
Abstract
Background We investigated the association between estimated aerobic fitness and cardiovascular risk factors, and how the association is affected by abdominal obesity.
Design Cross-sectional population study.
Methods Participants comprised 3820 adults aged 25 to 64 years from the FIN RISK 2002 Study in Finland. Aerobic fitness was estimated using a non-exercise test. Waist-to-hip ratio (WHR), blood pressure, total cholesterol, high-density lipoprotein cholesterol (HDL-C), triglycerides, HDL-C to total cholesterol ratio, and gamma-glutamyl transferase (GGT) levels were measured by standardized methods.
Results After controlling for age, smoking and alcohol consumption, aerobic fitness was inversely associated with systolic (P=0.027) and diastolic (P<0.001) blood pressure, total cholesterol (P=0.009), triglycerides (P=0.001), and GGT (P<0.001), and directly associated with HDL-C (P<0.001) and HDL-C to total cholesterol ratio (P<0.001) in men. In women, inverse associations were found for diastolic blood pressure (P=0.027) and triglycerides (P<0.001), and direct association for HDL-C (P<0.001) and HDL-C to total cholesterol ratio (P<0.001). Waist-to-hip ratio was independently associated with a better risk factor profile in both sexes. Interactions were found between fitness and WHR in relation to total cholesterol (P=0.001), HDL-C to total cholesterol ratio (P=0.005), triglycerides (P=0.001), and systolic (P=0.009) and diastolic (P<0.001) blood pressure among men only.
Conclusions Our data suggest that good estimated aerobic fitness is associated with a better cardiovascular risk factor profile, regardless of the level of abdominal obesity in Finnish men and women. Men in the highest WHR third seem to have more benefit of aerobic fitness on their cardiovascular risk levels than men with lower WHR. Eur J Cardiovasc Prev Rehabil 12: 126–131 © 2005 The European Society of Cardiology
Keywords
Introduction
Major risk factors for cardiovascular diseases include smoking, elevated levels of systolic and diastolic blood pressure, and serum total cholesterol, as well as low levels of high-density lipoprotein cholesterol (HDL-C) [1]. In addition, serum triglycerides, alcohol use, and diet have been shown to predict cardiovascular diseases [2, 3]. Obesity, particularly abdominal obesity, and physical activity are considered as both independent and mediating factors in the development of cardiovascular diseases [4, 5]. Gamma-glutamyl transferase (GGT), a liver enzyme, may also be associated with cardiovascular risk [6–8], although less studied in this respect.
Previous studies have shown that cardiovascular disease risk factor profile is better among those with higher levels of cardiorespiratory fitness or physical activity [9–16]. Only few studies have reported the combined effect of cardiorespiratory fitness or physical activity and obesity on risk factor levels, and none of them have used waist-to-hip ratio (WHR) as a measure of obesity [17–20]. Importantly, these studies found that blood pressure or lipids were better among the physically most active, the fittest and the leanest, while good fitness improved the risk factors regardless of the level of obesity. More studies are needed on the associations of cardiorespiratory fitness and abdominal obesity with cardiovascular risk factor levels, particularly in large population samples of both men and women and with a wide age range.
The aim of the study was to investigate the association of estimated aerobic fitness with cardiovascular risk factor profile by using a novel non-exercise fitness test in a large population sample of men and women 25–74 years of age, and further whether the association is affected by the degree of abdominal obesity, when using WHR as a measure of obesity.
Methods
Study population and design
This cross-sectional population study was part of the National FINRISK 2002 Study, which was conducted in the spring 2002 to monitor cardiovascular risk factors among Finnish adults aged 25–74 years. A stratified random sample by sex and 10-year age group comprised 13 500 subjects and was drawn from the Population Register in six geographical regions in Finland. Physical activity sub-sample included 8159 men and women aged 25–64 years. Participation rates were 59% (n = 2415) for men and 70% (n = 2873) for women. The Ethics Committee of the National Public Health Institute approved the study protocol and the participants gave their written consent. The study protocol, sampling, anthropometric and blood pressure measurements, as well as laboratory analyses, followed the WHO MONICA Project protocol closely [21] and the later recommendations of the European Health Risk Monitoring Project [22].
Individuals with any self-reported cardiovascular disease or related condition (angina pectoris, myocardial infarction, coronary artery bypass surgery, coronary angioplasty, stroke, heart failure, or medication for hypertension in the last 7 days) were excluded from the further analyses (n = 1192). These conditions and treatments might affect the heart rate variation, which is the essential factor in estimating aerobic fitness by the non-exercise test and thus can cause bias to the fitness estimates. Participants were excluded if any variable used in the analyses was missing. The final sample included 1787 men and 2033 women.
Measurements
Participants were mailed a self-administered questionnaire to be filled in at home, before arriving at the study site. The questionnaire included questions on medical history, smoking and alcohol behaviour, as well as menopausal status and hormone replacement therapy (in women). Smoking behaviour was assessed by a frequency of smoking and dichotomized into daily smokers or non-smokers. Alcohol consumption was calculated as grams of pure alcohol per week using a recall of the preceding week.
At the study site, a trained nurse carried out the following measurements: body weight and height, waist and hip circumference, blood pressure, and fitness test. Blood samples after 4-h fasting were drawn for lipid and GGT analyses. Waist girth was measured at the midpoint between the iliac crest and the lowest rib, and hip girth at the widest part of the pelvis. The WHR was calculated and divided into sex-specific thirds. Cut-off points were 0.93 and 0.98 for men and 0.80 and 0.85 for women. Blood pressure was measured after 5 min rest from the right arm in a sitting position. The mean of the first and the second blood pressure measurements was used in the analyses. From the blood sample, total cholesterol, HDL-C, triglycerides, and GGT levels were analysed, and HDL-C to total cholesterol ratio was calculated. All analyses were carried out at the central laboratory of the National Public Health Institute. Enzymatic methods were used to determine total cholesterol and HDL-C levels (CHOD-PAP; Thermo Elektron Oy, Finland), and triglyceride levels (GPO-PAP; Thermo Elektron Oy). Levels of GGT were measured by a kinetic method (ECCLS; Thermo Elektron Oy) as recommended by the European Committee for Clinical Laboratory Standards.
A non-exercise aerobic fitness test (the Polar Fitness Test; Polar Electro Oy, Kempele, Finland) was carried out. The fitness test estimates maximal aerobic power based on subject's weight, height, age, sex, the score of self-reported physical activity, and resting heart rate measurements. The test was carried out with the Polar S810 heart rate monitor (Polar Electro Oy) at rest, in a sitting position with legs placed at a horizontal level. The different validity tests of the Polar Fitness Test [23] against maximal oxygen consumption measured during a maximal treadmill test have reached correlation coefficients of 0.80 (standard error, SE, ± 5.1 ml/kg per min), 0.95 (SE 4.6 ml/kg per min) and 0.93 (SE 5.1 ml/kg per min), suggesting that the estimated aerobic fitness is a good measure of aerobic fitness. A more detailed description and validation results on Polar Fitness Test and the use of artificial neural networks and heart rate variability in estimating aerobic fitness have been reported elsewhere [23–26]. Based on the estimated aerobic fitness, expressed as ml/kg per min, the participants were first divided into seven sex and age-specific fitness classes: very poor, poor, fair, average, good, very good, and excellent, according to international classification standards published by Shvartz and Reibold [27]. For the analyses, the classes were merged into three major fitness categories: low (very poor, poor, fair), middle (average, good) and high (very good, excellent).
Statistical methods
We used the Statistical Package for Social Sciences (SPSS, version 11.0. 1; Chicago, Illinois, USA) for all analyses. Each risk factor; systolic and diastolic blood pressure, total cholesterol, HDL-C, HDL-C to total cholesterol ratio, triglycerides, and GGT, were analysed separately using a 3 × 3 analysis of covariance. With this method we were able to investigate the effect of estimated aerobic fitness and WHR separately and independently, and also for their combined effect on each risk factor. This allowed us to interpret the independent effect of aerobic fitness on risk factors at different levels of obesity. In the analyses, we adjusted for the following potential confounders: age, smoking behaviour, and alcohol use, as well as menopausal status and hormone replacement therapy for women. Men and women were analysed separately.
Results
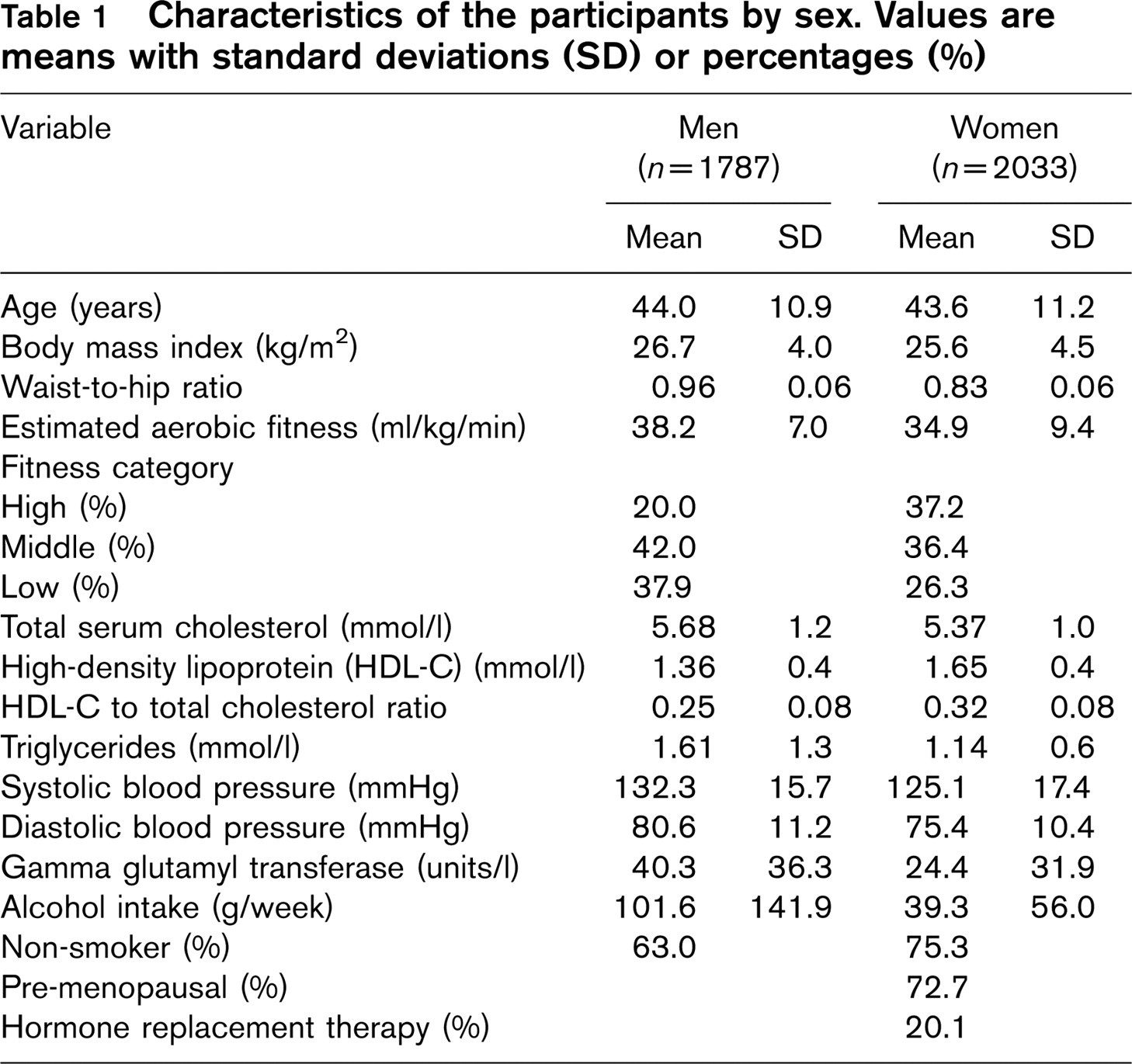
Major characteristics of the study population by sex are described in Table 1. The mean estimated aerobic fitness was 38.2 ml/kg per min for men and 34.9 for women. About 20% of men belonged to the ‘highly fit’ group, whereas in women, 37% were defined as ‘highly fit'.
In men, aerobic fitness had an inverse association with systolic and diastolic blood pressure, and serum total cholesterol, triglyceride and GGT levels (Table 2). A direct association was found between aerobic fitness and HDL-C, and HDL-C to total cholesterol ratio. The WHR had a direct association with systolic and diastolic blood pressure, total cholesterol, triglycerides and GGT, and inverse association with HDL-C and HDL-C to total cholesterol ratio. Statistically significant interactions between fitness and WHR were found in total cholesterol, HDL-C to total cholesterol ratio, triglycerides, and both systolic and diastolic blood pressure. Interactions related to total cholesterol and systolic blood pressure were unsystematic and difficult to interpret, but the association of aerobic fitness with HDL-C to total cholesterol ratio, triglycerides and diastolic blood pressure tended to be stronger among the abdominally obese than the lean men.
Characteristics of the participants by sex. Values are means with standard deviations (SD) or percentages (%)
In women, aerobic fitness had an inverse association with diastolic blood pressure and triglycerides and a direct association with HDL-C, and HDL-C to total cholesterol ratio (Table 3). Similarly as in men, WHR had a direct association with systolic and diastolic blood pressure, total cholesterol, triglycerides and GGT, and inverse association with HDL-C and HDL-C to total cholesterol ratio. Statistically significant interactions between fitness and WHR were found in triglycerides and GGT. The association of aerobic fitness with serum triglyceride and GGT levels was stronger among obese than lean women.
When the analyses were performed among pre-menopausal women only, the results did not change markedly, except the association between fitness and diastolic blood pressure became weaker. Analyses were not performed separately for post-menopausal women (n = 488), because the number of subjects in certain fitness and obesity groups were very low.
Discussion
Our results suggest that in the healthy Finnish adult population estimated aerobic fitness is independently associated with a better risk factor profile. Particularly strong and clinically significant associations existed for HDL-C and HDL-C to total cholesterol ratio in both sexes, and for triglycerides, GGT, and blood pressure in men. The WHR had strong associations with all measured risk factors. Those who were both unfit and abdominally obese had the most unfavourable risk factor profile. In general, obese individuals tended to benefit more from aerobic fitness than lean persons in regards their risk factor levels.
Mean risk factor levels by estimated aerobic fitness and waist-to-hip ratio (WHR) in men. Adjusted for age, smoking and alcohol use in two-way analysis of covariance
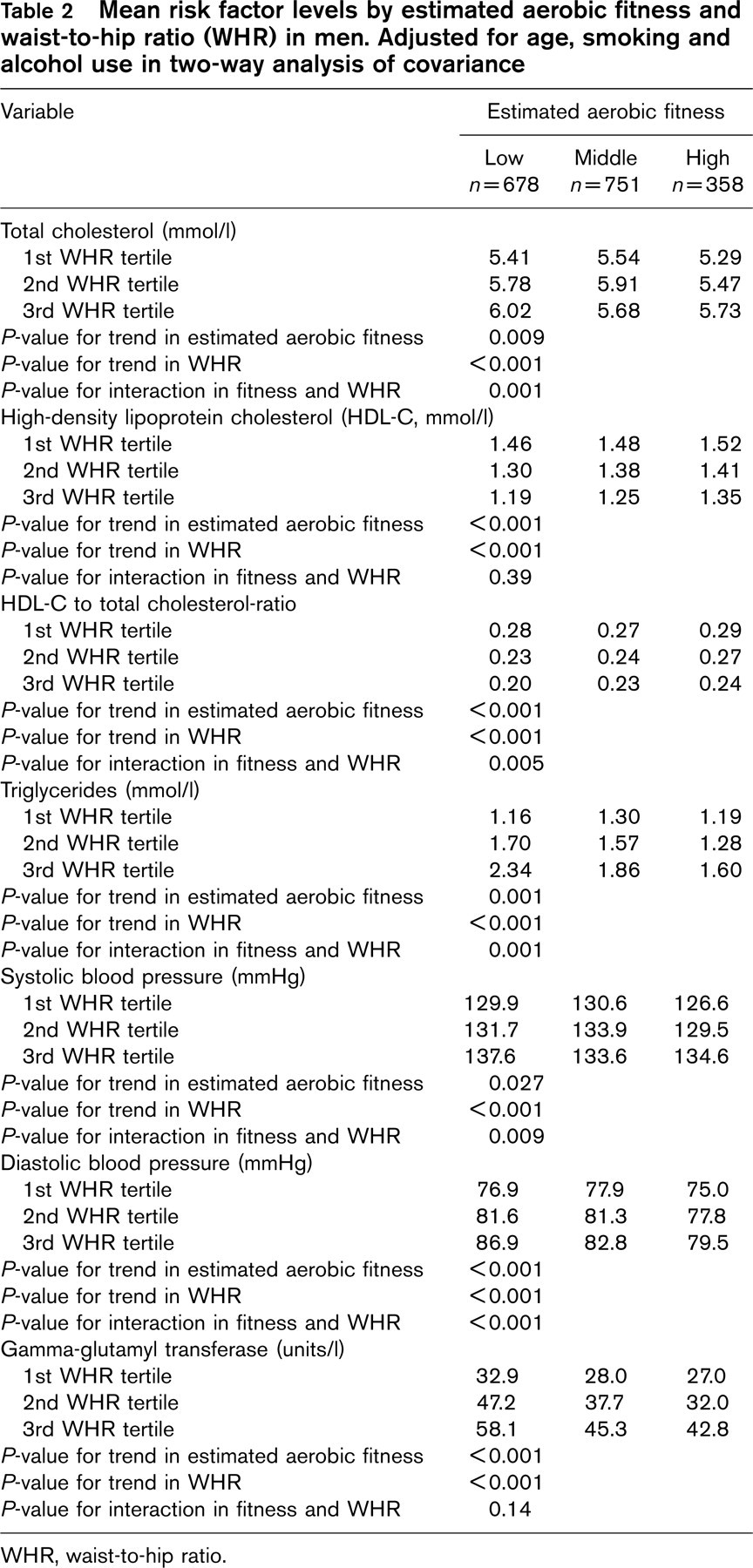
WHR, waist-to-hip ratio.
Aerobic fitness in most individuals is a result of long-term physical activity behaviours, and perhaps associates more strongly with risk factors than self-reports on physical activity [9, 28, 29]. The Polar Fitness Test is a new method of estimating aerobic fitness. It is simple and safe to carry out, and seems to be useful in population studies. The test uses self-reported leisure time physical activity measurement as one part of the test, which naturally gives a possibility for recall bias. Nevertheless, it should be emphasized that in a study of this magnitude, any other field or laboratory measurement of aerobic fitness is not feasible in the 10-week time frame of our study protocol.
Mean risk factor levels by estimated aerobic fitness and waist-to-hip ratio in women. Adjusted for age, smoking, alcohol use, menopausal status, and hormone replacement therapy in two-way analysis of covariance
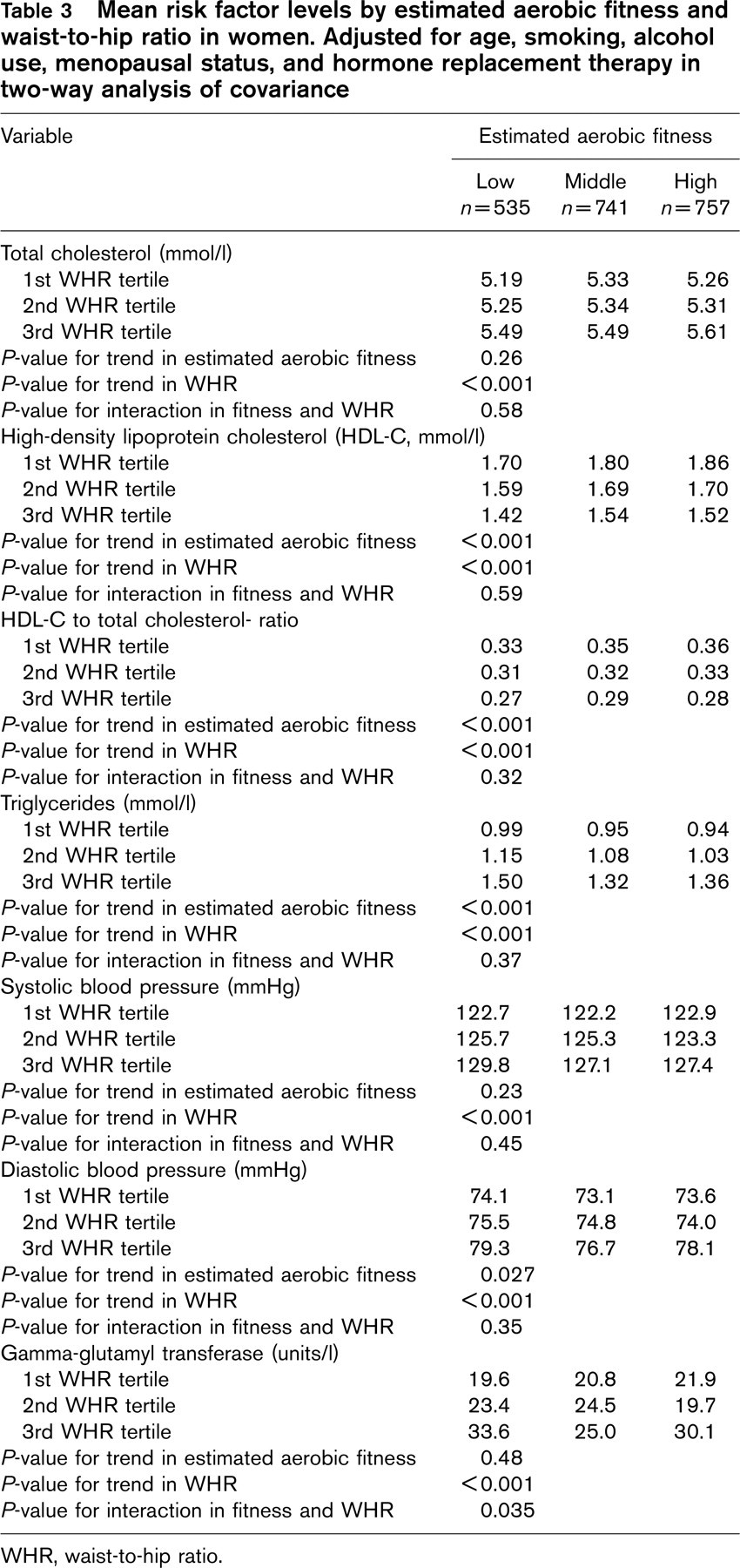
WHR, waist-to-hip ratio.
Distribution into fitness categories was different in men and women. While 20% of men belonged to the ‘high fitness’ group, a much larger proportion, 37%, of women were classified as highly fit. Most of these highly fit women were older, from the age group 55–64 years of age. Potential explanations for this high fitness group could be that the healthy older women in this population sample were actually truly fit, or that the Polar Fitness Test overestimated the aerobic fitness of these older women [24].
Some of the associations between estimated aerobic fitness and risk factors were stronger in men than women, and no interactions were found among women. This could result from different distributions of fitness categories in men and women, from menopausal status, or from hormone replacement therapy in women. However, the results remained unchanged in pre-menopausal women suggesting that hormonal status is an unlikely explanation. It is also noteworthy that WHR might function differently as a measure of obesity for men and women, mainly due to sex-specific propensities to gain extra fat at different locations of the body.
Our results are in concordance with many earlier studies on aerobic fitness and cardiovascular risk factors [9, 19, 30–32]. Most population studies use self-reported physical activity instead of aerobic fitness and thus their results are not fully comparable to ours. Nevertheless, our findings agree with many larger studies that self-reported physical activity is associated with a favourable blood lipid profile and lower blood pressure [14, 15, 20, 33]. One Finnish prospective study found a similar association between physical activity and hypertension [34]. Unexpectedly, we found no association between estimated aerobic fitness and systolic blood pressure in women. Concordant findings have been reported also from other studies [35, 36]. The plausible causes for these unexpected results could be related to the validity of estimated fitness level and their cut-off points, as the mean systolic blood pressure levels declined by fitness categories in women, but the decline was not dose dependent. Also, WHR is more strongly associated with blood pressure than aerobic fitness in women.
We found significant associations of aerobic fitness and WHR with GGT in men, but not in women. Similar findings have been reported previously with occupational physical activity and GGT [16]. Population studies on the association of fitness or physical activity with GGT are sparse, have included mainly men, and have not studied the inter-relations of physical activity and obesity [7, 37]. Gamma-glutamyl transferase is used both as a marker of obesity and long-term alcohol use. We additionally found that the leaner and fitter the men were, the lower was their self-reported alcohol consumption. In women, the more obese reported heavier alcohol use, but no difference in the alcohol use was found across the aerobic fitness categories.
Inter-relation between aerobic fitness and obesity has not been studied much in relation to cardiovascular risk profile. Our results agree with previous data, showing that overweight persons with high level of aerobic fitness also have a better blood lipid profile [18] and lower hypertension prevalence [17, 19]. A recent large cross-sectional study [20] suggested that obese individuals improved their risk profile more with physical activity than leaner persons. Similar results on the interaction were also found for coronary heart disease [38], all-cause and cardiovascular mortality [39, 40]. Contradictory, one Finnish study found no interaction between fitness and obesity with respect to all-cause and cardiovascular mortality [28].
These results provide new information on the associations of estimated aerobic fitness, obesity, and cardiovascular risk factors among a population-based random sample of relatively healthy individuals. The cross-sectional design of our study, however, limits the interpretation of the associations of the aerobic fitness with the risk factors to some extent. It is possible that healthier people with a better risk factor profile are more physically active, but because we excluded 1192 individuals with cardiovascular disease or related condition and hypertension medication, the effect of selection bias is most probably minor.
In conclusion, two important public health messages can be conveyed from this study. First, having both a good aerobic fitness and a low WHR seems to be beneficial to cardiovascular risk profile. Second, aerobic fitness may be more beneficial to abdominally obese than normal weight persons. More pronounced research on the association between aerobic fitness, obesity, and risk factor profile among women should be implemented in the future.
Footnotes
Acknowledgements
Some parts of the manuscript were presented at the Annual Meeting of the European College of Sport Science, July 2004, Clermont-Ferrand, France. This study was supported by a grant from the Finnish Ministry of Education and from the Polar Electro Oy. In addition, the corresponding author, K. B. received personal salary from the Doctoral Programs in Public Health, University of Helsinki. R. L. works as a Director, Exercise Science, at Polar Electro Oy.