
Abstract
Background
Design
Results
Conclusion
Introduction
Approximately 47 million adults in the US have metabolic syndrome (MetS), an important risk factor for the subsequent development of diabetes and cardiovascular disease (CVD)[1]. According to the current National Heart, Lung, and Blood Institute (NHLBI) and American Heart Association (AHA) definition, MetS is characterized by the presence of any three of the following: increased waist circumference (WC), increased triglycerides, low high-density lipoprotein (HDL), increased blood pressure (BP), and elevated fasting glucose levels [2, 3].
The management of MetS consists of a two-pronged approach of maintaining a healthy weight and increasing physical activity. Previous small studies have shown that physical activity may be protective against MetS independent of weight loss and change in body composition [4–6]. Some retrospective studies have shown an improvement in the components of MetS with moderate weight reduction [7]. In this study, we seek to determine the relative strength relationship between these two major determinants and the development of incident MetS in a population-based sample of middle-aged Americans.
Materials and methods
Study population
We obtained the public use data from the Atherosclerosis Risk in Communities (ARIC) study, a population-based cohort study of arteriosclerotic CVD sponsored by the NHLBI [8, 9], which was designed to look into the cause and natural history of atherosclerosis and its risk factors by race, sex, location and date. Population-based samples of 15 792 residents aged 45-64 years in four US communities in North Carolina, Mississippi, Minnesota, and Maryland were examined and reviewed by institutional review boards. These participants were re-examined every 3 years with the first screen (baseline) occurring in 1987-1989, and the third in 1993-1995. The response rate for this study was about 75-80%.
Of the baseline cohort of 15 792 individuals, we identified 9359 individuals who were free of MetS at baseline as our study population. We identified characteristics in 7854 individuals during their third cohort clinical examination, which formed the sample size for this study.
Classification of metabolic syndrome status
MetS is defined according to the revised Adult Treatment Panel III criteria, adopted by NHLBI and AHA, as the presence of three or more of the following components: (i) elevated BP: systolic BP ≥ 130 mmHg, diastolic BP ≥ 85 mmHg, or use of antihypertensive medications; (ii) elevated plasma glucose: fasting glucose ≥ 100 mg/dl (5.56 mmol/l), self-reported physician diagnosed diabetes, or current use of hypoglycemic agent or insulin; (iii) elevated serum triglycerides ≥ 150mg/dl (1.7mmol/l); (iv) decreased HDL-cholesterol: ≤ 40mg/dl (1.0mmol/l) for men and ≤ 50 mg/dl (1.3mmol/l) for women; and (v) greater WC: 102 cm (40 inch) for men and 88 cm (35 inch) for women [10, 11].
Obesity and physical activity
Baseline obesity was assessed using current Center for Disease Control body mass index (BMI) criteria: BMI less than 25 kg/m2 as normal weight, 25-29 kg/m2 as overweight, and ≥ 30 kg/m2 as obese. The leisure-time physical activity index was obtained in the ARIC study through the application of Baecke Physical Activity Questionnaires. For this analysis, we focused on leisure-time physical activity, which captures time spent viewing television (negative score), bicycling, walking, and time spent walking and bicycling to and from work or shopping. These responses were given a leisure-time physical activity score, ranging from 1 (low activity) to 5 (high activity), with 0.25 unit of increments [8]. For this analysis, we further subdivided the leisure-time physical activity into three categories using the tertile distribution - lowest tertile (1.00-2.00), middle tertile (2.25-2.50), and upper tertile (≥ 2.75).
Other covariates
Baseline demographic variables and risk factors for coronary heart disease (CHD) were assessed according to standardized protocols [12, 13]. These covariates include age, race, sex, education level, cigarette smoking status, prevalence of CHD and total cholesterol.
Statistical methods
The relationship between the incident MetS and obesity and physical activity was assessed using logistic regression models with adjustments for sample weights. The odds ratio and its 95% confidence interval (95% CI) were used to assess the strength of associations. All analyses were performed with SAS software (SAS institute Inc, Cary, North Carolina, USA)[14].
Results
Baseline characteristics
Baseline characteristics are presented in Table 1 for the entire study population and by 6-year incident MetS status. The mean age of the entire cohort at baseline was 53.5 years, with 56% female, and 21% African-American.
We used logistic regression models to estimate the odds ratios and the 95% CIs of 6-year incident MetS in relationship to baseline obesity and leisure-time physical activity. These results are presented in Table 2, from an unadjusted model (Model 1 in Table 2), and multivariable adjusted model (Model 2 in Table 2), and a model with both obesity and physical activity as independent variables (Model 3 in Table 2). As seen in Table 2, the incidence of MetS doubled in overweight groups and tripled in the obese group, with odds ratio of 2.81 (95% CI: 2.50-3.17) and 5.24 (95% CI: 4.50-6.12), respectively, from the unadjusted model. In individuals with a leisure-time physical activity in the upper tertile or in the middle tertile, the incidence of MetS was reduced with an odds ratio of 0.80 (95% CI: 0.71-0.91) and 0.92 (95% CI: 0.81-1.04), respectively from the unadjusted model. The baseline obesity and physical activity relationship with the incident MetS remain unchanged after adjusting for baseline covariables, including age, sex, race, education, current smoking, total cholesterol, and history of CHD. Furthermore, after additional adjustment for physical activity (Model 3), the baseline obesity and incident MetS relationship remained unchanged. There was significant graded increased risk of incident MetS with the increased level of obesity measures. However, after adjusting for obesity, the association between baseline physical activity and incident MetS was diminished towards a non-significant association, although the point estimates remain protective (odds ratio less than one with increased level of physical activity).
Baseline characteristics (mean, SD, or proportion) of study population
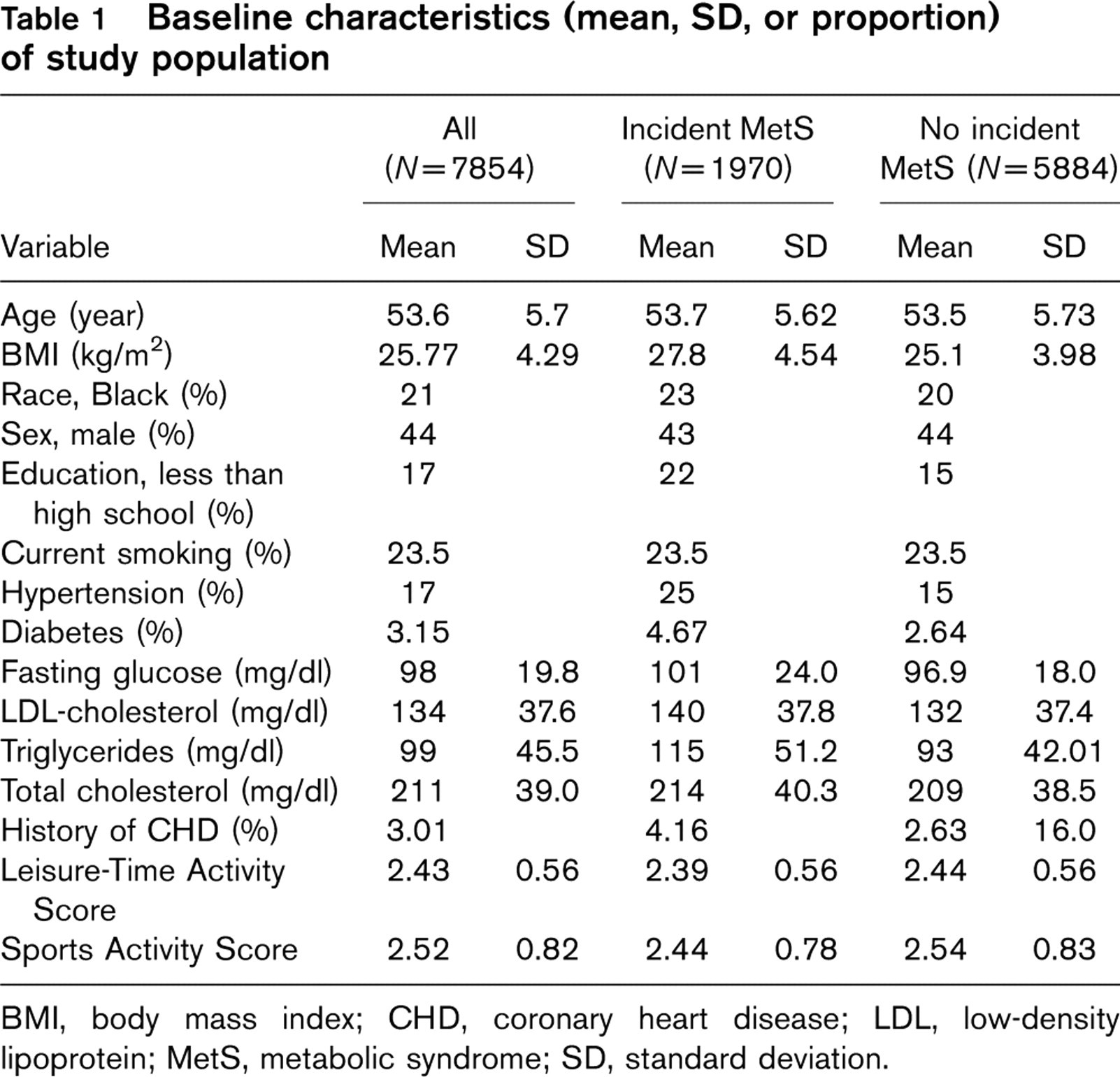
BMI, body mass index; CHD, coronary heart disease; LDL, low-density lipoprotein; MetS, metabolic syndrome; SD, standard deviation.
Association between obesity categories, leisure-time physical activity tertiles, and the 6-year incidence of metabolic syndrome
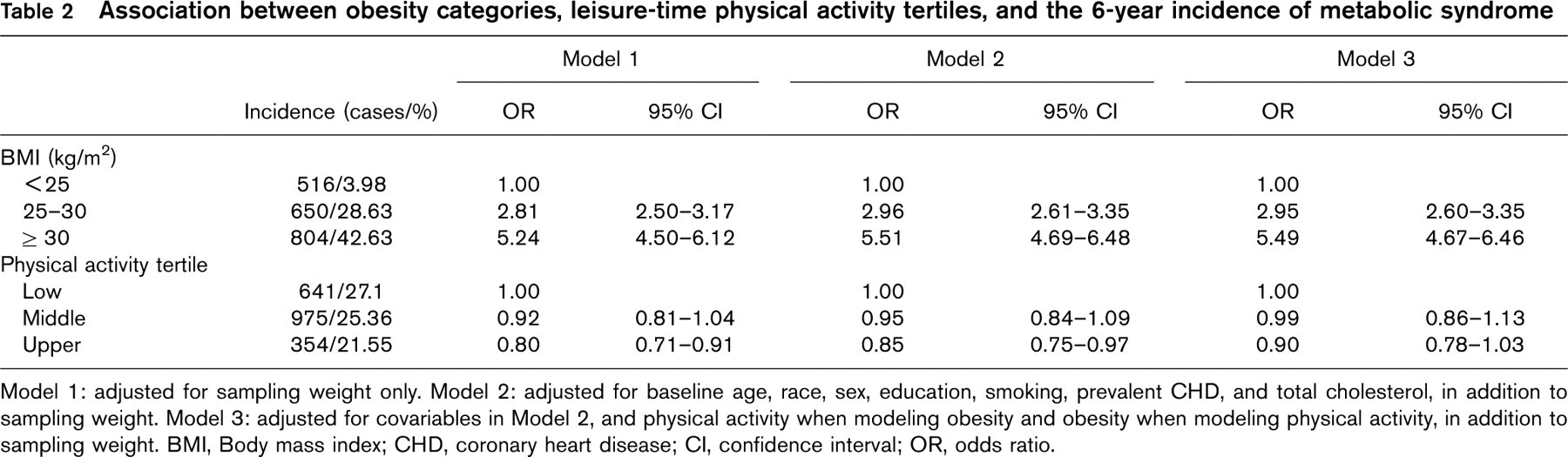
Model 1: adjusted for sampling weight only. Model 2: adjusted for baseline age, race, sex, education, smoking, prevalent CHD, and total cholesterol, in addition to sampling weight. Model 3: adjusted for covariables in Model 2, and physical activity when modeling obesity and obesity when modeling physical activity, in addition to sampling weight. BMI, Body mass index; CHD, coronary heart disease; CI, confidence interval; OR, odds ratio.
To determine which of the baseline factors (obesity or physical activity) is a better predictor of MetS, we examined the interaction between obesity and physical activity measures, and calculated the odds ratios and their 95% CI for the nine different combinations of obesity categories (normal weight, overweight, and obese) and physical activity tertiles (lowest, middle, and upper tertiles). These data are presented in Table 3, and the point estimates (the incident odds ratios of MetS) are graphically presented in Fig. 1. Table 3 and Fig. 1 both indicated that with BMI increases, the odds ratio for developing MetS significantly increases at all levels of physical activity, especially among obese patients (with an odds ratio greater than 5). At any level of physical activity, an increase in BMI corresponds with a clear dose-response increase in odds ratio, and the 95% CIs within a physical activity level do not overlap. In contrast, at any given level of BMI, there are no statistically significant changes in the odds ratio at different levels of physical activity and the 95% CI overlaps, except for the normal BMI group where there is a graded increased odds ratio with the decrease in physical activity levels. However, the magnitude of odds ratios clearly indicated a much stronger association from BMI measures than from leisure-time physical activity measures.
Discussion
In this population-based data, we found that obesity was strongly associated with the development of incident MetS, and leisure-time physical activity was weakly associated with incident MetS. After adjusting for each obesity and leisure-time physical activity, our findings clearly suggest that obesity is strongly associated with the development of incident MetS whereas physical activity is weakly associated with it. Even when adjusting for potential confounders such as age, sex, race, level of education, total cholesterol, history of CHD, and smoking status, obesity was a strong predictor of incident MetS than physical activity. These results highlight the need to target obesity more than physical activity to prevent the development of MetS in the general population. Although previous studies have shown that both these strategies as a solution for betterment of community health [15], the clinical implication of our study is that instead of following the dual strategy of reducing obesity and engaging in regular physical activity, it may be more beneficial for patients to focus on weight loss. Some studies have also shown that an intervention like physical activity can change the parameters of MetS and can also decrease the inflammatory markers [16, 17].
Joint effect of obesity categories and leisure-time physical activity tertiles on the 6-year incidence of metabolic syndrome
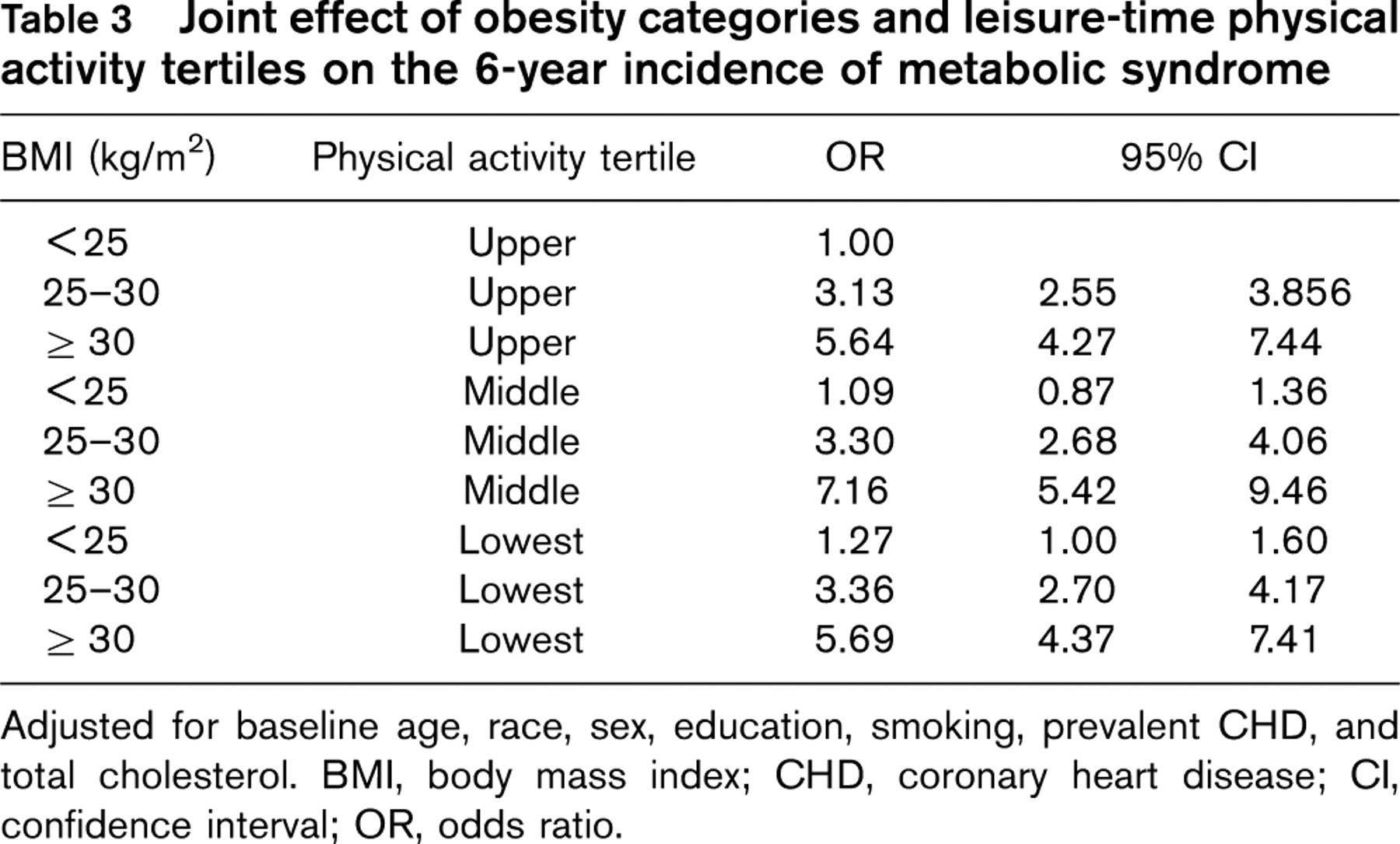
Adjusted for baseline age, race, sex, education, smoking, prevalent CHD, and total cholesterol. BMI, body mass index; CHD, coronary heart disease; CI, confidence interval; OR, odds ratio.
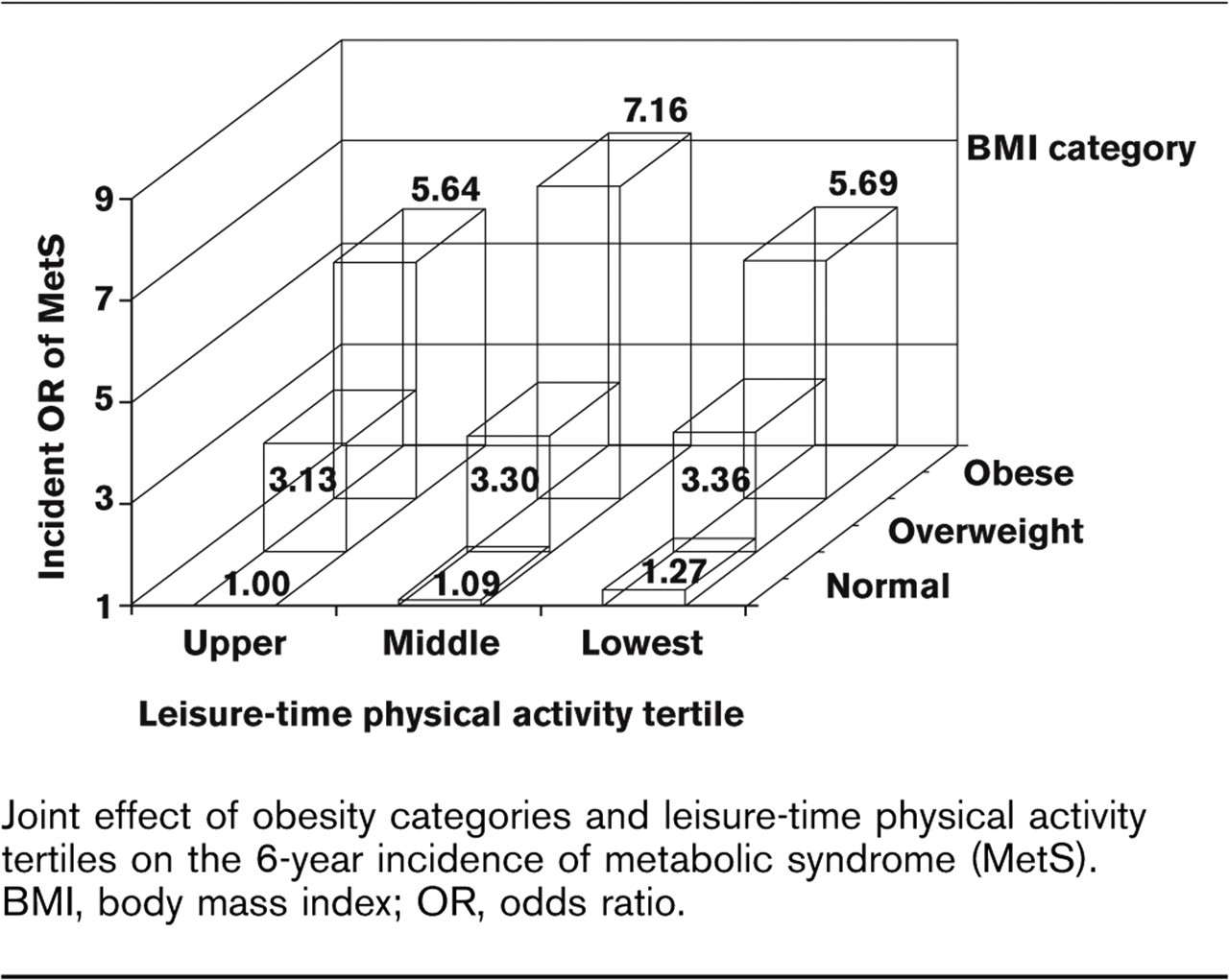
Joint effect of obesity categories and leisure-time physical activity tertiles on the 6-year incidence of metabolic syndrome (MetS). BMI, body mass index; OR, odds ratio.
Our study population was free of MetS at baseline. Since the varied components, which comprise the clinical definition of MetS have been closely linked to each other, it makes logical sense that WC and BMI would be highly correlated, which our study confirms. It is worth noting that we also performed the entire analysis excluding persons with baseline WC greater than the MetS-increased WC [WC ≥ 102 cm (40 inch) for men and ≥ 88 cm (35 inch for women)]. In this scenario, the pattern of associations from both obesity and leisure-time physical activity did not change meaningfully (data not shown). Therefore, the strong association between obesity and MetS observed in this study does not seem to be affected by our inclusion of individuals who have a large WC but did not otherwise meet the MetS criteria.
Several groups have proposed different definitions for MetS diagnosis criteria, including the WHO [18], the European Group for the Study of Insulin Resistance [19], US Adult Treatment Panel III of the National Cholesterol Education Program [2, 3], the American Association of Clinical Endocrinology [20], the International Diabetes Federation [21], and the AHA/NHLBI [8, 9]. We used the least stringent definition of MetS as characterized by Adult Treatment Panel III. However, the ARIC study is comprehensive, with a bi-racial cohort, large sample size and long enough follow-up time to be a representative study population. One may argue that the more subjective Baecke Physical Activity Questionnaire is not as reliable and valid as compared with more objective measures, such as energy expenditure (kJ/min), oxygen consumption (l/min or ml/min per kg), or metabolic activity relative to resting conditions (MetS). In contrast, the Baecke Questionnaire has been validated by other studies [22] and it is important to note that in the ARIC study, leisure-time physical activity assessed by the Baecke Questionnaire has been consistently shown to be predictive of cardiovascular events [8, 9].
In this middle-aged US population-based sample, the 6-year incidence of MetS was 25%, which is comparable with the MetS prevalence of 24% among adults in the US [1]. As MetS can result in type 2 diabetes and arteriosclerotic CVD [10, 11, 23, 24], which is the leading cause of death in the US and other developed countries, this study contains many implications for public health officials concerned about the obesity epidemic.
If physicians are able to identify groups with MetS as a possible precursor to diabetes or CVD, they can act to prevent this progression to disease at an earlier stage [25]. Clinicians can advise these patients that managing weight is a priority for an individual with MetS. Studies have shown that favorable metabolic changes are observed in obese patients with mild reduction in weight. This is attributed to sympathetic nervous system activation leading to preferential reduction in visceral fat mass [26]. Methods to prevent weight gain include assessing diet using a daily journal or speaking with a nutritionist about guidelines for healthy eating [12]. Physicians can also counsel patients about their attitudes about lifestyle choices that are causing weight gain and how to improve these behaviors [12]. Stone [12] describes several important strategies based on the Obesity Guidelines Panel from the National Institutes of Health report including (i) multistep strategies work better than a single approach and (ii) motivation increases as reasonable goals are set.
The major strengths of this study are a large number of African-American participants, detailed dietary habits and atherosclerotic disease pattern, which can be projected into US population. The other strengths are simple design, prospective study, large number of patients with potentially confounding variables, and extensive follow-up time. The limitations are use of self-reported physical activity, which can lead to bias. The other limitations are lack of Hispanic representation and a limited number of questions in the study regarding physical activity.
Conclusion
Obesity remains a national concern, affecting 65% of adults and 17% of children in the US and is growing to be a worldwide issue [13, 27]. This population-based data indicates that body weight is a more important determinant than leisure-time physical activity in the development of MetS. Thus, assessing obesity by BMI and treating overweight and obese patients are important goals in curbing this crisis [28–31]. Reducing body weight by an achievable amount of 5-10% would significantly improve the prognosis for patients with MetS [13]. As obesity is an important indicator for the development of MetS, targeting this should remain a focus for public health officials.
Footnotes
Acknowledgements
The ARIC Study is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with the ARIC Investigators. The authors thank the NHLBI for providing the public use data for this investigation. The authors thank the staff and participants of the ARIC study for their important contributions. We also thank Laurie Schwing, MLS, for advice, guidance and editorial support for this project. The authors did not receive any source of funding for this project from anyone. There is no conflict of interest to report.