
Abstract
Background
Increased arterial stiffness has been found in patients with chronic high-grade inflammatory diseases. Whether mitigation of low-grade systemic inflammation, through a low-cholesterol/low-saturated fat diet, may have a role in improving arterial stiffness is still untested.
Design
We investigated whether variations in blood lipids and plasma C-reactive protein induced by low-cholesterol/low-saturated fat diet are associated with variations in large-artery stiffness in hypercholesterolemia.
Methods
Thirty-five patients with primary hypercholesterolemia and 15 normal control subjects were recruited for the study. Hypercholesterolaemic patients followed an 8-week low-cholesterol/low-saturated fat diet (30% total fat, 5% saturated fat, cholesterol <200mg/daily). Anthropometric characteristics, blood lipids, plasma C-reactive protein and arterial stiffness were measured at baseline and after the diet.
Results
Arterial stiffness and C-reactive protein levels were higher in hypercholesterolaemic patients than in controls. Significant reductions in body weight (2 kg, 3%), plasma total cholesterol (13.4mg/dl, 5.3%), low-density lipoprotein cholesterol (11.2 mg/dl, 6.4%), C-reactive protein (0.7 mg/l, 39%) and arterial stiffness (from 8.9 ± 2.0 to 8.1 ± 1.9 m/s, 11%) were achieved among hypercholesterolaemic patients after the 8-week diet (P < 0.05 for all). Bivariate correlations and multivariate analysis showed reduction in arterial stiffness after short-term diet to be associated with reduction of plasma C-reactive protein levels (r = 0.59, β = 0.38, P<0.05 for both).
Introduction
Arterial stiffness is generally accepted as a predictive factor for cardiovascular morbidity and mortality [1–3, and a prolonged survival has been reported in high-risk patients who achieve a reduction in arterial stiffness [4]. These data suggest the potential role of arterial stiffness as a therapeutic target. An increase in arterial stiffness is associated with a number of cardiovascular risk factors, such as smoking [5], hypertension [6], diabetes [7] and advancing age [8]. The relationship between hypercho-lesterolaemia and arterial stiffness is more controversial, however [9–12. In familial hypercholesterolaemia, arterial stiffness has been found to be higher [9, 10] or lower [11] than in normal control subjects. In addition, a positive relationship between plasma cholesterol levels and arterial stiffness has been described in some [12, 13], but not all [14], studies. Interestingly, Aggoun et al. [15] have shown that stiffness of the carotid wall was increased in children with familial hypercholesterolaemia, independently of plasma total or low-density lipoprotein (LDL) cholesterol levels.
Lipid-lowering intervention studies, aimed at examining the effects of cholesterol reduction on arterial stiffness, have reported contrasting results [16–19. Both increased [16, 17] and reduced [18, 19] arterial stiffness have been found after plasma cholesterol reduction. Whether cholesterol lowering alone, or rather additional features that frequently accompany plasma cholesterol reduction, may be responsible for changes in arterial compliance is still a matter of debate. Hypercholesterolaemia is frequently paralleled by an inflammatory state [20, 21], which in turn has been associated to an impairment of arterial compliance in chronic inflammatory diseases [22, 23], irrespective of plasma lipids and traditional cardiovascular risk factors. In addition, among hypercholesterolaemic patients, hypolipidaemic diet is frequently effective in reducing both plasma cholesterol and markers of inflammation [24, 25].
The purpose of the present study was to evaluate whether potential changes in arterial stiffness in hypercholesterolaemic patients receiving a short-term low-cholesterol/low-saturated fat diet might be explained by the concomitant variations in plasma levels of cholesterol and/or C-reactive protein (CRP), a prototypic marker of systemic inflammation and possibly of cardiovascular risk [26].
Methods
Subjects
The study population consisted of 35 outpatients with primary hypercholesterolaemia recruited from our Lipid Clinic, and of 15 matched normocholesterolaemic control subjects. Diagnosis of hypercholesterolaemia was based on the average of two measurements of serum LDL cholesterol > 4.1 mmol/l. Exclusion criteria were secondary hyperlipidaemia due to diabetes mellitus, renal, liver or thyroid disease, and alcohol consumption of > 40 g/ day. Subjects with known hypertension, history of cardiovascular disease, ultrasonographic evidence of atherosclerotic plaques of the carotid arteries or with any clinical or laboratory evidence of inflammation over a period of ≥ 1 month before the study starting were excluded from the study. None of the participants was a smoker or receiving drug treatment with antiplatelet, anti-inflammatory, or hypolipidaemic agents. All participants gave their informed consent to participate in the study.
Procedures
The determinations were made in the medical centre between 8.00 a.m. and 10.00 a.m. after 12 h fasting, with a room temperature between 21 and 23°C. Weight and height were measured and body mass index (BMI) calculated as well as waist and hip circumferences. Brachial blood pressure was measured by a physician with a mercury sphygmomanometer after patients had sat for 10 min or longer. The average of three measurements was considered for the analysis. After measuring blood pressure, aortic pulse wave velocity (aPWV) was determined with an automatic device, the SphygmoCor Vx system (AtCor, Sydney, Australia), which uses a single-lead ECG and a high-fidelity applanation tonometer to measure the pressure pulse waveform sequentially in two peripheral artery sites, one at the base of the neck for the common carotid artery and the other over the femoral artery. aPWV was calculated from measurements of pulse transit time and the distance between the two sites, according to the following formula:
The numerator is the distance between the suprasternal notch and the femoral artery, minus the distance between the carotid sampling site and the suprasternal notch; the denominator is the time interval between the systolic R wave and the femoral systolic up-stroke minus the time interval between the systolic R wave and the carotid systolic up-stroke. The distance between the two sites was measured using a large compass system, which avoided the measure being influenced by thoracic and abdominal profiles. The average of 10 different cardiac cycles on each of the sites was used for the analysis. All measurements were performed by the same observer. The intra-observer variability measured in 50 healthy young volunteers was 5.1%.
Total cholesterol, triglycerides and high-density lipoprotein cholesterol were determined by the enzymaticcolorimetric method (Dimension Autoanalyzer; DADE Inc. Newark, NJ, USA); LDL cholesterol was calculated by the Friedewald equation [27]. Plasma CRP levels were measured using the Latex-Enhanced CRP assay (Dade Behring High Sensitivity CRP Assay, Marburg, Germany) on the same nephelometer.
A low-cholesterol/low-saturated fat diet, to be followed for 8 weeks under isoenergetic conditions, was recommended to all hypercholesterolaemic patients. Briefly, we recommended to all hypercholesterolaemic patients a reduced intake of total fat (30% of total calories), saturated fat (5% of total calories), and cholesterol (< 200 mg/day) [28]. The diet was individually tailored to meet each person's energy requirement. In order to allow subjects to vary their choice and thereby improve their compliance to diet, the participants were allowed to choose a limited number of food items, free of fat and cholesterol, that provided 5% of the total daily energy intake. The subjects were instructed to maintain their habitual pattern of physical activity for the duration of the study. They were also asked to record in a diary deviations from the diet, medications used, free-food choice, and changes in activity patterns. Compliance with the diet was checked by a trained dietician by means of interviews, checking the diary, and measuring body weight every week.
Hypercholesterolaemic patients underwent a second visit after the 8-week diet regimen, during which clinical examination, blood sampling and aPWV assessment were repeated.
Statistical analysis
SPSS statistical package, release 8.0 (SPSS Inc, Chicago, IL, USA) was used for all statistical analyses. Values are expressed as the mean ± SD. CRP and triglycerides were logarithmically transformed for statistical testing to improve their skewness, and the distribution of the residuals from the fitted models became normally distributed after log transformation. Student's t-test was performed to compare continuous variables between hypercholesterolaemic patients and normal control subjects. A paired two-tailed t-test was performed to assess the effects of the 8-week low-cholesterol/low-saturated fat diet on study variables. Variations of the study variables (D) after the diet were calculated as the difference between values at the end of the diet and those at baseline. Pearson's and Spearman's correlation analyses were performed between baseline variables as well as between variations of the study variables after the 8-week diet programme. Stepwise linear regression analysis was used to estimate prediction of ΔaPWV by including simultaneously in the model those variables that changed significantly after the 8-week low-cholesterol/low-saturated fat diet, as well as blood pressure and heart rate variations.
Results
Thirty-five subjects with primary hypercholesterolaemia and 15 matched normocholesterolaemic subjects were entered into the study. Clinical characteristics of hypercholesterolaemic and normocholesterolaemic subjects are summarized in Table 1. No significant difference was found between the two groups in terms of age, indices of adiposity, blood pressure values, and heart rate. By definition, total and LDL cholesterol values were significantly higher in the hypercholesterolaemic than in the normocholesterolaemic patients group (P < 0.001 for both comparisons). Plasma CRP levels as well as aPWV were significantly higher in hypercholesterolaemic patients than in normocholesterolaemic subjects (P < 0.05 for both comparisons). aPWV had significant correlations with indices of adiposity (r = 0.35, P = 0.04 for BMI; r = 0.35, P = 0.04 for waist circumference), systolic (r = 0.34, P = 0.02) and diastolic (r = 0.30, P = 0.05) blood pressures, CRP (r = 0.44, P = 0.008) and LDL cholesterol (r = 0.32, P = 0.051).
Table 1 reports results, among hypercholesterolaemic patients, of an 8-week low-cholesterol/low-saturated fat diet on the study variables. A mild significant reduction in BMI after the low-fat diet was paralleled by a slight decrease of plasma total and LDL cholesterol concentrations and of plasma CRP levels as well. A significant 11% decrease of aPWV was also found. A slight but not significant reduction in blood pressure values was observed (Table 1). To minimize the effect of time-related variations in BMI, cholesterol, CRP and aPWV, analysis of covariance with baseline measurements included as covariate was performed. The analysis still showed those variables changing significantly after the 8-week diet period.
Figure 1 shows correlations, among hypercholesterolaemic patients, between diet-induced variations in aPWV on the one hand, and plasma CRP, total cholesterol and LDL cholesterol on the other. ΔaPWV was significantly correlated with ΔCRP (r = 0.59, P <0.001), but not with Δtotal cholesterol (r = 0.15, 0.39) or ΔLDL cholesterol (r = 0.04, 0.78). Multivariate analysis in hypercholesterolaemic patients was performed including ΔaPWV as dependent variable and the ‘Δ’ of those variables that changed significantly after the 8-week diet as independent variables, named Δtotal cholesterol, ΔLDL cholesterol, ΔBMI and ΔCRP. The multivariate model confirmed ΔCRP as the only significant predictor of ΔaPWV (Table 2), even when Δheart rate and either Δsystolic blood pressure, Δdiastolic blood pressure, or both were included in the analysis.
Clinical and biological characteristics of 15 normocholesterolaemic subjects and of 35 hypercholesterolaemic patients before and after cholesterol-lowering diet
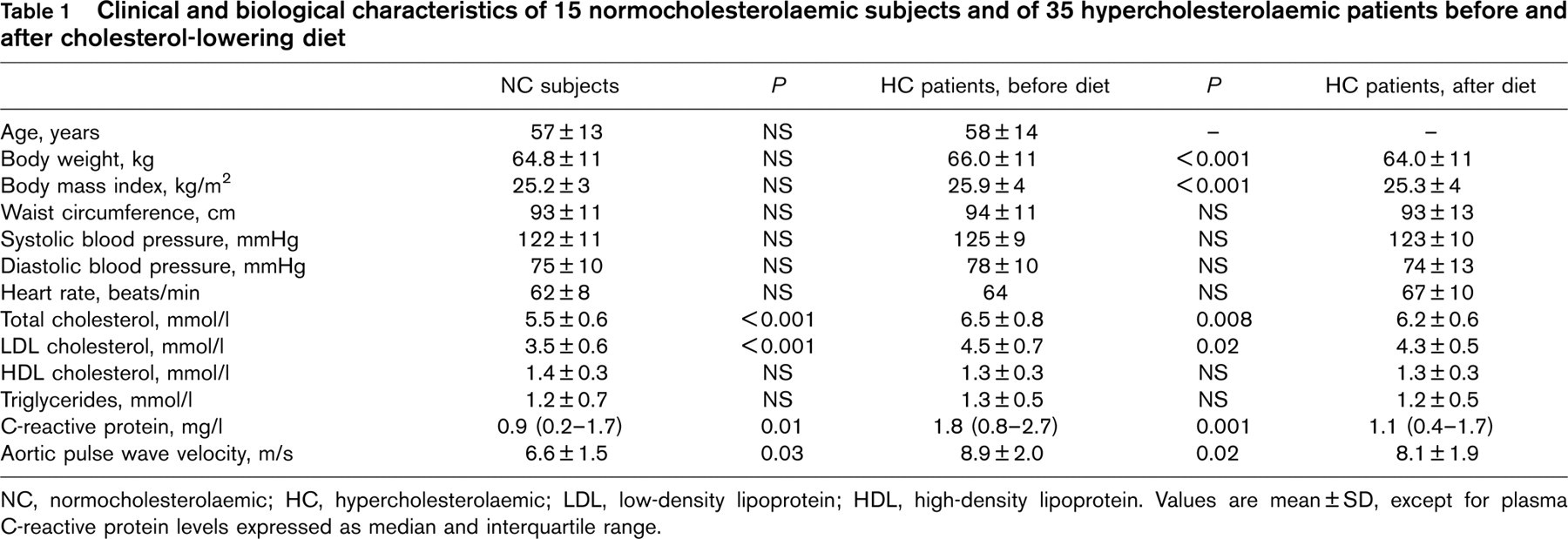
NC, normocholesterolaemic; HC, hypercholesterolaemic; LDL, low-density lipoprotein; HDL, high-density lipoprotein. Values are mean ± SD, except for plasma C-reactive protein levels expressed as median and interquartile range.
Multiple linear regression analysis in hypercholesterolaemic patients with ΔaPWV as a dependent variable
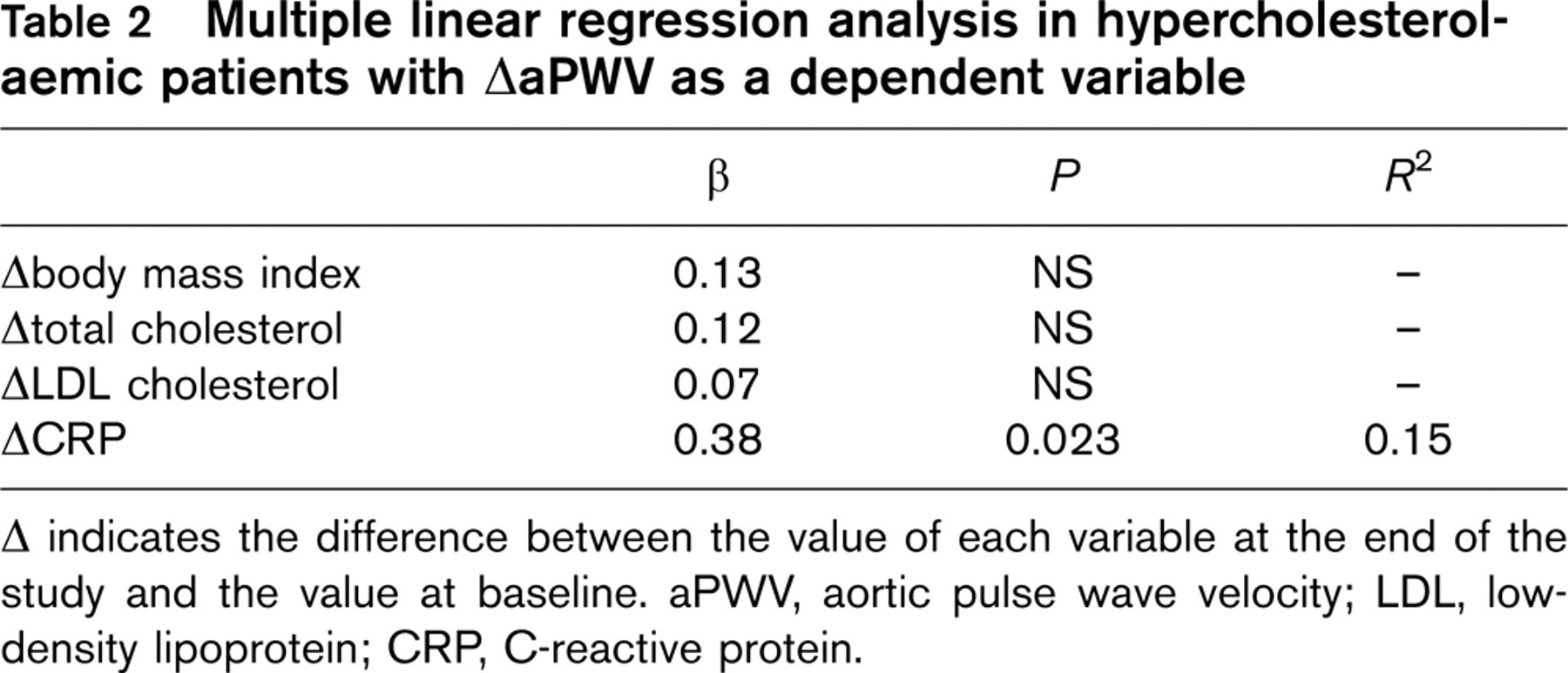
Δ indicates the difference between the value of each variable at the end of the study and the value at baseline. aPWV, aortic pulse wave velocity; LDL, low-density lipoprotein; CRP, C-reactive protein.
Discussion
In the present study, a short-term low-cholesterol/low-saturated fat diet resulted in an improved large-artery compliance and produced significant decreases in plasma cholesterol and CRP concentrations in patients with hypercholesterolaemia. These benefits were observed in the absence of other interventions that have been shown to improve large artery stiffness, named lipid-lowering [16–19 and/or anti-hypertensive drugs [29]. Moreover, we demonstrated that the amelioration in large artery stiffness among hypercholesterolaemic patients was predicted by plasma CRP reduction after the diet, rather than by mild reduction of plasma cholesterol levels.
By contrast, clinical studies support the intuitive hypothesis that high cholesterol levels should stiffen large artery wall [9–15. Some studies found that patients with hypercholesterolaemia have stiffer blood vessels than in matched controls [9, 10], and that intensive and prolonged cholesterol reduction may have a role in reducing large artery stiffness [18, 19]. However, other authors reported an increased aortic distensibility in subjects with heterozygous familial hypercholesterolaemia [11], an inverse association between cholesterol and aortic stiffness [14], as well as increased arterial stiffness after cholesterol-lowering therapy [16, 17]. In the present study mild cholesterol lowering (5.3 %) does not seem to play an immediate role in reducing arterial stiffness in hypercholesterolaemic patients; other covariates of arterial stiffness, namely increased plasma CRP concentration, might play this role. Accordingly, using multivariate analysis, a 39% reduction of plasma CRP levels after the 8-week diet programme was the only predictor of the improvement of large artery stiffness, irrespective of other parameters that changed after the short-term low-cholesterol/low-saturated diet.
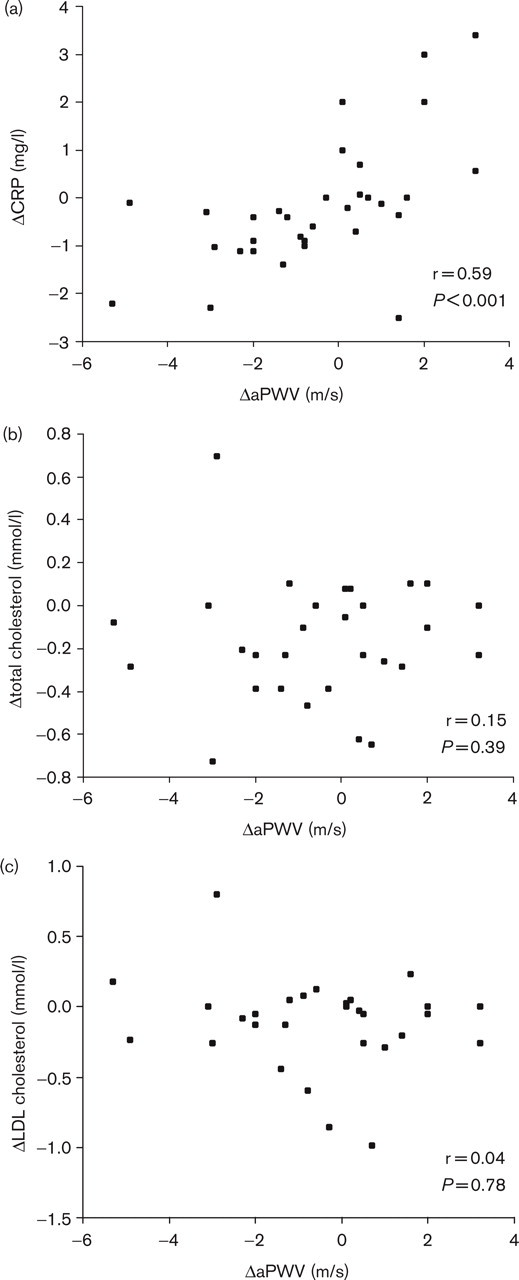
Spearman's correlation analysis between ΔCRP and ΔaPWV (panel a). Pearson's correlation analyses between Δtotal cholesterol, ΔLDL cholesterol and ΔaPWV (panels b and c). D indicates the difference between the value of each variable at the end of the diet and the value at baseline.
Evidence that adipose tissue is a source of pro-inflammatory cytokines [30], which in turn stimulates liver CRP synthesis [31], is undisputed. The efficacy of weight loss to mitigate low-grade systemic inflammation has also been reported [32, 33]. On this basis, the slight but significant diet-induced weight loss, observed in the present study, might have favoured a reduced release of pro-inflammatory cytokines by adipose tissue, thus mitigating the low-grade systemic inflammation state that we found at baseline in hypercholesterolaemic patients as compared with the normocholesterolaemic subjects. However, a direct anti-inflammatory effect of a low-fat diet should be considered.
Attenuation of systemic inflammation might have been responsible for the improvement in large artery stiffness that hypercholesterolaemic patients experienced in the present study after the low-cholesterol/low-saturated fat diet. The latter conclusion is supported by an increasing number of studies showing that patients with chronic inflammatory diseases, as for instance rheumatoid arthritis and systemic lupus erythematosus, have stiffer arteries compared with healthy controls, irrespective of plasma cholesterol levels [22, 23]. Wong et al. found that plasma CRP concentration is also an important direct covariate of arterial rigidity [22]. In addition, we recently found that plasma CRP concentration is independently associated in hypertensives to pulse pressure[34], an indirect measure of increased arterial stiffness, as well as to aortic pulse wave velocity in hypercholesterolaemic patients [35]. Localization of plasma CRP in vessel walls, CRP binding of neutrophils, interaction with adhesion molecules, complement activation, are conditions that all together might act synergistically in a pro-inflammatory and arterial stiffening manner.
Finally, inflammation is associated with impaired endothelial function [36]. It is possible that impaired endothelial function, which has been shown to participate in modulating the intrinsic elastic properties of the arteries through smooth muscle cell relaxation-contraction [37], could be the link between inflammation and artery stiffness.
In the present study the diet intervention was not controlled in parallel groups, being hypercholesterolaemic patients assigned to the intervention but not to placebo. Thus, regression toward the mean, as well as intraobserver measurement variability, might have influenced the observed variations in aPWV and other variables. Repeated measures of aPWV (see Procedures) and analysis of covariance with the baseline measurement of BMI, cholesterol, CRP and aPWV included as covariates should have minimized time-related variations of these variables. In addition, the low intra-observer aPWV measurement variability should have reduced the observed variations in aPWV.
Irrespective of the mechanisms underlying the arterial stiffness reduction observed in our study, the present results encourage low-cholesterol/low-saturated fat consumption as a successful first-line approach to attenuate low-grade systemic inflammation and to improve the compliance of large arteries. However, looking at only cholesterol reduction as a measure of the efficacy of a short-term lipid-lowering therapy might not be sufficient to predict an amelioration of the status of the large arteries.