobic effect on both respiratory and/or other muscles seems unlikely. Inspiratory muscle training did not influence the ventilatory response to exercise, since the VE/VCO2 did not change. Resting heart rate was significantly reduced and peak heart rate showed a tendency to decrease in the training group, during treadmill testing. Hence, it is possible that a training-induced bradycardia allowed the same workload to be achieved at a lower sympathetic drive, heart rate and myocardial oxygen requirements. Thus, it is possible that reserve exercise capacity was enhanced. These findings may reflect a beneficial feedback between improvements in respiratory function and shifts in autonomic balance from sympathetic to vagal prominence and/or involvement of a diaphragmatic-mediated reflex, which may influence overall sympathetic tone. This new reflex suggested may form the ‘missing link’ between diaphragm and peripheral muscles to explain respiratory-training induced improvements in exercise capacity in CHF. It has recently been demonstrated, that diaphragmatic fatigue in normal subjects was associated with redistribution of blood flow away from the limb muscles to support the newly recruited respiratory muscles, suggesting a ‘steal’ phenomenon by the diaphragm [23, 24]. Sheel and co-workers [25] attributed the observed limb vasoconstriction to a ‘metaboreflex’ originating in the diaphragm, which reaches its threshold for activation during fatiguing contractions and may cause sympatho-excitation with a decrease in peripheral blood flow. Although, we do not have the evidence, we speculate that this reflex may be tonically active in patients with CHF and chronic elevation in the work of breathing. A shift in blood flow distribution from the peripheral muscles to respiratory muscles to support a more active tissue in order to maintain life may be present. This suggestion may explain the increased oxidative capacity of the diaphragm in CHF patients.
Inspiratory muscle training may have modified the threshold of this ‘metaboreflex’ achieving a redistribution of blood flow from respiratory muscles to the limb muscles. This reflex may function in either way. When patients perform whole-body exercise the peripheral muscles increase their circulatory demands first, before reaching diaphragmatic fatigue. This may explain findings by Mancini and co-workers [8, 10] who showed deoxygenation of the accessory muscles of respiration in CHF patients during whole-body exercise, but not during isolated respiratory training.
In addition, Nanas and co-workers [26] observed a sustained decrease in maximal inspiratory pressure and a slower decline in oxygen consumption in patients with CHF who displayed low oxygen consumption at peak exercise. They suggested a decreased recovery of the energy stores of the inspiratory muscles.
Therefore, a modification of the metabolic requirements of the respiratory muscles might have resulted from inspiratory training with a better balance between O2 demands and supply to the respiratory muscles. Consequently, a possible delay in diaphragmatic fatigue with improvement in diaphragmatic ‘metaboreflex’ response may have contributed to a regulation of the overall sympathetic activity and improved exercise capacity in our training group. In previous studies, exercise capacity was also improved by unloading the respiratory muscles with a helium-oxygen mixture, or methoxantine, a vasoconstrictor that may prevent bronchial vasodilatation [27, 28].
Patients in the training group increased their walking distance significantly as measured by the six-minute walk test, which was associated with a decrease in perceived dyspnea. A direct modification of the symptom of dyspnea might have occurred explaining the improvement in both treadmill testing performance and walking distance. This is further enhanced by the increase in exercise time duration during treadmill testing in the training group. The level of perceived dyspnea did not change in the control group who exercised under similar conditions with the training group. Therefore, an adaptation to this symptom in the training group seems unlikely. Decreased inspiratory endurance may be the cause of dyspnea. Mancini and co-workers [11] have previously described a significant correlation between maximal mouth pressures and Borg scale rating of perceived dyspnea, suggesting a cause-and-effect relation between respiratory function and dyspnea. Therefore, the decrease in inspiratory muscle weakness and decreased work of breathing may have modified proprioceptive information affecting the threshold of perceived dyspnea. Receptors originating in the respiratory muscles may contribute to the perception of this symptom. Improvement in quality of life further supports the beneficial effects of inspiratory muscle training in patients with CHF.
Study limitations
A potential limitation of our method is that Pimax and SMIP are measured during the same inspiratory effort. This might suggest a ‘learning effect’ in the control group who increased Pimax and decreased SMIP. Patients may have increased their effort either in strength or endurance measurement. However, this was not observed in the training group. Reduction in resting heart rate in the training group may indicate an influence of inspiratory muscle training on autonomic balance. However, direct measures of autonomic function were not used in this study and further assessment of heart rate variability and sympathetic activity related to diaphragmatic-fatigue may enrich these findings.
Inspiratory muscle training might have also improved right ventricular ejection fraction with a consequent improvement in exercise capacity. Unfortunately, we did not evaluate right ventricular function.
Conclusion
Our study demonstrated a safe and effective way of improving exercise capacity, decreasing dyspnea and improving quality of life in patients with CHF. This was a controlled study with patients in the control group unable to improve their functional status or decrease dyspnea. Therefore, motivating factors or visiting the hospital, were not associated with improvements seen in the training group. All patients enjoyed the training regime employed. Home administration of the device used in the present study could be widely applicable and may be found to have clinical benefits. Moreover, improvement in quality of life with respiratory training may suggest that this modality might well complement the more widely used exercise rehabilitation programs.
Different mechanisms were analysed providing new insights into the pathophysiological contribution of respiratory muscles in CHF. Our findings suggest that respiratory muscles may play a crucial role in beneficially modifying both exercise capacity and symptoms of dyspnea in patients with CHF. Further investigation to highlight the effects of inspiratory muscle training in CHF is needed.
Footnotes
Acknowledgements
We wish to thank the Alexander S. Onassis, Public Benefit Foundation for funding this study and Miss Oanna Ionescou for assistance with the equipment.