
Abstract
Background
Data on the recent evolution in coronary heart disease (CHD) mortality and incidence rates are lacking in France. This paper aims to investigate whether the declining trends observed from 1985–1993 still persist in the second half of the 1990s.
Methods
Population registers of acute CHD have been implemented in three specific geographical areas, first as part of the MONICA Project (1985–1993) and, since 1997, according to a simplified registration procedure. Weighted Poisson regressions have been used to investigate time trends in CHD events in men and women aged 35–64 after correction for registration differences.
Results
Data obtained from 1997–2000 showed that the north-to-south gradient of decreasing frequency of CHD events in France was still present. Besides, they revealed no specific trend in CHD morbidity by centre and gender, except in Lille (in the north of France) where events tended to increase in women. Coronary heart disease mortality rates in recent years were decreasing in men, particularly in the north and east of France, but were stable in women with, even, a rising tendency in the north.
Conclusion
The decreasing trend in CHD events in France observed from the mid 1980s to the early 1990s seemed to markedly slow down in the second half of the 1990s.
Introduction
From 1985–1993, three French registers covering regions at contrasting risk of coronary heart disease (CHD) mortality participated in the WHO-MONICA Project [1], using precise definitions of coronary events and standardized criteria [2, 3]. In most northern and western European countries, CHD mortality rates substantially decreased until the early 1990s, particularly in those with high CHD mortality rates [4], thanks to an improvement in acute coronary care and a reduction of CHD incidence [5, 6]. For France, a north-to-south gradient in CHD rates was highlighted. A decrease in coronary events over 10 years was observed, especially in Strasbourg. The reduction in CHD mortality rates was also quite sizeable in Toulouse and Strasbourg, but modest in Lille [4, 7]. If in some countries the decreasing trend seems to be persisting, we have no information about the recent evolution in France, a country with rather low CHD mortality rates.
In this work, we estimated geographical variations of coronary event rates in the second half of the 1990s in France and assessed their trends in the recent years and since the mid 1980s. We particularly aimed to investigate whether the declining trends of CHD morbidity and mortality observed from 1985–1993 still persisted in the second half of the 1990s. However, a simplified registration procedure compared with the MONICA protocol has been used since 1997. An annual validation system was therefore necessary to take into account these methodological differences when time trends of the main indicators were assessed from 1985–2000.
Methods
Population
The French CHD registers located in Lille (in the north of France), Strasbourg (north-east) and Toulouse (southwest) cover geographical areas of about one million inhabitants each: respectively the Urban Community of Lille, the district of Bas-Rhin and the district of Haute-Garonne. Coronary events are monitored in the 35–74 year age group for non-fatal and in-hospital fatal events and in a restricted 35–64 year age group for out-of-hospital fatal events. Information on the population living in the three areas comes from the census data and extrapolations taking into account migrations and deaths for intercensal years. A national co-ordination located in Paris centralizes the French data and provides a continuous quality control.
Data collection
The present register concerns men and women resident in the three geographical areas with one of the following pathological events.
Acute myocardial infarction: the diagnosis should be made by a clinician on the basis of the complete history of each event.
Fatal events: coronary deaths, sudden deaths and deaths of unknown cause. All deaths among the population of suitable age groups are identified and selected for validation from a list of diagnoses recorded on the death certificates according to the International Classification of Diseases (ICD), ninth revision [8].
The event must have been detected and diagnosed within 28 days of onset. Survival at 28 days after the onset of an episode was searched for. A new event is monitored only if it takes place more than 27 days after any formerly recorded coronary event in the same subject.
The case findings were sourced from public and private hospitals, emergency departments, cardiologists', and GPs' private practices. A regular screening of coroners' reports was performed. All registered death certificates were reviewed monthly and selected for validation. General practitioners were mainly interviewed during the search for further information on causes of death [9]. Details on the circumstances of death, death certificate diagnosis and findings at autopsy were recorded. Every year, the list of registered events is cross-checked with the computerized list covering the hospital discharge diagnoses to ensure the completeness of the registration.
Classification of events
Each event is classified in a diagnostic category.
Myocardial infarction (MI): the documented event, whether non-fatal or fatal, has definitively been diagnosed as an MI whether clinically or at autopsy. Logically, all non-fatal recorded events belong to this category.
Coronary death (CD): fatal event, whether sudden or not, for which there is no good evidence of another cause of death – clinically or at necropsy – but with typical or atypical symptoms, or with a history of chronic CHD, or with evidence of chronic coronary occlusion or stenosis or old MI at necropsy.
Possible coronary death (PCD): rapid death in less than 24 h, with no history of typical or atypical symptoms, no history of chronic CHD, no necropsy and with no other diagnosis.
Validation procedure
An annual validation system for a 15-day period, arbitrarily determined from the 1–15 November, has been established to evaluate the consistency and the continuity of the indicators measured with the two registration protocols (the present register and the MONICA register). The major difference lies in the MI event category, since registration procedures of fatal events are similar. In fact, in the MONICA register, definite MI events had to verify strict clinical, biological and ECG criteria. In the present register, clinicians might conclude to MIs for all these events, but they would also recognize other milder or sub-acute events as MIs. During the validation period, all potential events are then analyzed twice and classified in their appropriate categories following the procedure suitable for each protocol. Ratios of numbers in corresponding categories (validation ratios) have been used to correct for the registration changes.
Statistical methods
Age-standardized morbidity and mortality rates were obtained according to the direct method with 5-year age groups and the world standard population. Recurrent events were defined as those with a previously recorded MI episode. Case fatality, defined as the proportion of events that were fatal by the 28th day, was computed for in-hospital events and for the totality of events. The trends in event rates were computed with log-linear Poisson regression models with the year as an independent variable. Validation ratios obtained from the four annual validation periods (1997–2000) were applied to the data of the corresponding years and were used to weight 1997–2000 data in the regressions. When assessing time trends since 1985, departure from linearity was assessed by adding a quadratic term for year in the model. When it was statistically significant, linear trends were tested over three separate periods: 1985–1988; 1989–1993; and 1997–2000. Statistical tests were considered with a significance level of 0.05. All analyses were performed using the SAS software (version 8, SAS Institute Inc., Cary, North Carolina, USA).
Results
Present register (1997–2000)
During the four years, 2555 events were collected in Lille, 2619 in Strasbourg and 1919 in Toulouse, in the 35–64 year age group (Table 1). The man/woman ratios were 4.6, 4.5 and 6.6 respectively. The distribution per diagnostic category was close in the three centres, except for the proportion of non-fatal events, which was higher in Toulouse than in the two other centres, and especially when Toulouse was compared with Lille.
As shown in Figure 1, the rates of MI rose continuously with increasing age from 4.5/100 000 in women and 56/100 000 in men in the 35–44 year age group in Toulouse to 234 in women and 582 in men in the 65–74 year age group in Strasbourg. The 4-year annual standardized CHD rates were consistently higher in Strasbourg and in Lille than in Toulouse, whatever the definition of events used (MI, MI and CD or MI + CD + PCD) (Table 2). The between-centre ratios Strasbourg/Toulouse or Lille/Toulouse extended from 1.19–1.38 in men and from 1.77–2.23 in women. Poisson regressions revealed no specific trend by centre and gender, except in Lille where rates tended to increase in women for all definitions.
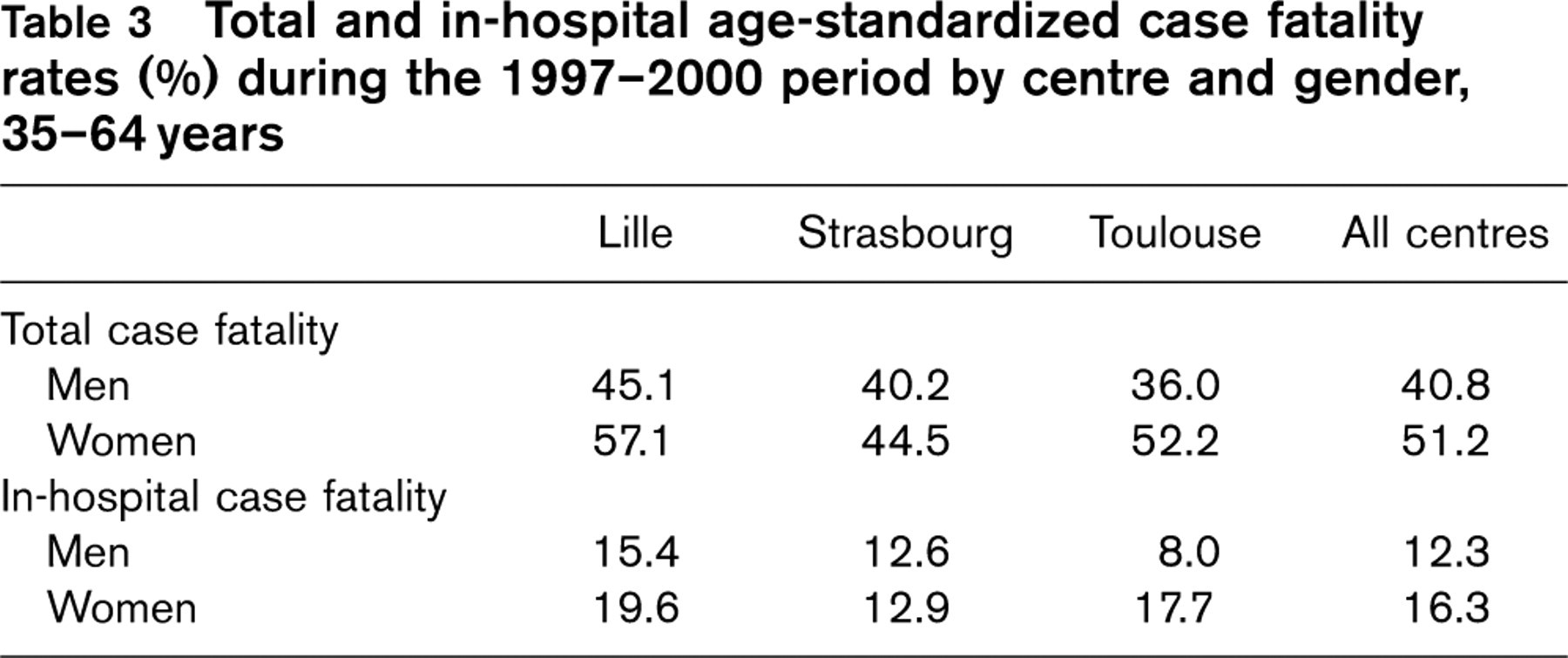
Table 3 displays total and in-hospital standardized case fatality rates during the 1997–2000 period. In women aged 35–64, one of two events was fatal by the 28th day and this proportion was higher than in men (40%) in all centres. Time trends in total case fatality (the three centres combined) revealed a decrease in both genders (P = 10−4). However, a declining trend was not significant when separate analyses were performed by centre.
Number of events registered from 1997–2000 in the three French centres in the 35–64 year age group
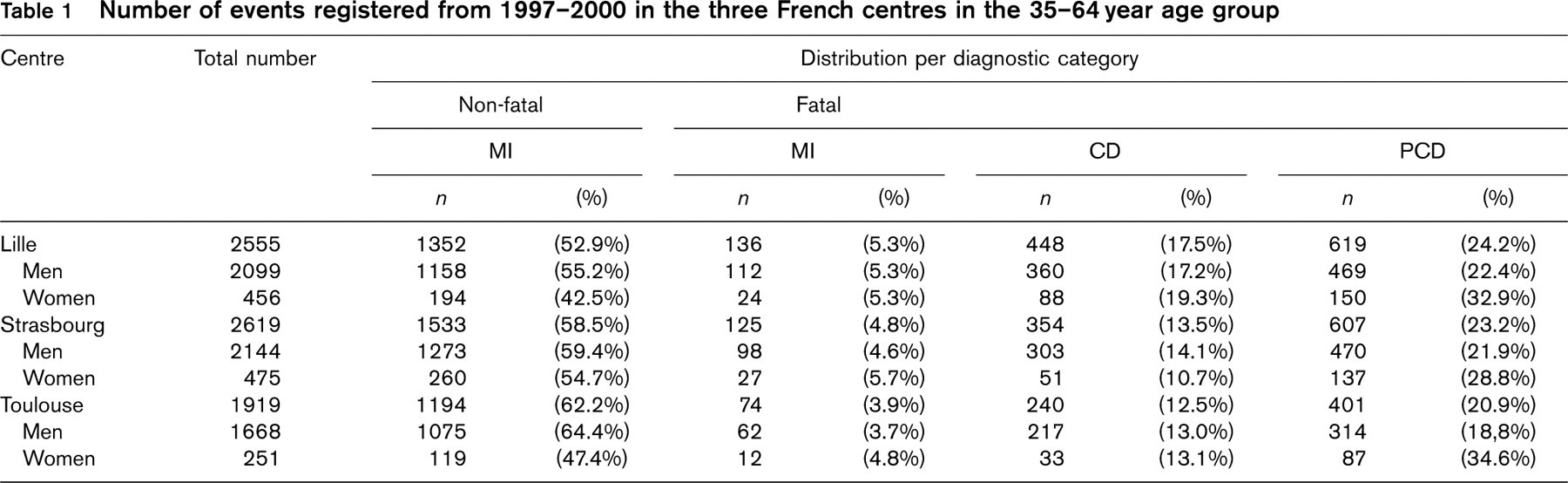
MI, myocardial infarction; CD, coronary death; PCD, possible coronary death.
The 28-day in-hospital case fatality rates increased with age in both genders (from 5.8 in men and 10.1 in women in the 35–44 year age group to 16.8 in men and 22.4 in women in the 55–64 year age group) whatever the centre. The highest in-hospital case fatality rates were observed in Lille in both genders and the lowest ones in Toulouse men and Strasbourg women. Analyses of time trends in in-hospital case fatality during these 4 years showed a non-significant declining trend in all centres and genders. This trend reached statistical significance in women when combining data from the three centres (P < 10−3).
Validation procedure
For all categories, the number of events recorded in the present register is higher than that obtained from MONICA procedure (Table 4). The difference is essentially due to the number of recorded MIs. Nearly all definite MIs defined by the MONICA algorithm were considered as MIs in the new register whereas about 20% more MIs were recorded in the new register. The validation ratios displayed in Table 4 were fairly consistent between the three centres and their combined value in each gender was taken as correction factors for estimating MONICA event rates in the 1997–2000 period.
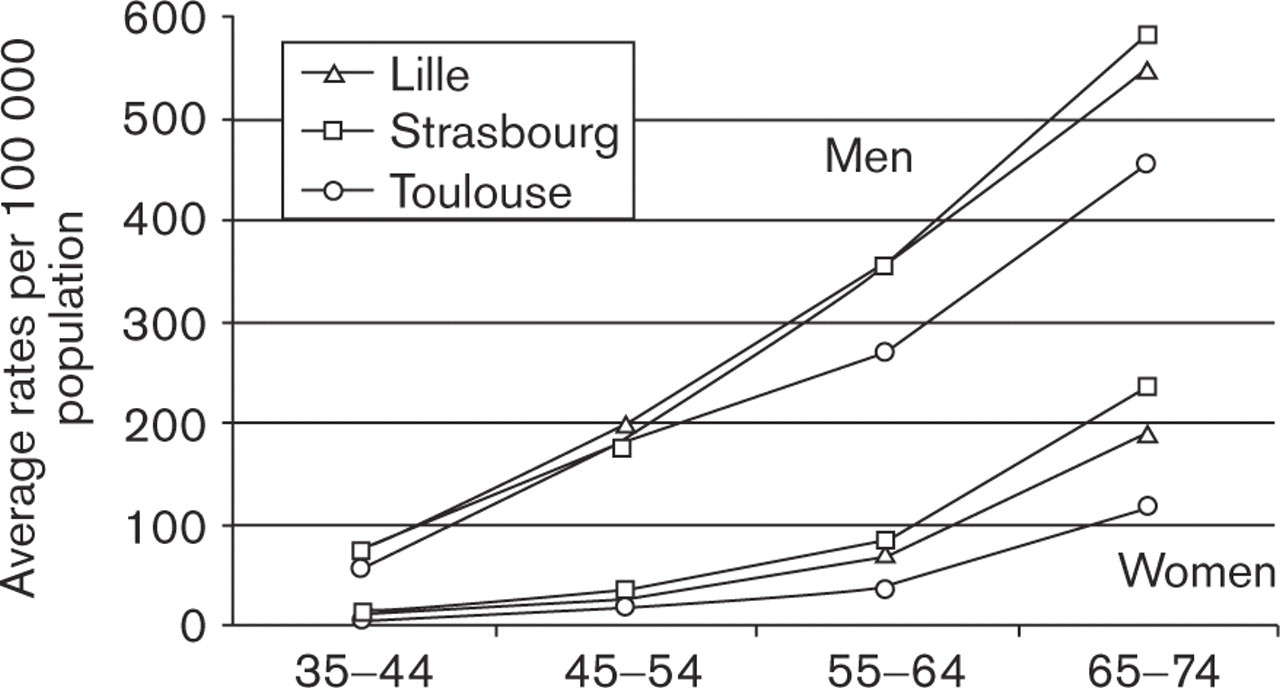
Average rates of myocardial infarction (per 100 000 inhabitants) in each centre by gender and age in the 1997–2000 period, 35–74 years.
Age-standardized annual event rates per 100 000 population during the 1997–2000 period for different definitions of events in men and women, 35–64 years
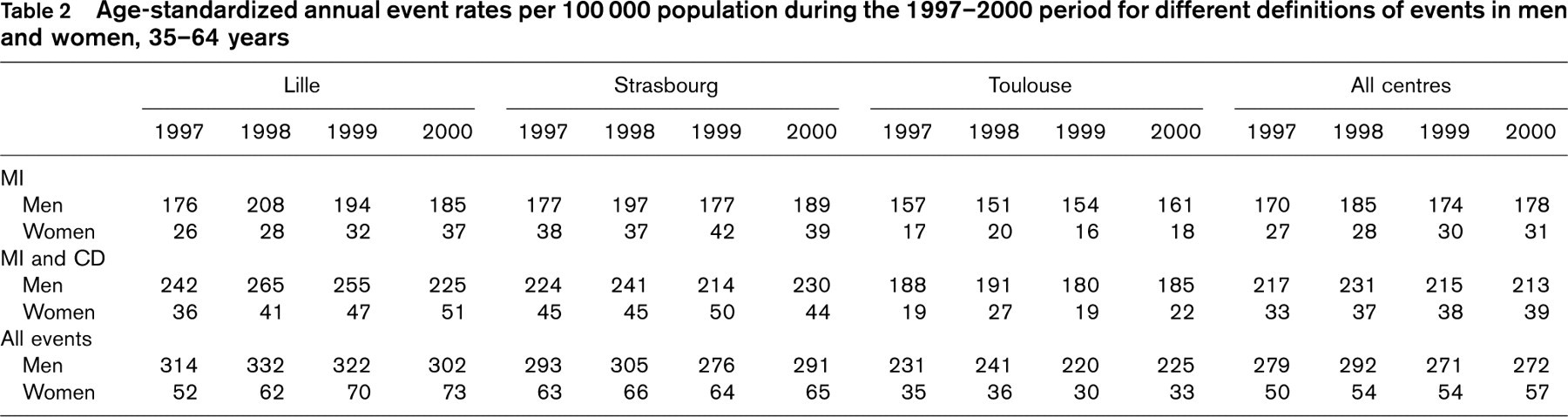
MI, myocardial infarction; CD, coronary death; PCD, possible coronary death. All events=MI+CD+PCD.
Total and in-hospital age-standardized case fatality rates (%) during the 1997–2000 period by centre and gender, 35–64 years
Time trends in CHD events (1985–2000)
Figure 2 shows trends in standardized MI + CD rates according to the MONICA protocol between 1985 and 2000 for the combined centres by gender. A significant decrease was obtained throughout the 15-year period and the quadratic term for the year was significant in both genders, pointing out a departure from linearity. In fact, the decreasing trend originated in the first 9 years of the global period with a stabilization in recent years among men, and an increasing trend among women. Globally, the same patterns of results were observed for total events (not shown).
Since the present registration procedure for fatal events is identical to that of the MONICA protocol, time trends in CHD mortality were evaluated without any correction for recent years (Fig. 2). A slowdown of the CHD mortality decrease in women has been apparent since 1993. A significant quadratic effect for year was disclosed with a decreasing trend in CHD mortality until 1993, followed by some stability in recent years. In men, all periods were characterized by a significant declining trend in CHD mortality.
Trends in standardized MI and CD rates between 1985 and 2000 were also analyzed by centre (Fig. 3). They decreased significantly over the 15-year period, with the exception of Lille for both genders. The quadratic term for year was significant in both genders in the Strasbourg district. In fact, in either Strasbourg or Toulouse, the decreasing trend originated in the first 9 years of the total period. Since 1997, stability in the rates of MIs and CD has been observed in all centres, with even an increasing trend in women from Lille.
Trends in CHD mortality were computed for each centre (Fig. 4). A significant quadratic effect was found in Strasbourg in both genders, and in Toulouse for men only. Separate analyses by period confirmed the curvature of the trend with a slowdown of the decrease in men from Toulouse and in women from Strasbourg. The decrease slackened during the 1989–1993 period in men from Strasbourg but was significant again in recent years. Lille was characterized by a declining global trend in mortality rates in both genders. Analyses of the 1997–2000 period showed that the decrease tended to continue in men, although not significantly, whereas an increasing trend was observed in women during the past few years.
Discussion
Registration of coronary events in France from 1997–2000 has showed stability of CHD morbidity in both genders and of mortality in women, contrasting with the decreasing trends observed during the 1985–1993 period.
Indeed, France was characterized by a marked diminution of CHD rates during the MONICA registration period [4, 7]. Since 1997, the three French centres have used a simplified registration procedure, essentially because recording MONICA diagnostic criteria had proved to be too time consuming. The clinician's diagnosis written on the discharge letter has therefore been taken into account. The simplified procedure has permitted an enlargement of the age-range up to 74 years. An annual validation procedure has been set up to allow an adequate connection between the two periods of data with a very simple multiplicative correction factor applied to attack rates.
Numbers of coronary heart disease events simultaneously recorded during 1997–2000 validation periods according to the new register and MONICA procedures and their ratios (95% confidence intervals), 35–64 years
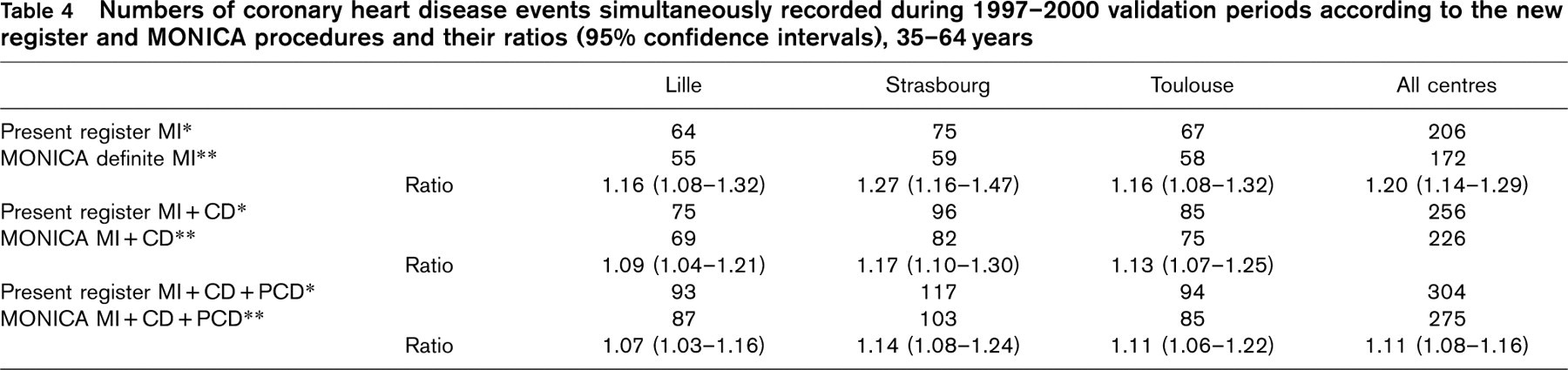
∗ MI, myocardial infarction, CD, coronary death, PCD, possible coronary death.
∗∗ MONICA MI, non-fatal or fatal definite acute myocardial infarction, MONICA CD, coronary death, MONICA PCD, death with insufficient data.
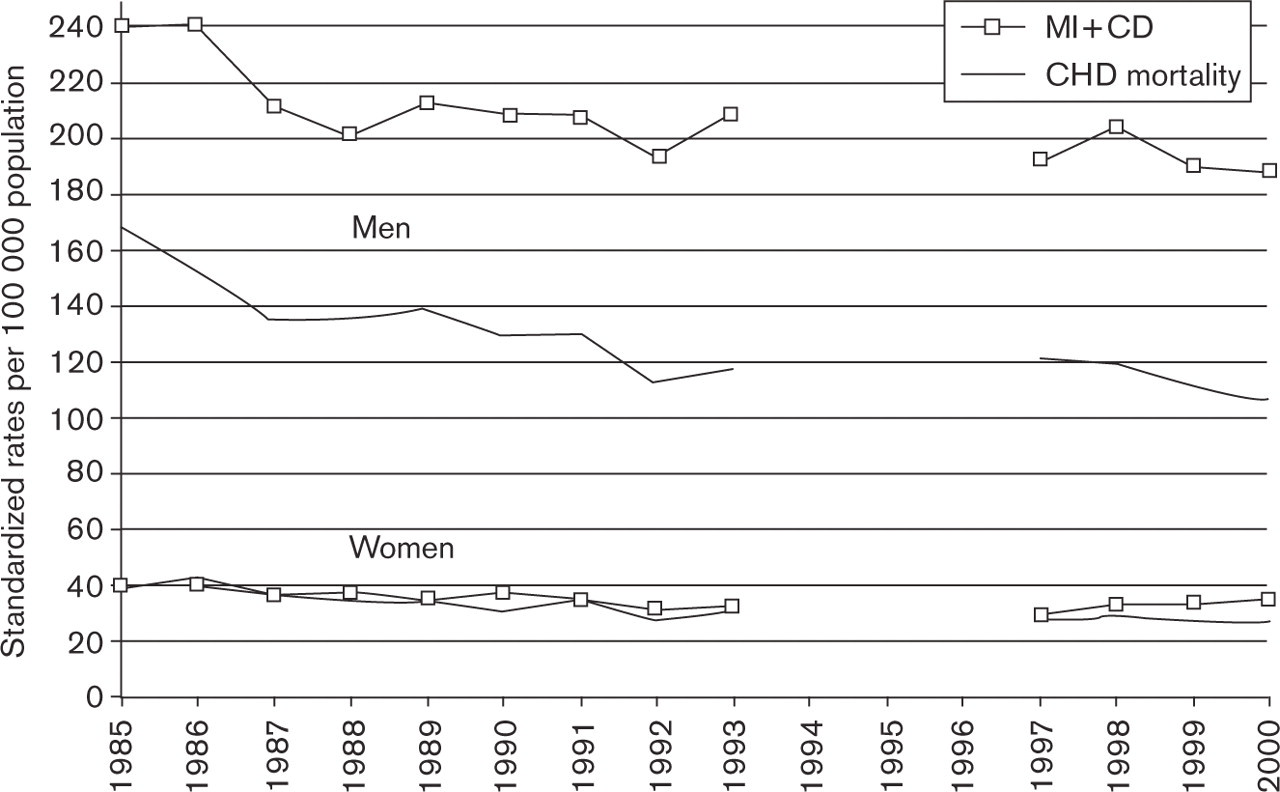
Trends in myocardial infarctions (MI) + coronary deaths (CD), and in coronary heart disease (CHD) mortality since 1985 by gender in the three centres combined, 35–64 years.
A previous paper analyzed the rate trends in the French MONICA centres, using various definitions of coronary events. Although the absolute levels of annual incidence, mortality and case-fatality rates varied according to the definition of events, the analyses of trends were mostly concordant whatever the definition, and the disparities between regions were preserved [10].
In the present register the north-to-south gradient of decreasing frequency of CHD events was still evident. This gradient was also found in the older age group (65–74 years) previously not investigated. The distribution per centre of case-fatality observed in recent years was similar to that previously found in the MONICA registers. The high total case-fatality rates, which may appear surprising, are explained by the consideration of both in-hospital and out-of-hospital events—the latter all being fatal.
Although we have observed a decrease in MI and CD rates since 1985, they were stable in the recent years in the three centres. This raises the question whether this stability is real or is related to our current methodology and to the correction by validation ratios. They were computed by combining four annual 15-day periods of validation, with a total sample of at least 200 events, which should allow a precise correspondence between the two registration procedures. Moreover, the fact that CHD mortality rates were also fairly stable in recent years, without using any correction by validation ratios, supported the hypothesis of stability.
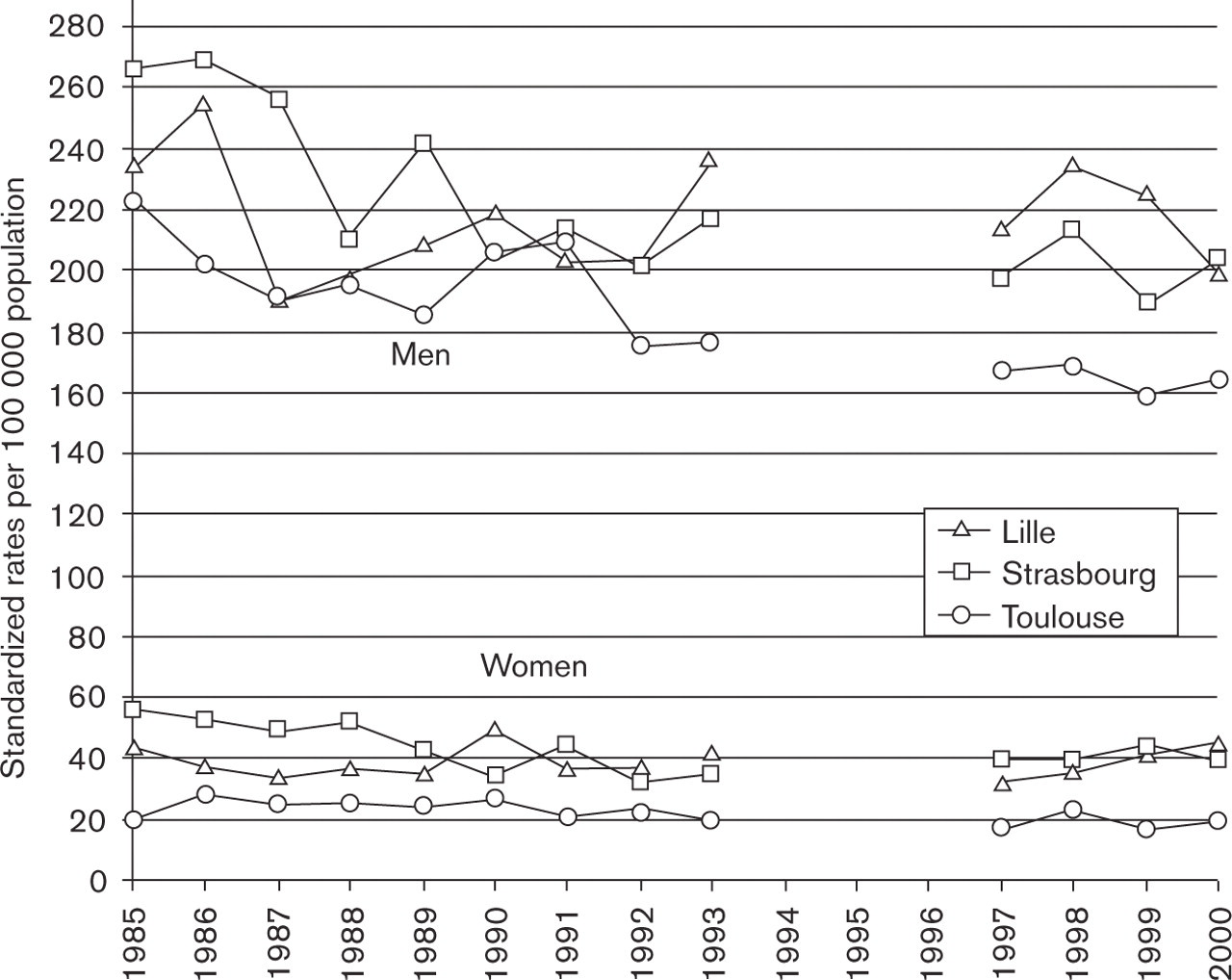
Trends in myocardial infarction + coronary deaths rates since 1985 in each centre by gender, 35–64 years.
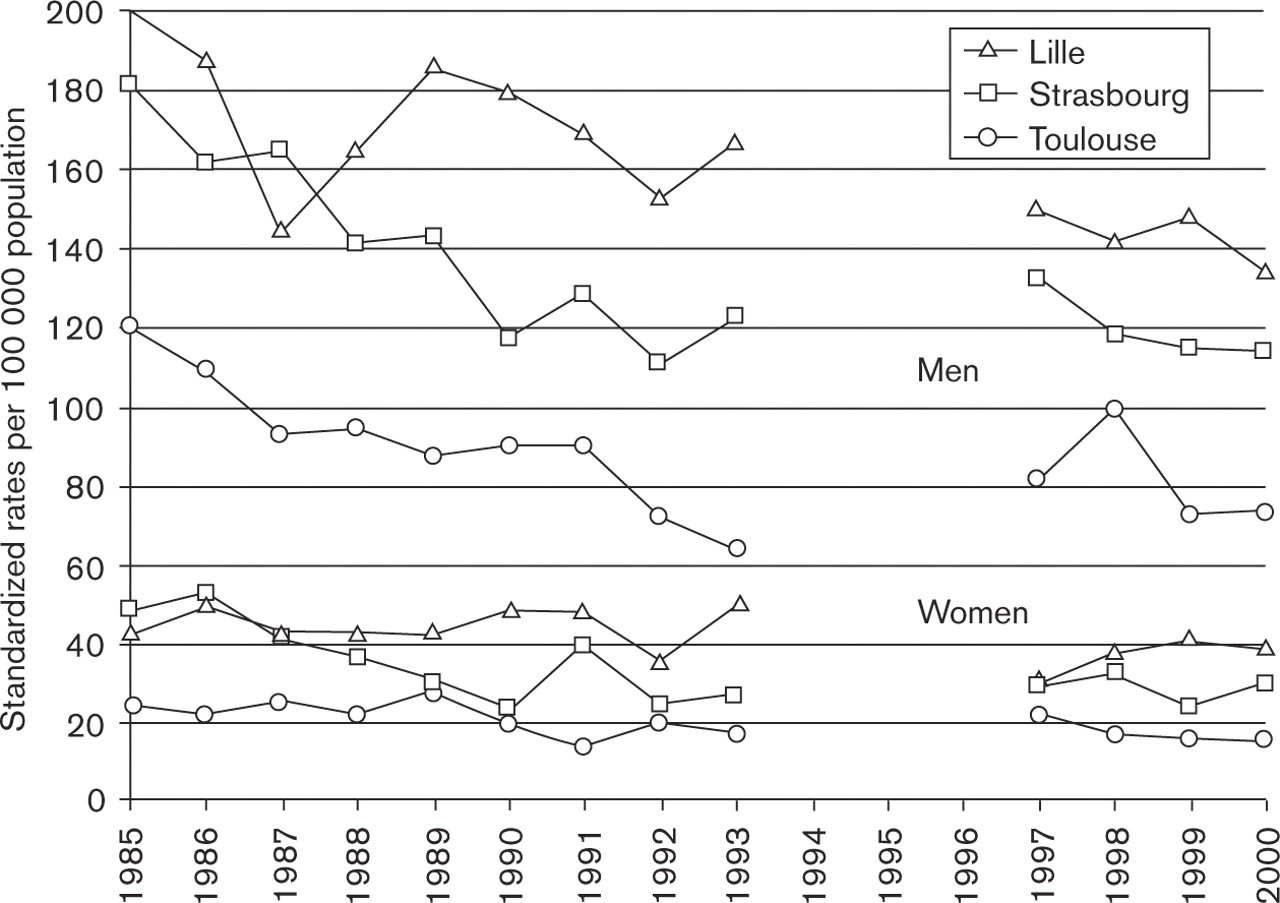
Trends in coronary heart disease mortality since 1985 in each centre by gender, 35–64 years.
Similarly, data from the same three geographical areas obtained from the National Mortality Statistics between 1985 and 1999 also showed the same patterns of evolution concerning the deaths ascribed to CHD (ICD 9 codes 410–414).
In other countries where the MONICA registration procedure was continued and reported, a decreasing trend in CHD morbidity or mortality was observed until recent years, in Italy [11] (MONICA Brianza), Germany [12] (MONICA Augsburg) and Finland [13, 14] (FIN MONICA). In Germany, time trends were computed during the 1983–1998 period but separate analyses concerning more recent years were not described. In France, we also observed a globally negative trend in CHD morbidity and mortality for the whole 1985–2000 period. Nevertheless, in contrast to the recent stability pointed out in France, a reduction in the occurrence of CHD events was still observed in the past decade in men in Italy or in both genders in Finland. In the USA [15], recent data obtained on the basis of hospital registers also showed a continuation of the decline in CHD rates. Of course, the differences in event registration, methodology and age groups make any comparison between countries difficult.
The lack of recent data concerning the management of acute and chronic CHD and the prevalence of cardiovascular risk factors in the population did not allow us to discuss further the causes of the present stability in France. We might also postulate, at least for Toulouse, that since CHD rates were among the lowest in western countries during the MONICA period, the continuation of the decrease in this area would be less statistically evident than in countries with much higher rates in the early 1990s.
One weakness of our study should be mentioned. We assessed recent trends on the basis of 4 years of registration. This period might be too short to predict the future evolution of CHD rates in France and further data during the early 2000s are necessary to make more specific predictions.
In conclusion, data obtained with a simplified registration system in the second half of the 1990s still highlight a north-to-south gradient of decreasing frequency of CHD within France, even in the 65–74 year age group. The decreasing trend in CHD events observed from the mid-1980s to the early 1990s seems to have markedly slowed down.
Footnotes
Acknowledgements
This work was supported by a grant from the Institut National de la Santé et de la Recherche Médicale (INSERM) and from the Institut National de Veille Sanitaire (INVS). We would like to thank the Investigators of the three French Centres for their invaluable contribution to the careful collection and validation of the data, the physicians and the cardiologists who helped in this process.