
Abstract
Objective Recent experimental and clinical data indicate that abnormal inflammatory and apoptotic processes contribute to the progression of chronic heart failure (CHF). We sought to study the effects of growth hormone (GH) on circulating soluble apoptosis mediators, and to investigate whether these GH-induced anti-apoptotic effects are associated with the reduction of left ventricular (LV) volumes and attenuation of exercise intolerance in idiopathic dilated cardiomyopathy (IDC) patients.
Methods Plasma tumour necrosis factor-α (TNF-α), its soluble receptors sTNFRI and sTNFRII, and plasma apoptosis mediators soluble Fas (sFas) and sFas Ligand (sFAsL) were measured (enzyme-linked immunosorbent assay) in 12 IDC patients (NYHA III; LVEF: 24±2%) before and after a 3-month subcutaneous administration of GH 4IU every other day (randomized, crossover design). Peak oxygen uptake (VO2max), as well as LV volume indices, wall thickness, and endsystolic wall stress (ESWS) were also determined at the same period.
Results Treatment with GH produced a significant reduction in plasma TNF-α (7.8±1.1 versus 5.5±0.9 pg/ml, P<0.02), sTNFRI (4.0±0.4 versus 3.3±0.3 ng/ml, P<0.05), sTNFRII (2.8±0.3 versus 2.4±0.2 ng/ml, P<0.05), sFas (4.7±0.7 versus 3.3±0.5 ng/ml, P<0.05) and sFasL (33.5±9.7 versus 20.2±6.2 pg/ml, P<0.01). A significant reduction in ESWS (841±62 versus 634±48 g/cm2, P<0.01), LV end-systolic volume index (LVESVI, 128±12 versus 102±12 ml/m2, P<0.001) and LV end-diastolic volume index (LVEDVI, 228±16 versus 200±18ml/m2, P<0.01) as well as a significant increase in VO2max (15.3±0.7versus 17.1±0.9 ml/kg per min, P<0.01) were also observed in the patient population after GH administration. Significant correlations were found between the GH-induced decrease of sTNFRII and sFasL and respective reduction of LVESVI.
Conclusion Growth hormone administration reduces circulating TNF system and soluble apoptosis mediators in patients with IDC. These GH-induced anti-apoptotic effects may be associated with the improvement in exercise capacity as well as with the reverse of LV remodelling in patients with CHF and IDC. Eur J Cardiovasc Prev Rehabil 12: 164–168 © 2005 The European Society of Cardiology
Introduction
Growth hormone administration has been considered as a possible treatment for heart failure and has been shown to improve left ventricular (LV) contractility and geometry in rats with experimental heart failure [1–3]. Furthermore, small clinical studies have demonstrated the beneficial effects of human recombinant growth hormone on clinical performance and exercise tolerance in patients with idiopathic dilated cardiomyopathy and chronic heart failure [4–6]. Recently, we found [7] that 3-month growth hormone treatment attenuates abnormal peripheral immune responses in patients with dilated cardiomyopathy leading to a decrease of LV wall stress and cardiac volumes. However, there are no in vivo data about the relationship of growth hormone-induced improvement in LV geometry in these patients and respective modulation of representative soluble apoptosis markers such as tumour necrosis factor-α (TNF)/TNF receptors and Fas/Fas Ligand systems. In this study, we investigated the anti-apoptotic properties of growth hormone, as well as their correlations with the drug-induced reverse cardiac remodelling and improvement of exercise capacity in dilated cardiomyopathy patients.
Methods
Study design
The study population consisted of 12 patients with idiopathic dilated cardiomyopathy, who were classified as New York Heart Association functional class III and had a mean LV ejection fraction 24±2%. Diagnosis of idiopathic dilated cardiomyopathy was based on clinical history, normal coronary arteriography, and histological findings of endomyocardial biopsy. All patients were being treated with angiotensin-converting enzyme inhibitors and diuretics. Some patients were also received beta-blockers, aldosterone antagonists, digoxin and anticoagulants. Exclusion criteria were infections, malignancies, thyroid or other endocrine disease, chronic obstructive pulmonary disease, hepatic or renal impairment, and use of drugs influencing immunoreactivity. The Institutional Ethics Committee approved the study, and each patient gave written consent.
In this randomized crossover study, six patients sub-cutaneously received 4 IU recombinant human growth hormone (Genotropin, Pharmacia Corporation, Sweden) every other day for 3 months (with growth hormone period) followed by another 3 months without growth hormone therapy, whereas the remaining six patients continued their conventional treatment for 3 months (without growth hormone period) followed by another 12 weeks of growth hormone therapy. Other medications remained unchanged throughout the two phases of the study.
Laboratory measurements
Exercise capacity of heart failure patients was evaluated using the cardiorespiratory stress test (Medical Graphics Corp., St Paul, Minnesota, USA) measuring peak oxygen uptake (VO2max, ml/kg per min) in the two periods of the study. Additionally, LV dimensions, volumes, wall thickness, mass index, ejection fraction, and end-systolic wall stress were determined by echocardiography [8].
Plasma samples were assayed in duplicate for TNF-α, soluble TNF receptor I, soluble TNF receptor II, soluble Fas and soluble Fas Ligand concentrations using commercially available enzyme-linked immunosorbant assay kits (Ramp;D systems Inc., Minneapolis, Minnesota, USA for TNF-α, its soluble receptors and soluble Fas; Diaclone Research, Besancon, France, for soluble Fas Ligand). The intra-assay and inter-assay coefficients of variation were < 8% for all enzyme-linked immunosorbent assays in our laboratory. All laboratory tests were performed before daily medication had been taken and were conducted by staff who were blinded to the treatment status of the individual subjects. Demographic and clinical characteristics as well as medications of heart failure patients at initiation of the study are summarized in Table 1.
Demographics, clinical characteristics and medications of dilated cardiomyopathy patients at baseline (mean±SEM)
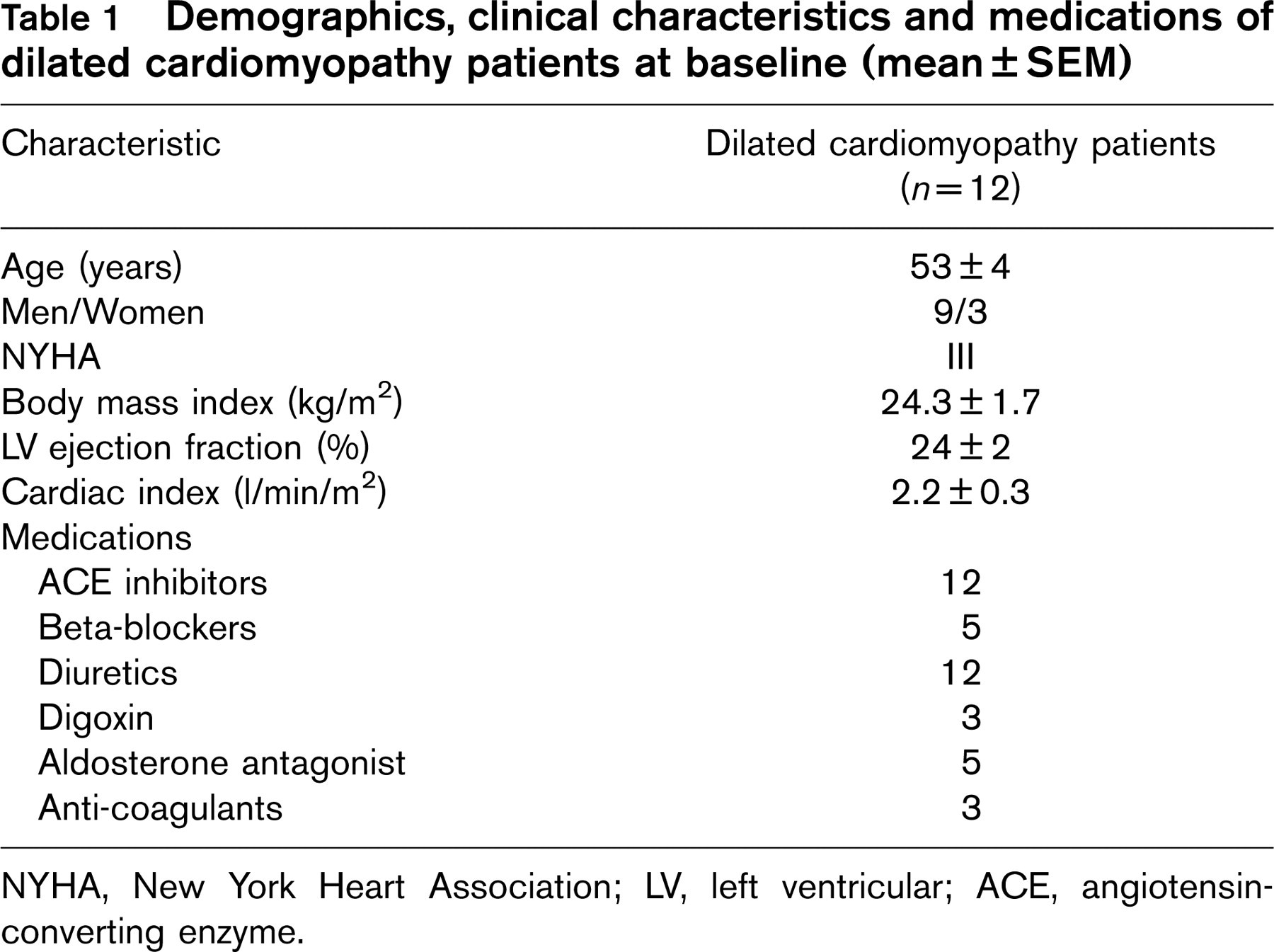
NYHA, New York Heart Association; LV, left ventricular; ACE, angiotensin-converting enzyme.
Statistical analysis
The trial was analyzed according to the recommendations of Hills and Armitage for crossover trials [9]. Simple regression analysis was used to examine the relationship between the growth hormone-induced changes in soluble apoptosis markers and VO2max or wall stress and echocardiographic indices of cardiac remodelling. All values are given as mean±SE (standard error), and a P-value < 0.05 was considered statistically significant.
Results
Table 2 describes echocardiographic variables (LV volumes, ejection fraction and wall stress), soluble apoptosis markers and peak oxygen uptake (VO2max) in the two phases of the study. Compared to the without growth hormone treatment period, drug administration causes a significant reduction in plasma levels of TNF-α (P < 0.01), its soluble receptors TNF receptor I and II (both P < 0.05), soluble Fas (P < 0.05) and soluble Fas Ligand (P < 0.01) (Table 2). Exercise capacity of heart failure patients, expressed by VO2max, was also improved with the 3-month growth hormone treatment (P < 0.01) (Table 2). Additionally, LV end-diastolic (P < 0.001) and end-systolic volume (P < 0.01) indices (ml/m2), as well as end-systolic wall stress (P < 0.01) were significantly decreased (Table 2).
Effects of growth hormone (GH) therapy on soluble apoptosis mediators, peak oxygen uptake, and echocardiographic variables reflecting left ventricular wall stress and remodelling
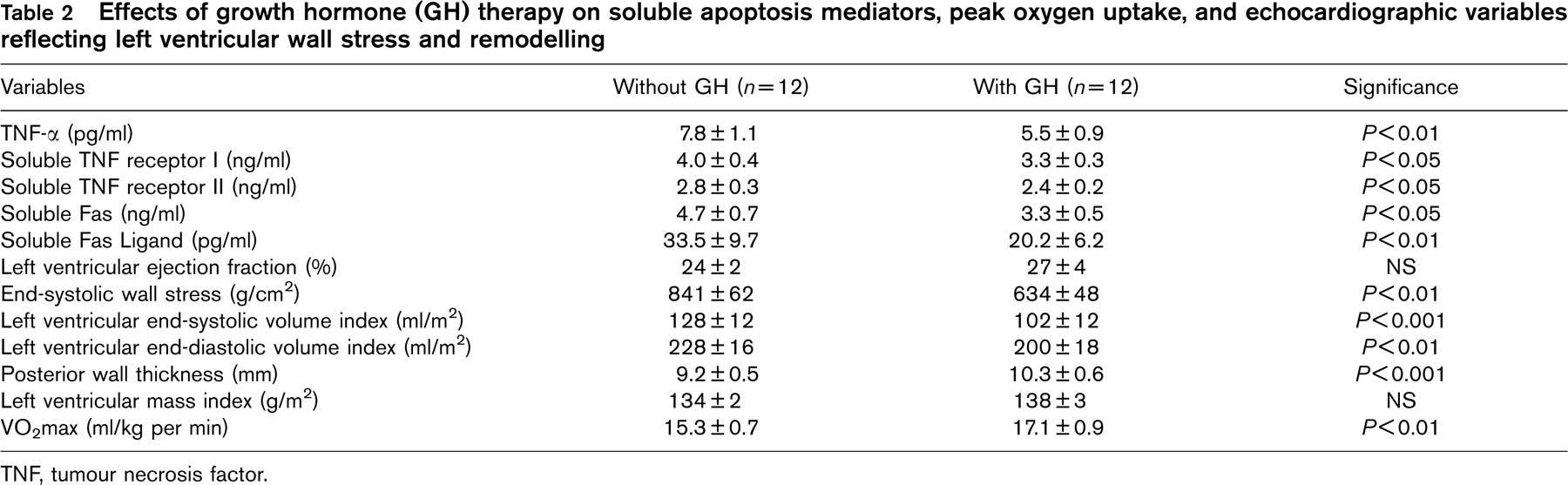
TNF, tumour necrosis factor.
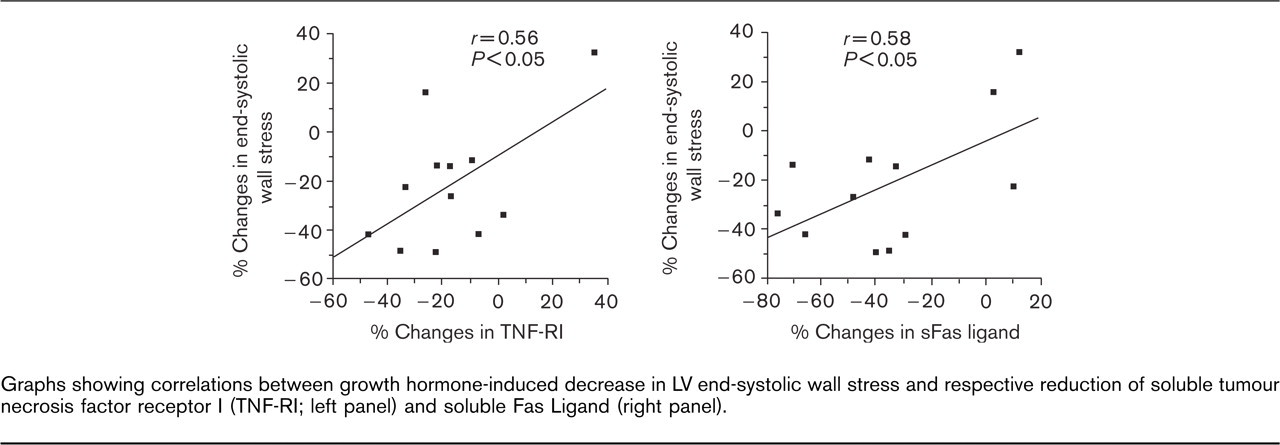
Graphs showing correlations between growth hormone-induced decrease in LV end-systolic wall stress and respective reduction of soluble tumour necrosis factor receptor I (TNF-RI; left panel) and soluble Fas Ligand (right panel).
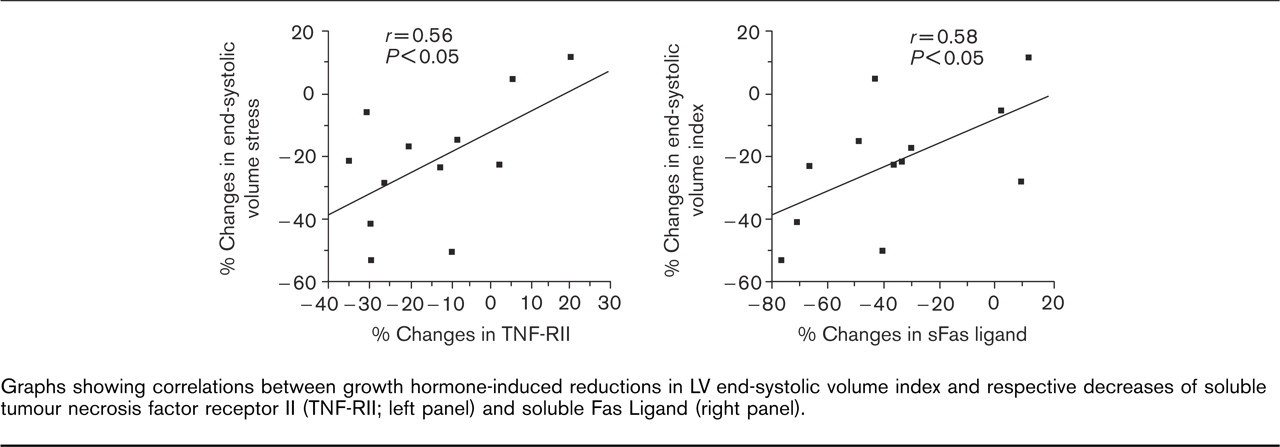
Graphs showing correlations between growth hormone-induced reductions in LV end-systolic volume index and respective decreases of soluble tumour necrosis factor receptor II (TNF-RII; left panel) and soluble Fas Ligand (right panel).
Growth hormone-induced increase in VO2max was significantly correlated with respective decrease of circulating TNF-α (r = −0.62, P < 0.05), soluble TNF receptor II (r = −0.59, P < 0.5) and soluble Fas Ligand (r = −0.66, P < 0.01), as well as the reduction of LV end-systolic volume index (r = −0.55, P < 0.05). Significant correlations were also found between reductions of soluble TNF receptor I and Fas Ligand and respective decreases of end-systolic wall stress (Fig. 1). Finally, GH-induced reduction in LV end-systolic volume index was significantly correlated with decease of soluble TNF receptor II, and Fas Ligand (Fig. 2) Growth hormone treatment was safe and without serious side effects.
Discussion
Pro-inflammatory cytokine over-expression and subsequent excessive activation of cardiomyocyte apoptosis signalling pathways are essential parameters of heart failure progression, leading to maladaptive LV remodelling [10–12]. In previous reports, we have demonstrated that growth hormone administration induces a significant down-regulation of circulating pro-inflammatory cytokines and soluble signalling molecules Fas and Fas Ligand, which are actively implicated in the pathophysiology of the apoptotic process into the cardiovascular system [7, 13]. In this study, we showed for the first time that beneficial modulation of major apoptotic signalling pathways such as soluble TNF and Fas/Fas Ligand systems by growth hormone, are strongly related with improvement of LV geometry, reduction of cardiac wall stress, and increase of exercise capacity in patients with chronic heart failure.
There is growing evidence underlining the prognostic significance of the enhanced levels of soluble TNF receptors (especially type II) in chronic heart failure [14]. It has been also reported that the increase in circulating TNF-α in patients with heart failure was associated with a substantial decrease in myocardial TNF receptors and an increase in their soluble forms [15]. Growth hormone by virtue of its anti-inflammatory and anti-apoptotic effects may lead to down-regulation of myocardial TNF-α expression and up-regulation of tissue TNF receptors, offering a potential explanation of the drug-induced reduction in soluble TNF receptor levels as well as the attenuation of cytokine cardiac spill over into circulation.
The circulating soluble Fas/Fas Ligand system is a major apoptosis signalling pathway that is up-regulated in patients with dilated cardiomyopathy in proportion to the severity of heart failure, and it may provide important prognostic information, and be correlated with T-lymphocyte activation and abnormal intracellular calcium homeostasis in the failing hearts [12, 16, 17]. Growth hormone down-regulates the soluble Fas/Fas Ligand system and resets homoeostasis of cardiomyocyte death at a lower level, possibly through the restoration of intracellular calcium abnormalities, up-regulation of anti-apoptotic gene (i.e., Bcl-2) expression, and stimulation of cardiomyocyte growth signalling pathways [1, 18, 19]. In addition to the potential calcium homeostasis-related direct effects of growth hormone on cardiomyocyte apoptosis, this drug may inhibit an important stimulus for cardiac cytokine and apoptosis mediator production through the decrease of cardiac wall stress. Down-regulation of these apoptosis inducers was also associated with reduction of cardiac volumes and improvement in functional status of heart failure patients, indicating that growth hormone may exert its beneficial effects by suppressing pro-inflammatory cytokine and apoptotic mediator activation characterizing maladaptive cardiac remodelling and clinical deterioration of heart failure. This is in keeping with recent experimental data [20] showing that in a dog model of heart failure induced by rapid ventricular pacing, treatment with growth hormone analogue insulin-like growth factor-1 partially prevented cardiomyocyte apoptosis and attenuated LV remodelling and dysfunction. Dalla Libera et al. [21] found similar results in peripheral muscles of rats with experimental heart failure, showing that GH administration causes decrease of apoptotic nuclei, attenuation of muscle atrophy and significant reduction of serum TNF-α levels. These findings were significantly correlated with better exercise capacity of treated rats, as well as with the down-regulation of apoptotic intracellular enzymes (caspases) and pro-apoptotic genes (bax) [21].
Although large clinical studies are needed in order to investigate the long-term effects of growth hormone on cardiac remodelling and survival rate of patients with dilated cardiomyopathy and heart failure, this kind of treatment may be a promising therapeutic approach through the modulation of major cellular signalling pathways regulating pathophysiological events of progressive cardiac remodelling and peripheral muscle atrophy [22].
Conclusion
This randomized, crossover trial investigated the effects of a 3-month growth hormone administration on peripheral apoptosis inducers such as circulating TNF and soluble Fas/soluble Fas Ligand systems, and left ventricular volumes in patients with chronic heart failure secondary to idiopathic dilated cardiomyopathy. Growth hormone-induced down-regulation of soluble apoptosis mediators was associated with the reduction of cardiac volumes/wall stress and improvement of exercise tolerance, indicating that beneficial effects of growth hormone on left ventricular geometry and clinical performance of chronic heart failure patients may be (at least partially) due to its anti-apoptotic properties.