
Abstract
Objective Metabolic syndrome is a condition that promotes atherosclerosis and increases the risk of cardiovascular mortality and morbidity. We evaluated whether leisure time physical activity is associated with the levels of inflammatory and coagulation markers, in people with metabolic syndrome.
Methods From May 2001 to December 2002 we randomly enrolled 1514 men and 1528 women (>18 years old), without any clinical evidence of cardiovascular disease, stratified by age-gender (census 2001). The population of the study was divided into those who fulfilled the NCEP ATP III criteria for the metabolic syndrome (n = 701 or 33% men and 13% women) and the rest of the participants (n = 2341). We assessed the relationship between self-reported physical activity status and inflammatory, and coagulation markers [i.e., C-reactive protein (CRP), serum amyloid-A (SAA), interleukin (IL)-6, tumour necrosis factor (TNF)-α, white blood cell (WBC) counts, and fibrinogen (FIB)], after taking into account the effect of several confounders.
Results Of the non-metabolic syndrome group, 56% of men and 58% of women were classified as sedentary, while of the metabolic syndrome group 58% men and 72% women were sedentary. After controlling for various potential confounders we found that physically active individuals with the metabolic syndrome had 36% lower levels of CRP, 15% lower levels of WBC, 19% lower levels of SAA, 15% lower levels of TNF-α, 30% lower levels of IL-6 and 15% lower levels of FIB, compared to sedentary (all P<0.05). Similar results were observed in the non-metabolic syndrome group.
Conclusions The adoption of a physically active lifestyle is independently associated with lower levels of the investigated biomarkers in individuals with the metabolic syndrome. The latter may suggest a pathway for reducing cardiovascular events, even in high-risk people. Eur J Cardiovasc Prev Rehabil 12: 151–158 © 2005 The European Society of Cardiology
Introduction
The metabolic syndrome is a condition that promotes atherosclerosis and increases the risk of cardiovascular events [1–3]. The characteristics of the metabolic syndrome include atherogenic dyslipidemia, a pro-thrombotic state, insulin resistance, hypertension and abdominal obesity [2]. Each abnormality promotes atherosclerosis independently, but when clustered together, these metabolic disorders are increasingly atherogenic and enhance the risk of cardiovascular morbidity and mortality. In recent years, health care professionals have focused on prevention and therapy of the atherosclerotic diseases through the evaluation and modification of several risk factors. Special attention has been given in high-risk populations, like people with the metabolic syndrome. Recently the NCEP ATP III suggested a number of Therapeutic Lifestyle Changes [2] in order to reduce the prevalence of the metabolic syndrome, which revealed the importance of diet and exercise.
The beneficial effect of physical activity on coronary heart disease risk has already been underlined in many studies, mainly through the reduction in body mass, and arterial blood pressure levels [4–6]. Recently findings from the ATTICA study [7] confirmed previous reports [8] that physical activity was associated with lower levels of various inflammatory markers in healthy subjects. Since inflammation plays a role in the pathogenesis of cardiovascular disease [9], and metabolic syndrome could be seen as a low-grade, systemic, inflammatory condition [10], instituting anti-inflammatory measures might be beneficial in preventing or halting the progress of metabolic syndrome. To the best of our knowledge the relationship between physical activity and the inflammation and coagulation process in people with the metabolic syndrome has rarely been evaluated. In this work we investigate the association between leisure time physical activity and inflammatory and coagulation markers related to coronary heart disease [C-reactive protein (CRP), interleukin (IL)-6, tumour necrosis factor (TNF)-α, serum amyloid-A (SAA), white blood cell (WBC) counts and fibrinogen], in people with the metabolic syndrome.
Methods
Sample and design
The ‘ATTICA’ study [7, 11, 12] is a health and nutrition survey, carried out in the province of Attica (including 78% urban and 22% rural areas), where Athens is the major metropolis. The sampling was random, multistage and on the city–gender–age distribution of the province of Attica provided by the National Statistical Service (census of 2001). People living in institutions were excluded from the sampling. The number of participants was determined by power analysis, and chosen to evaluate two-sided differences between the investigated parameters and physical activity levels greater than 0.5 standard deviations, achieving a statistical power of > 0.90 at a < 0.05 probability level (P-value).
From May 2001 to August 2002, 4056 inhabitants from the above area were randomly asked to participate in the study. Of those, 3042 agreed to participate (75% participation rate); 1514 were men and 1528 were women (>18 years old). The participants had no clinical evidence of cardiovascular or any other atherosclerotic disease, as well as chronic viral infections, dental problems or any type of surgery in the past week. They also exhibited no signs of cold or flu, or acute respiratory infection, since the use of anti-inflammatory drugs could influence our findings. There were only minor differences in distribution by gender and age between the study population and the target population. Trained personnel using a standard questionnaire, which was developed for the purposes of the study, interviewed all participants.
Of the 3042 participants, 504 (33%) men and 197 (13%) women were defined as having the metabolic syndrome, according to the NCEP ATP III criteria [2]; that is, a diagnosis can be established if three or more of the following risk factors are present.
Waist circumference > 102 cm (40 in) for men or > 88 cm (37 in) for women;
Triglyceride level > 150 mg/dl;
HDL cholesterol level < 40mg/dl for men or < 50 mg/dl for women;
Blood pressure > 130/85 mmHg;
Fasting glucose > 110 mg/dl.
Physical activity ascertainment
Weekly energy expenditure was assessed in all participants by considering the frequency (times per week), duration (in minutes) and intensity of sports related physical activity during a usual week. Intensity was graded in qualitative terms such as: light (expended calories < 4 kcal/min, namely walking slowly, cycling stationary, light stretching etc.), moderate (expended calories 4–7 kcal/min, namely walking briskly, cycling outdoors, swimming moderate effort etc.) and high (expended calories > 7 kcal/min, namely walking briskly uphill, long distance running, cycling fast or racing, swimming fast crawl etc.). Participants who did not report any physical activities were defined as sedentary. For the rest, we calculated a combined score by multiplying the weekly frequency, duration and intensity of physical activity. Then we calculated the tertiles of this score. Thus, physically active participants were equally classified into three groups: ‘low physical activity’ (first tertile), ‘medium physical activity’ (second tertile) and ‘high physical activity’ (third tertile).
Although there are some concerns with self-reported physical activity, the introduced evaluation is now considered reliable, valid and has been used by many other similar studies [13].
Biochemical and clinical measurements
The blood samples were collected from the antecubital vein between 0800 h and 1000 h, in a sitting position after 12 h of fasting and avoiding of alcohol. The biochemical evaluation was carried out in the same laboratory that followed the criteria of the World Health Organization Lipid Reference Laboratories. C-reactive protein and SAA were assayed by particle-enhanced immunonephelometry (N Latex; Dade-Behring Marburg GmbH, Marburg, Germany) with a range from 0.175–1100 and 0.75–1000 mg/l, respectively. Interleukin-6 was measured with high sensitivity enzyme-linked immunoassay (R & D Systems Europe Ltd, Abingdon, UK) with a range from 0.156–10 pg/ml. The intra- and inter-assay coefficient of variation was < 5% for CRP and SAA and < 10% for IL-6. Plasma fibrinogen levels were measured using a BNII Dade-Behring automatic nephelometer. For the determination of fibrinogen, blood was anticoagulated with 3.8% trisodium citrate (9:1 vol/vol) and cooled on ice until centrifugation. The intra- and inter-assay coefficients of variation of fibrinogen did not exceed 9%. We also measured white blood cell counts using a Medicon analyser (Medicon Ltd., Athens, Greece). We used the enzyme-linked immunosorbent assay (ELISA) method for the quantitative determination of human TNF-α in duplicate in serum samples of the participants by Quantikine HS/human TNF-α immunoassay kit (R & D Systems, Inc. Minneapolis, Minnesota, USA).
Serum total and HDL cholesterols, as well as triglycerides were measured using a colorimetric enzymic method in a automatic analyser RA-1000 (Technicon Instruments, Tarrytown, New York, USA). The intra- and inter-assay coefficients of variation of cholesterol and triglycerides levels did not exceed 4%.
Arterial blood pressure was measured at the end of the physical examination with the subject in a sitting position for 25–30 min. Three measurements were obtained from the right arm (ELKA using an aneroid manometric sphygmometer; Von Schlieben Co., Berlin, West Germany). Patients whose average blood pressure levels were greater or equal to 140/90 mmHg or taking antihypertensive medication were classified as hypertensives. Participants with total serum cholesterol levels greater than 200 mg/dl or those taking lipid-lowering agents were classified as hypercholesterolaemic and those with blood sugar > 125 mg/dl or using anti-diabetic medication were classified as diabetic. However, in all statistical analyses continuous measurements of blood pressures and chemistries were used. Also, a physician recorded a detailed medical history of the participants.
Demographic and lifestyle characteristics
In addition to the physical activity status, the study's questionnaire included demographic characteristics like age, gender, family status (married, divorced, widowed), financial status (average annual income during the past three years), and education level. The educational level of the participants (as a proxy of social status) was measured in years of schooling. Information about smoking habits was collected using a standardized questionnaire developed for the study. Current smokers were defined as those who smoked at least one cigarette per day. ‘Never smokers’ were classified as those who have never tried a cigarette in their life and former smokers were defined as those who had stopped smoking more than 1 year previously. In all multivariate statistical analyses cigarette-smoking habits were taken into account using the pack-years (cigarette packs per day × years of smoking). However, in order to correct for the amount of nicotine containment in various types of cigarettes smoked (i.e., light, heavy, very heavy), we assigned a weight in each different type of cigarette pack, using the 0.8 mg/cigarette as the standard.
Consumption of non-refined cereals and products, vegetables, legumes, fruits, olive oil, dairy products, fish, pulses, nuts, potatoes, eggs, sweets, poultry, red meat and meat products were measured as an average per week during the past year through a validated food frequency questionnaire (FFQ) [14]. The frequency of consumption was then quantified approximately in terms of the number of times a month a food was consumed. Alcohol consumption was measured by daily ethanol intake, in wineglasses (100 ml and 12% ethanol concentration). Based on the Mediterranean diet pyramid [15], we calculated a special diet score ranged from 0–55. Higher values of this score indicate adherence to the traditional Mediterranean diet, characterized by moderate consumption of fat and a high mono-unsaturated : saturated fat ratio), while lower values indicate adherence to the ‘Westernized’ diet.
Body mass index was calculated as weight (in kilograms) divided by standing height (in metres squared). Obesity was defined as body mass index > 29.9 kg/m2.
Statistical analysis
Continuous variables are presented as mean values ± standard deviation, while qualitative variables are presented as absolute and relative frequencies. Associations between categorical variables were tested by the use of contingency tables and the calculation of chi-squared test. Comparisons between normally distributed continuous variables and categorical variables were performed by the calculation of Student's t-test and one-way or multi-way analysis of co-variance (multi-way ANCOVA), after controlling for homoscedacity. The Kolmogorov–Smirnov criterion was used for the assessment of normality. In the case of asymmetric continuous variables the tested hypotheses were based on the calculations of non-parametric tests, such as Mann–Whitney and Kruskal–Wallis. Correlations between inflammation variables and physical activity levels were tested through multiple linear regression analysis after the adjustment for several potential confounders and interactions. Due to its skewed distribution C-reactive protein levels were log-transformed.
The odds ratio of being classified as having the metabolic syndrome with respect to physical activity status was evaluated through multiple logistic regression analysis, after taking into account the effect of various potential confounders. Deviance residuals were calculated for the evaluation of the predicted association models.
All reported P-values are based on two-sided tests and compared to a significance level of 5%. However, due to multiple comparisons within a test we used the Bonferroni correction in order to account for the increase in type I error. SPSS 11.0.5 software (SPSS Inc. 2003, Chicago, Illinois, USA) was used for all the statistical calculations.
Results
Physical activity and metabolic syndrome
The population of the study was divided into those who fulfilled the criteria for the metabolic syndrome (n = 701) and in to those who did not fulfil the ATP III criteria (n = 2341). Of the non-metabolic syndrome group, 56% of men and 58% of women were classified as sedentary, while in the metabolic syndrome group 58% of men and 72% of women were defined as sedentary. Table 1 presents the investigated characteristics of the participants according to their physical activity status. No significant interaction between sex and physical activity status was observed regarding the presence of the metabolic syndrome (P = 0.83). Therefore the following analyses will be only age-adjusted and not stratified by gender.
Table 2 presents the components of the metabolic syndrome by physical activity status, in both groups of the study. Physical activity was associated with a lower prevalence of high waist circumference in non-metabolic syndrome participants, and with higher HDL-cholesterol levels in both metabolic and non-metabolic syndrome subjects. No other significant associations were observed between physical activity and components of the metabolic syndrome in both groups of the study.
Demographic and behavioural characteristics by physical activity status
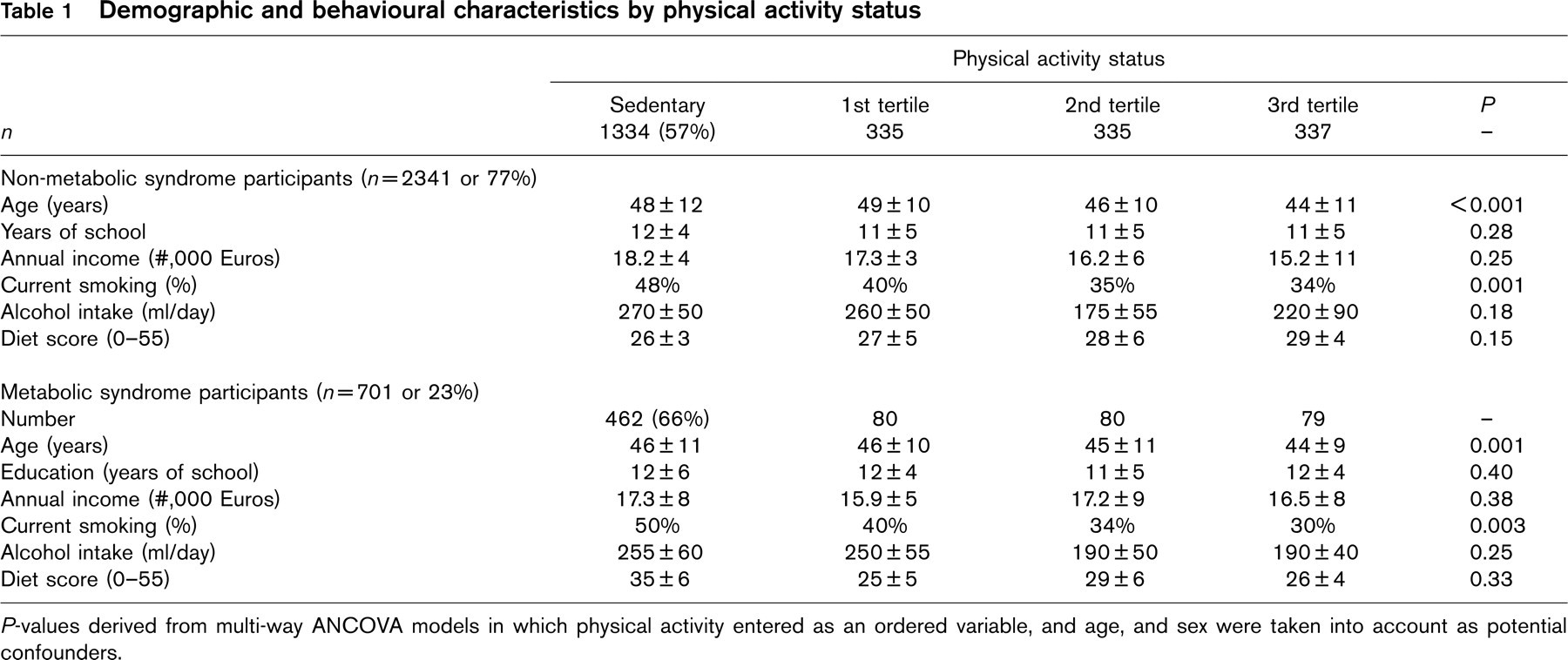
P-values derived from multi-way ANCOVA models in which physical activity entered as an ordered variable, and age, and sex were taken into account as potential confounders.
Physical activity and inflammatory and coagulation markers
People who had the metabolic syndrome had higher values of all the investigated biomarkers compared to people without the metabolic syndrome (Table 3). This trend was observed across all tertiles of physical activity, but did not reach statistical significance. Regarding physical activity and inflammatory and coagulation markers, unadjusted analysis revealed a decreasing trend across tertiles of physical activity in all biomarkers, both in metabolic and non-metabolic syndrome groups (Bonferroni α∗ < 0.05). It is notable that the significant reduction in the investigated markers was observed even in the moderate physical activity group (second tertile) in both the metabolic and non-metabolic syndrome participants (Table 3). Moreover, when we combined the physical activity groups and compared them with the sedentary group, we observed that metabolic syndrome individuals who were reported to be physically active had 36% lower levels of CRP, 15% lower levels of white blood cell counts, 19% lower levels of SAA, 15% lower levels of TNF-α, 30% lower levels of interleukin-6, and 15% lower levels of fibrinogen (all P< 0.05). Similar reductions were observed in the non-metabolic syndrome group, namely, 36% lower levels of CRP, 15% lower levels of white blood cell counts, 19% lower levels of SAA, 15% lower levels of TNF-α, 30% lower levels of interleukin-6 and 15% lower levels of fibrinogen (all P < 0.05).
No significant interactions were observed on the investigated biomarkers between physical activity status, group of study (i.e., metabolic or non-metabolic syndrome) and (a) the type of exercise, namely resistance or endurance (F-test for the interaction = 0.70, P = 0.85); and (b) the educational (F-test for the interaction = 0.65, P = 0.7) or the financial status of the participants (F-test for the interaction = 0.9, P = 0.4).
Components of the metabolic syndrome and physical activity status
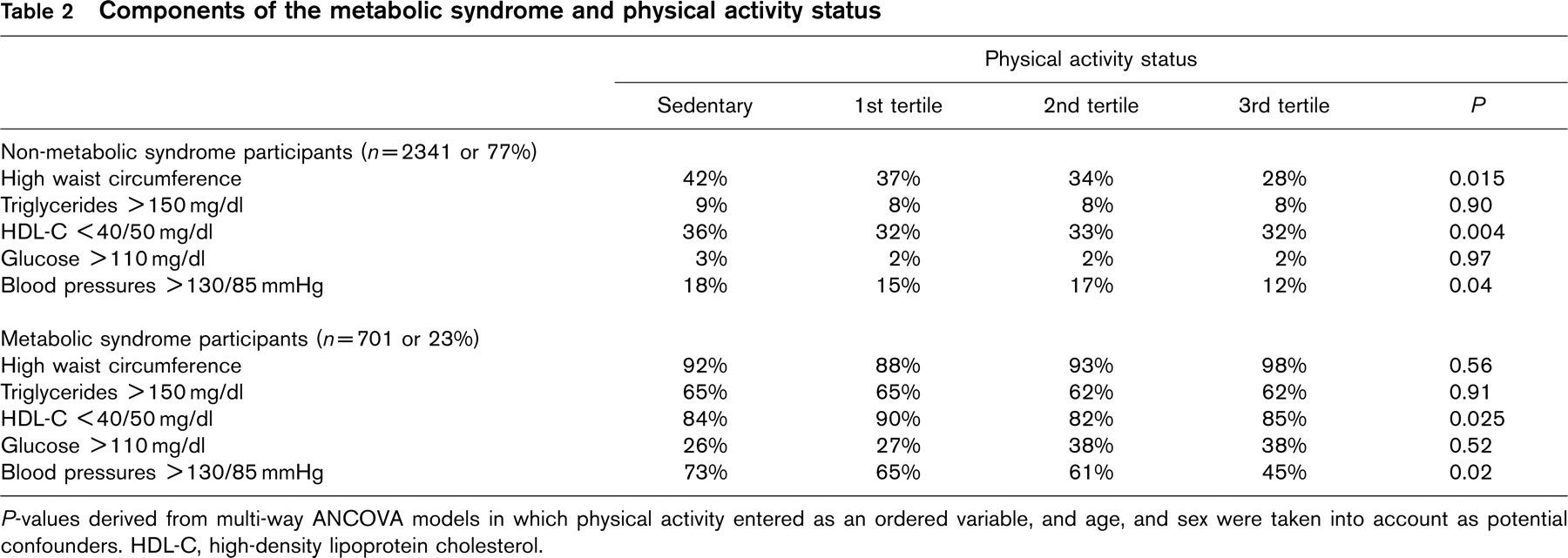
P-values derived from multi-way ANCOVA models in which physical activity entered as an ordered variable, and age, and sex were taken into account as potential confounders. HDL-C, high-density lipoprotein cholesterol.
Inflammatory markers and physical activity status in metabolic and non-metabolic syndrome participants
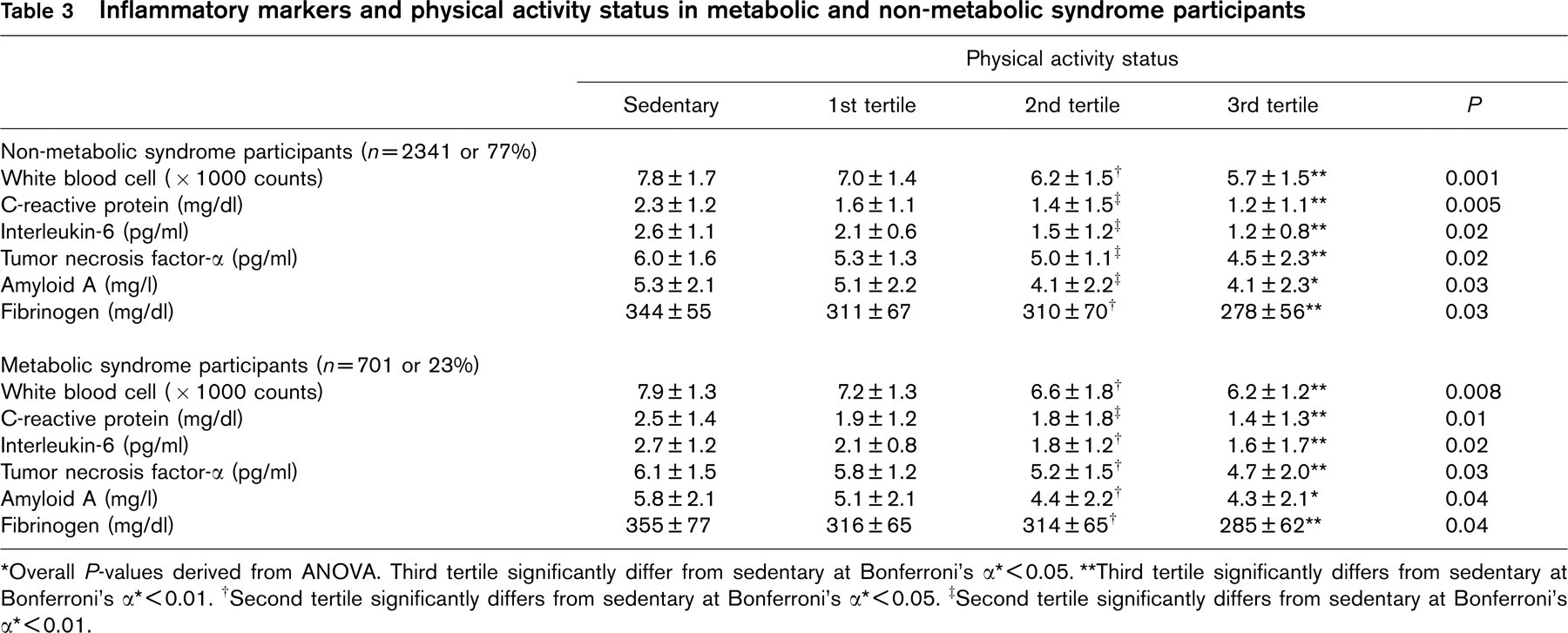
∗ Overall P-values derived from ANOVA. Third tertile significantly differ from sedentary at Bonferroni's α∗ <0.05.
∗∗ Third tertile significantly differs from sedentary at Bonferroni's α∗ <0.01.
† Second tertile significantly differs from sedentary at Bonferroni's α∗ <0.05.
‡ Second tertile significantly differs from sedentary at Bonferroni's α∗ <0.01.
Since many confounding factors may alter the previous results we performed multiple regression analysis after adjustments for gender, age, pack years of smoking, years of schooling, waist circumference, total- and HDL-cholesterol, blood glucose and systolic and diastolic blood pressure levels, alcohol consumption and dietary habits of the participants. We revealed that compared to sedentary individuals, metabolic syndrome participants who were classified in the highest tertile of the physical activity group had significantly lower levels of C-reactive protein (P < 0.001), interleukin-6 (P < 0.001), fibrinogen (P < 0.001), tumour necrosis factor-α (P = 0.03), amyloid A (P = 0.03), and white blood cell (P = 0.04). Moreover, compared to sedentary individuals, participants without the metabolic syndrome who were classified in the highest tertile of physical activity had significantly lower levels of C-reactive protein (P < 0.001), interleukin-6 (P < 0.001), fibrinogen (P < 0.001), tumour necrosis factor-α (P = 0.02), amyloid A (P = 0.02), and white blood cell (P = 0.03). Significant associations were also observed when we compared participants who were classified in the moderate exercise group (second tertile) against the sedentary group (Fig. 1) (a) in all investigated markers in people without the metabolic syndrome (all P's < 0.05), and (b) in C-reactive protein (P = 0.04) and fibrinogen (P = 0.04), in people with the metabolic syndrome. Figure 1 illustrates the results from multiple regression analysis as standardized beta coefficients, in order to allow for comparisons between the different biological factor levels. It is important to underline that the previous findings were independent from the components of the metabolic syndrome, as well as from the dietary and smoking habits of the participants.
Discussion
Our results reveal that leisure time physical activity was associated with a 15–36% lower level of inflammatory and coagulation markers compared to sedentary individuals in people with the metabolic syndrome. The latter findings were independent from known confounding factors, including the components of the syndrome. The beneficial effect of exercise on the investigated biomarkers was comparable to the effect observed in non-metabolic syndrome participants.
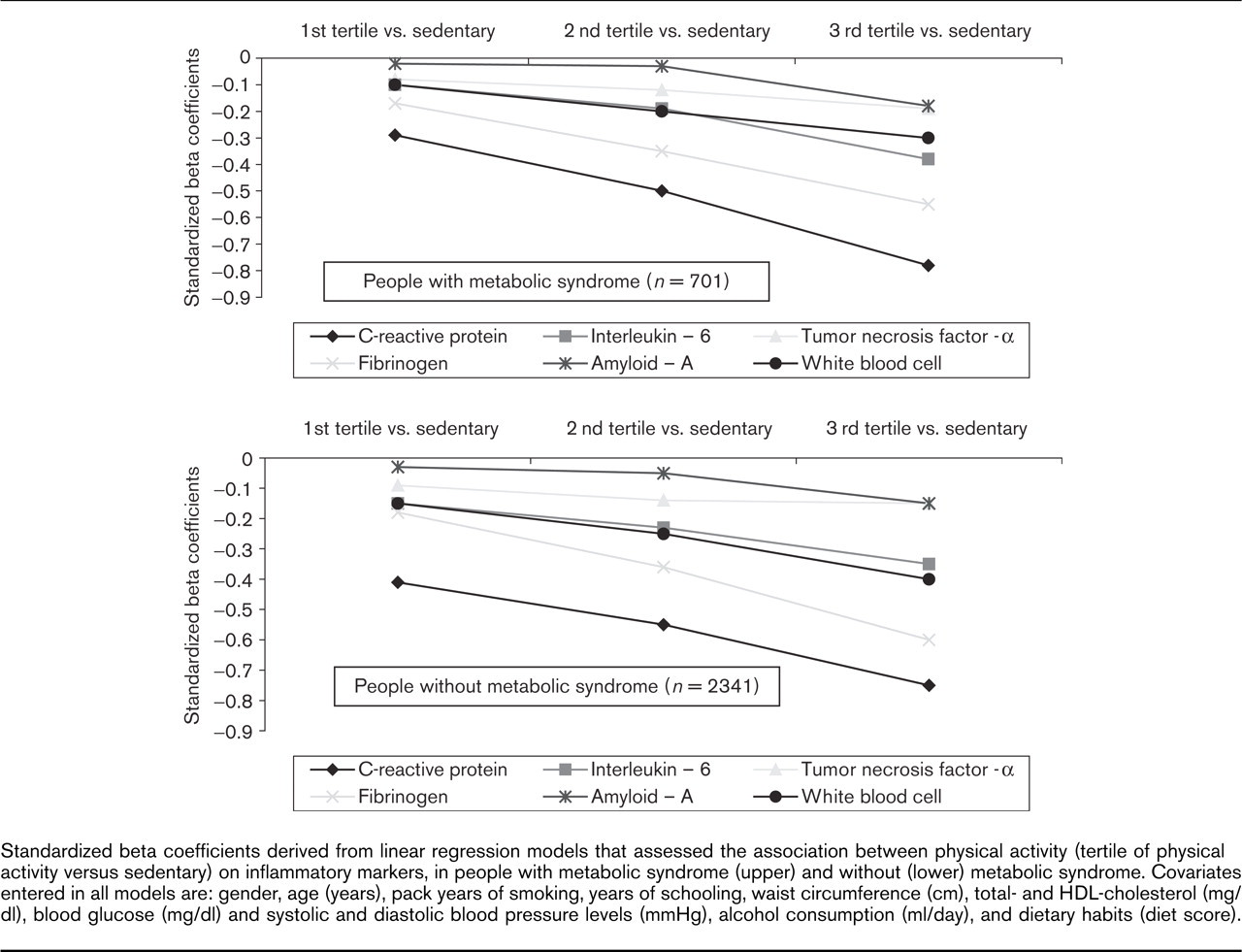
Standardized beta coefficients derived from linear regression models that assessed the association between physical activity (tertile of physical activity versus sedentary) on inflammatory markers, in people with metabolic syndrome (upper) and without (lower) metabolic syndrome. Covariates entered in all models are: gender, age (years), pack years of smoking, years of schooling, waist circumference (cm), total- and HDL-cholesterol (mg/dl), blood glucose (mg/dl) and systolic and diastolic blood pressure levels (mmHg), alcohol consumption (ml/day), and dietary habits (diet score).
The health benefits of physical activity are well recognized. Numerous observational and clinical studies have shown that the risk of coronary heart disease mortality or morbidity is inversely related to the level of physical activity [1–8]. The protective role of physical activity on the cardiovascular system is, at least in part, attributed to the favourable effects of exercise on several ‘traditional’ coronary risk factors, like blood pressure levels and body mass index [1, 2]. Low fitness has been associated with higher metabolic and other disturbance levels, which are diagnostic criteria for metabolic syndrome [16–18]. Physical activity, together with a healthy diet, is one of the most important components of therapy in metabolic syndrome with a positive effect on almost all metabolic disturbances characteristic for this syndrome [11, 19].
We observed a consistent inverse association of physical activity with several inflammatory and coagulation markers related to cardiovascular disease, in both the metabolic and non-metabolic syndrome groups. In addition, we revealed that even moderate amounts of physical activity could have a profound and favourable effect on these inflammatory and coagulation markers. These findings have clinical as well public health significance, since the moderate intensity and amount of physical activity is well tolerated by most middle-aged and older individuals and has a relatively low risk [3]. Moreover, our findings are in agreement with the reports by Ford [20] and King et al. [21] in healthy adults. In particular, they observed that the time devoted to physical activity was inversely associated with CRP levels, as well as with both plasma fibrinogen concentration and white blood cell count, after adjusting for several potential confounders. In contrast, Pischon et al. [22] reported that the association between physical activity and inflammatory markers was lost after adjusting for BMI and leptin. However, all these studies were based on population samples and not in people with the metabolic syndrome. To the best of our knowledge very few studies have shown an effect of physical activity on inflammatory and coagulation markers in people with the metabolic syndrome. Moore and colleagues [23] have shown that physical activity is associated with lower agreeability and adhesivity of platelets, activation of the fibrinolytic system and higher concentration of tissue plasminogen activator, which is inhibited in metabolic syndrome. Aronson et al. [24] reported that fasting glucose was significantly and positively associated with plasma CRP in middle-aged subjects, suggesting that a pro-inflammatory effect may contribute to the adverse cardiovascular outcome associated with diabetes, impaired fasting glucose, and increasing glucose levels within the normal range. Moreover, Temelkova-Kurktschiev et al. [25] reported that sub-clinical inflammation was a strong predictor of cardiovascular events and could be suggested to be a part of the metabolic syndrome. Recently we showed that pre-hypertension status is associated with the inflammation process among healthy adults from the ATTICA study [26]. Therefore we could speculate that since physical activity plays a role in the inflammation process among healthy individuals, and components of the metabolic syndrome are associated with pro-inflammatory markers, the presence of physical activity may reduce, at least in part, the prevalence of the metabolic syndrome through the modification of inflammatory and coagulation marker levels.
Limitations
All blood chemistries were evaluated once. Although we made an effort to follow the World Health Organization guidelines for biochemical analyses the reported number of participants with the metabolic syndrome may be under- or overestimated. The presence of occupational physical activity was recorded, but was not taken into account for the analysis due to difficulties in evaluation and standardization. This exclusion may confound our findings, but the large sample size and the randomised procedure for the selection of the participants can spread the subjects who reported occupational exercise equally in both groups of the study. Another limitation is that leisure time physical activities have been related to healthier lifestyle habits and consequently to a better health status. For example, adoption of a healthier dietary pattern or reduced smoking habits may be more common among individuals who were devoted to leisure time exercise. Although we took into account the dietary and smoking habits of the participants the influence of these potential confounders cannot entirely be excluded due to misreporting. Finally, this is a cross-sectional study that cannot provide evidence for causality but only generate hypotheses. A randomized trial in people with the metabolic syndrome would confirm or refute our findings regarding the association of exercise on the inflammation process.
Conclusion
We extended the current scientific knowledge of the association between exercise and cardiovascular disease, illustrating that physical activity is associated with lower inflammatory and coagulation factor levels in people with the metabolic syndrome. Moreover, the association of physical activity on the investigated pro-inflammatory biomarkers was similar to the one observed in people without the syndrome. Because atherosclerotic vascular disease has been associated with inflammation and coagulation, the adoption of lifestyle habits that have pathobiologic, prognostic and treatment-related relevance should take a role of considerable importance, especially in high-risk individuals. Despite the known limitations of the cross-sectional design, our findings have an additional public health impact, since moderate levels of physical activity can be well tolerated by most people with minimal risk for injury.
Footnotes
Acknowledgements
The ATTICA study is funded by research grants from the Hellenic Society of Cardiology. The authors would like to thank the field investigators of the ‘ATTICA’ study: Dr John Skoumas (principal field investigator), Dr Natasa Katinioti (physical examination), Dr Spiros Vellas (physical examination), Dr Efi Tsetsekou (physical/psychological evaluation), Dr Dina Masoura (physical examination), Dr Lambros Papadimitriou (physical examination), as well as the technical team: Dr Marina Toutouza (biochemical analysis), Ms Carmen Vasiliadou (genetic analysis), Mr Manolis Kambaxis (nutritional evaluation), Ms Konstadina Paliou (nutritional evaluation), Ms Chrysoula Tselika (biochemical evaluation), Ms Sia Poulopoulou (biochemical evaluation) and Ms Maria Toutouza (database management).