
Abstract
Background
Fitness and obesity are both independently associated with cardiovascular events and mortality. C-reactive protein (CRP), a predictor of cardiovascular events is associated with obesity; but its association with cardiorespiratory fitness in early adulthood is uncertain. The aim of this study was to examine the relationship between cardiorespiratory fitness and CRP, controlling for obesity in an unselected cohort of young adults.
Design
A cross-sectional study in a representative birth cohort.
Methods
We measured CRP levels, cardiorespiratory fitness, anthropometric variables, blood pressure and smoking in 26-year-old men (n=400) and women (n=315). Log CRP levels were compared across cardiorespiratory fitness with adjustment for body mass index (BMI), sex, blood pressure, smoking and combined oral contraceptive use.
Results
Geometric mean CRP levels were higher in women (3.23 mg/l, 95% CI 2.85–3.64) compared with men (1.70mg/l, 1.52–1.89). Regression analysis adjusting for sex and weight showed an inverse association between fitness and CRP (β= −0.16, P<0.001). This association held after statistical controls were added for BMI, systolic blood pressure and smoking and combined oral contraceptive use (P ≤ 0.01).
Conclusions
Cardiorespiratory fitness levels are inversely associated with CRP levels in young adults independent of obesity, blood pressure, smoking and combined oral contraceptive use in women. Physical fitness may decrease the risk of cardiovascular events by reducing inflammation.
Introduction
Low levels of fitness and physical activity are risk factors for all-cause and cardiovascular mortality [1, 2]. Physical activity is also inversely associated with C-reactive protein (CRP), a marker of systemic inflammation, in middle-aged and elderly individuals [3–7]. CRP has been shown to predict cardiovascular events in apparently healthy individuals [8–12], suggesting that atherothrombosis may be a chronic inflammatory disorder, in addition to being a disease of lipid accumulation [13]. Obesity is also associated with higher CRP levels [14, 15], and it has been proposed that the increased cardiovascular risk of obesity may be mediated by systemic inflammation [14].
Obesity and poor fitness appear to be independent risk factors for cardiovascular disease and mortality [16]. In middle-aged and elderly men and women obesity and poor fitness also appear to be independently related to CRP [17–21]. To address the hypothesis that physical fitness influences CRP levels independently of obesity in early adulthood, we evaluated the association between cardiorespiratory fitness and CRP, adjusting for body mass index (BMI) in an unselected cohort of young adults.
Methods
Sample
Participants are members of the Dunedin Multidisciplinary Health and Development Study, a longitudinal investigation of health and behaviour in an unselected birth cohort [22]. The study members were born in Dunedin, New Zealand, between April 1972 and March 1973. Of these, 1037 children (91% of eligible births; 52% male) participated in the first follow-up assessment at age 3 years, constituting the base sample for the remainder of the study. Cohort families represent the full range of socio-economic status in the general population of New Zealand's South Island, and are primarily white of European descent. Follow-ups have been carried out at ages 5, 7, 9, 11, 13, 15, 18, 21, and most recently at 26 years when we assessed 980 of the 1019 study members still alive (96%). The study was approved by the Otago Ethics Committee and participants gave written informed consent. At the age of 26 years assessment venepuncture was performed at the same time each day (between 1615 and 16 45 h). Ninety per cent (n = 882) consented to venepuncture, including 31 out of 33 who were pregnant. CRP data was available for 872 study members. Pregnant women (n = 31), those who refused the cardiorespiratory fitness or anthropometry assessments (n = 126) were excluded from the analysis, leaving complete observations for 715 study members (400 men and 315 women).
C-reactive protein
Non-fasting CRP was measured in venous blood on a Hitachi analyser using an immunoturbidimetric assay (Boehringer Mannheim, Mannheim, Germany). The coefficient of variation ranged from 5.6 to 12.9%. The lower sensitivity level of the assay was 1 mg/l.
Cardiorespiratory fitness
To assess cardiorespiratory fitness, study members completed a submaximal exercise test on a friction-braked cycle ergometer (Monark, Sweden). Depending upon the extent that heart rate increased during a 2-min 50 Watt warm-up, the workload was adjusted to elicit a steady heart-rate in the range 130–170 bpm. After a further 6-min constant power output stage the maximal heart rate was recorded and used to calculate predicted maximum oxygen consumption (VO2max; l/min) according to standard protocols [23].
Anthropometry
Height was measured in stocking feet to the nearest millimeter. Body weight was recorded using calibrated scales (Tanita, Tokyo, Japan, model no. 1609N) in light clothing to the nearest 0.1 kg. Waist girth was taken as the perimeter at the level of the noticeable waist narrowing located approximately half way between the costal border and the iliac crest, and was measured using a steel tape to the nearest millimeter. All measurements were taken twice and the mean of two readings was calculated. BMI was calculated as weight divided by height squared and was categorized as lean (≤ 24.9 kg/m2), overweight (25.0–29.9) and obese (≥ 30.0).
Blood pressure
The blood pressure assessment was conducted according to standard protocols [24] using a Hawksley random-zero sphygmomanometer with a constant deflation valve. Cuffs were chosen on the basis of the circumference of an individual's arm. Study members were seated in a quiet room with their right arm resting at heart level. A 5-min rest period preceded the first measurement, followed by two further measures 5 min apart. Systolic and diastolic blood pressure were calculated as the mean of the three measurements.
Smoking
Those who had smoked daily for a month or more during the previous year were considered smokers.
Statistical analysis
Because of the skewed nature of its distribution, data for CRP were log transformed for all analyses. To allow transformation of 0 values, 1 was added to CRP values before log transformation. T-tests and chi-squared tests were used to test differences between men and women. The association between log CRP and cardiorespiratory fitness, using fitness as a continuous variable, and BMI was tested using linear regression in men and women. We then estimated the association between predicted VO2max (l/min) and CRP controlling for sex and weight; and subsequently estimated the association controlling for BMI, systolic blood pressure, smoking, and combined oral contraceptive use. Statistical significance for all analyses was defined as P < 0.05.
Results
The geometric mean CRP was 1.70 mg/l in men and 3.23 mg/l in women (P < 0.001, Table 1). Women also had significantly lower fitness, waist circumference, systolic and diastolic blood pressure (all P < 0.001). BMI and smoking prevalence were similar for men and women.
Regression of log CRP on VO2max with the effect of sex and weight statistically controlled revealed a significant inverse association (coefficient = −0.16, SE = 0.04, P < 0.001). There was no significant fitness by sex interaction on CRP levels. However, as previous research had shown an association between the use of combined oral contraception and CRP [25] analyses were performed separately for men and women. For both men and women, regression analysis showed that geometric mean CRP decreased with increasing fitness (women, P < 0.001, men, P = 0.016) and increased with increasing BMI (women, P < 0.001, men, P = 0.009). For illustrative purposes, data are presented by sex, divided into thirds according to predicted VO2max adjusted for body weight (Table 2).
Mean (95% confidence interval) C-reactive protein, cardiorespiratory fitness, body mass index, blood pressure, percentage daily smoking, and combined oral contraceptive use of 26-year-old men and women
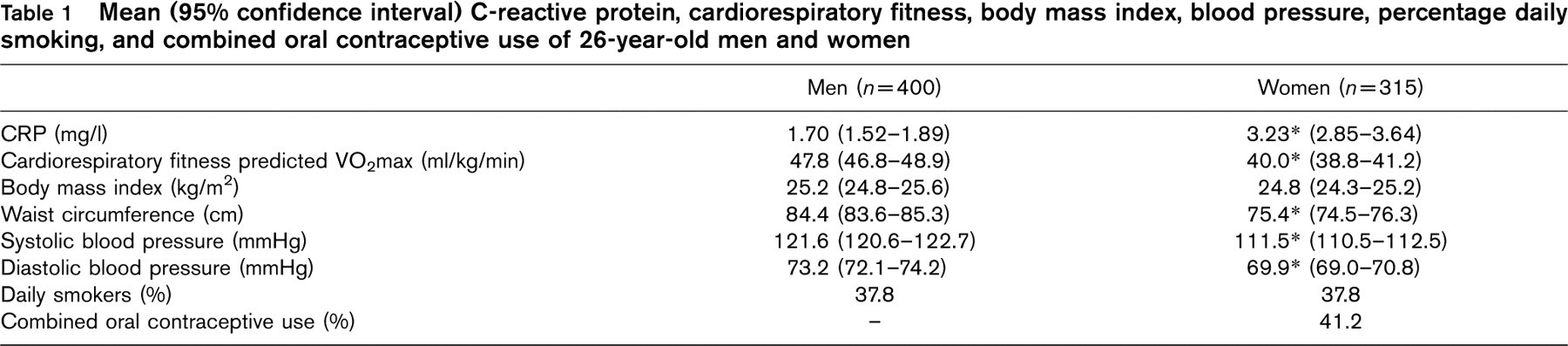
CRP, C-reactive protein (geometric mean); VO2max, maximum oxygen consumption.
∗ Differs from men at P<0.001.
Geometric mean C-reactive protein levels of men and women according to fitness and body mass index groups
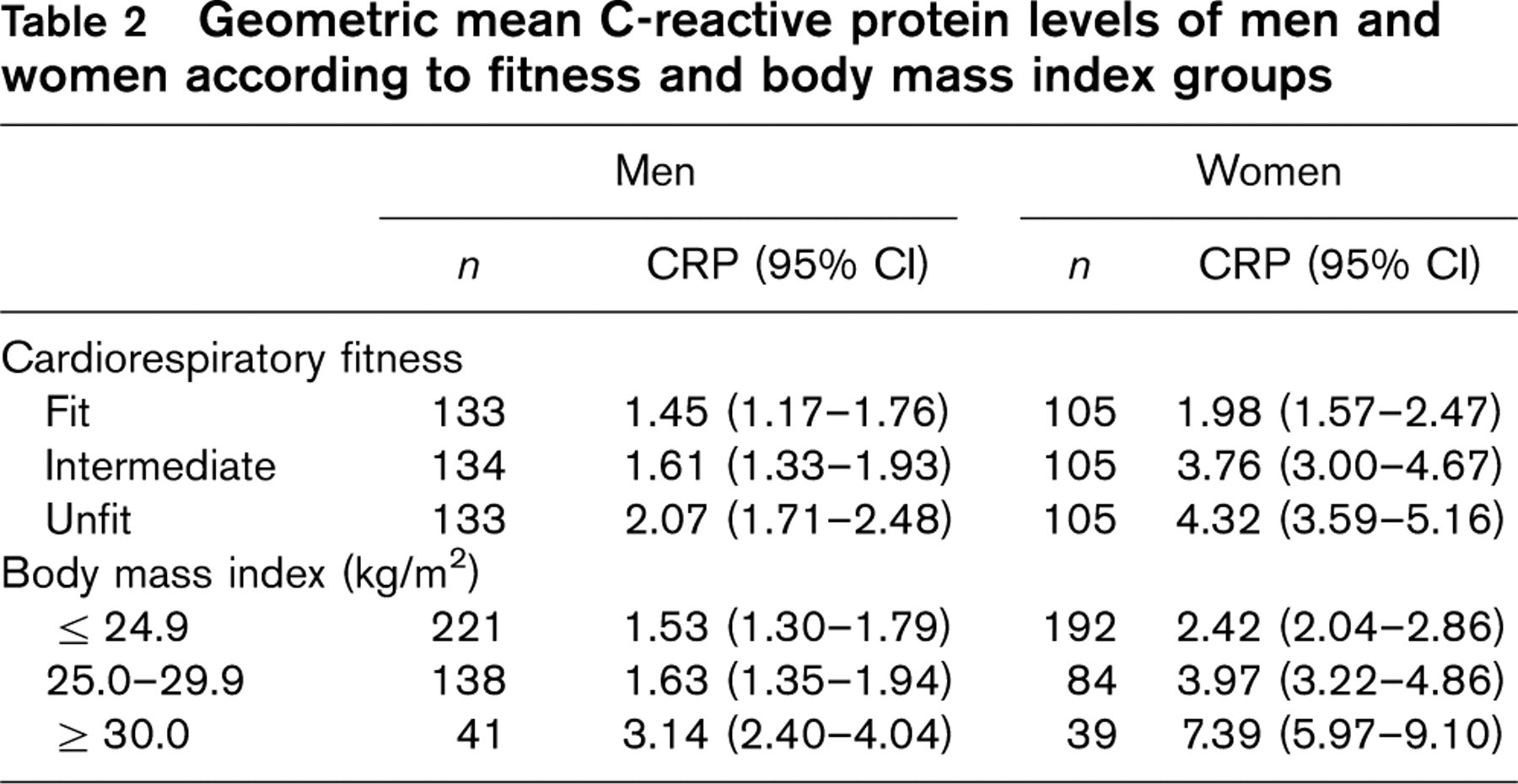
CI, Confidence interval; CRP, C-reactive protein levels reported as mg/l. Fitness is shown in terms of sex-specific thirds of cardiorespiratory fitness adjusted for body weight.
Multiple regression analyses of log CRP on VO2max, controlling for BMI, systolic blood pressure, smoking and combined oral contraceptive use for each sex, are shown in Table 3. For both men and women, there were inverse associations between fitness and log CRP after the effects of all other covariates were controlled (P = 0.01 and P = 0.009, respectively), and there were also positive associations between BMI and log CRP (P < 0.001). For men there was a negative association between systolic blood pressure and log CRP (P = 0.007), whereas for women there was a positive association between systolic blood pressure and log CRP (P = 0.007). For women there was also a positive association between combined oral contraceptive use and log CRP (P < 0.001). An analysis testing for an interaction between fitness and oral contraceptive use was not significant, implying that there was no difference in the relationship between fitness and log CRP in women using oral contraceptives compared with those not using oral contraceptives. The results did not change when multiple regression analyses were repeated with waist circumference substituted for BMI.
Discussion
This study has shown that physical fitness is inversely related to CRP levels in an unselected community cohort of young adults. This association was independent of measures of adiposity (BMI and waist circumference). Our findings are consistent with those of earlier reports [17–20, 26]. LaMonte et al. [18] reported a relationship between plasma CRP concentrations and physical fitness independent of BMI in 135 overweight middle-aged women. The present study extends these findings in a larger unselected community cohort of younger women with a lower mean BMI, and confirms the association after adjustment for other covariates known to influence CRP levels, including the use of combined oral contraceptives.
Association between log C-reactive protein and fitness for men and women, controlling for body mass index, systolic blood pressure, smoking, and combined oral contraceptive use (women only)
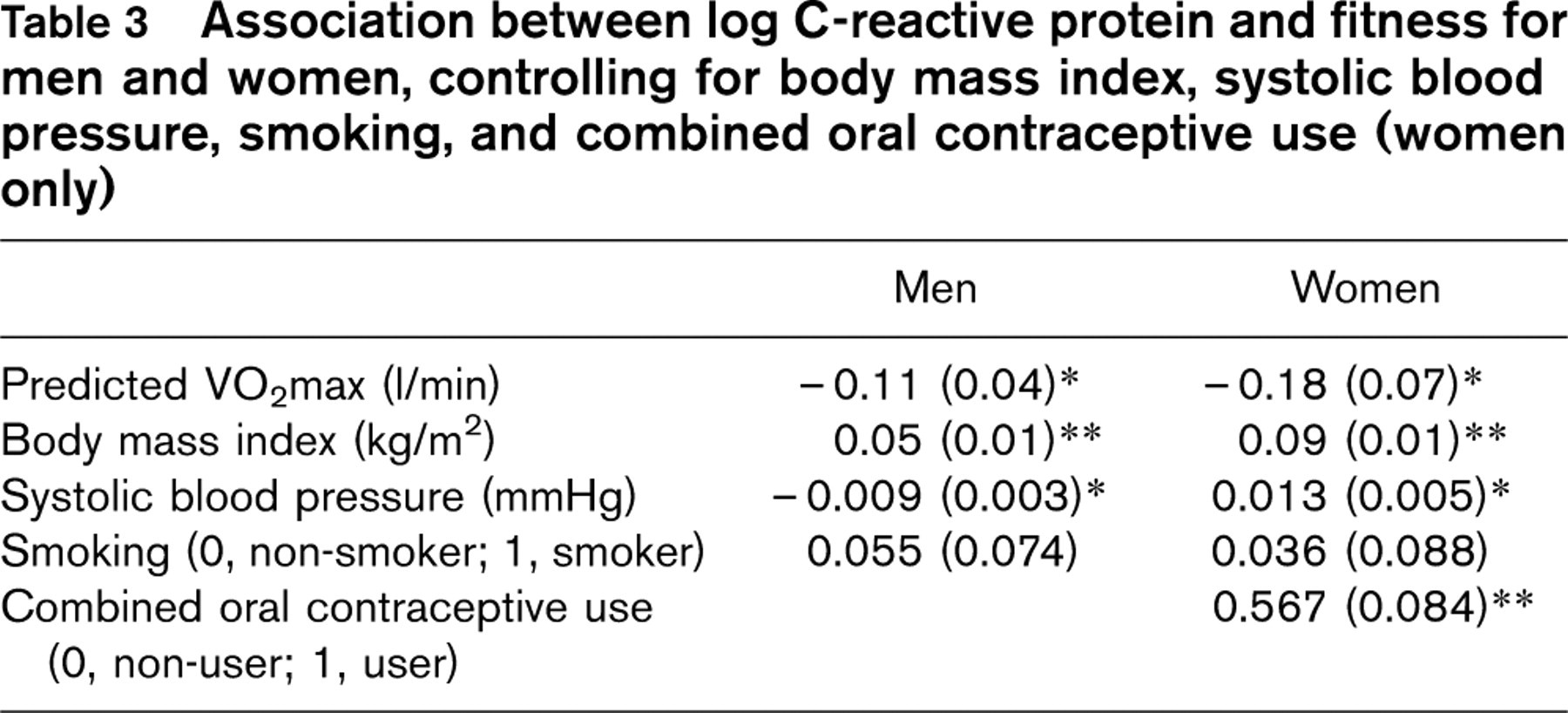
∗ P ≤ 0.01;
∗∗ P<0.001.
Regression coefficients per unit change in maximum oxygen consumption (VO2max), body mass index and systolic blood pressure. Panels show unstandardized regression coefficients (standard errors).
We also found an inverse association between physical fitness and CRP in young men after adjustment for potential confounders of BMI, systolic blood pressure and smoking. This is similar to the findings of Church et al. [17], who reported increased levels of CRP with decreasing levels of fitness in middle-aged men, which remained significant after adjustment for age, BMI, medications, the presence of inflammatory disorders, cardiovascular disease, diabetes and smoking. Isasi et al. [26] conducted a study in 205 children and young adults (mean age 10.2 years, SD 3.9) and reported an inverse association between CRP and physical fitness in men but not women. Our findings in a substantially larger group of 26 year olds showed no fitness by sex interaction, suggesting that the association of CRP with physical fitness is consistent across both sexes by early adulthood.
The present study shows that elevated inflammatory markers related to obesity and low levels of fitness are present early in adult life, and may play a role in the subsequent pathogenesis of atherosclerosis [27]. This finding is consistent with previous studies showing both fitness and fatness as independent risk factors for mortality [16].
Intervention studies in women have shown that weight loss alone [28] and weight loss with increased physical activity [29, 30] decrease CRP levels. Recommendations for lifestyle intervention have emphasized the importance of weight loss, whereas the importance of exercise has received less attention. Diet and vigorous exercise reduces blood pressure, insulin and lipid levels within 3 weeks [31], emphasizing that exercise improves cardiovascular risk independent of obesity. A recently published study has shown that cardiac rehabilitation and exercise training reduces CRP levels independently of weight loss [32]. Although it is possible that regular exercise has an anti-inflammatory action, a study in obese adolescents [33] failed to show a decrease in CRP with regular physical training, and therefore the efficacy of exercise in reducing CRP levels requires confirmation in larger intervention studies.
The limitations of this study are that we used a low sensitivity CRP assay, which may underestimate the strength of the association of CRP with fitness. Physical fitness was determined using a submaximal bicycle ergometer-based test to predict maximal oxygen uptake. The inaccuracies associated with this approach are unlikely to have biased our results, but may also have led us to underestimate the strength of the association. The study is cross-sectional and thus the risk of cardiovascular morbidity is inferred rather than measured and we were not able to evaluate mechanisms for our observations.
In conclusion, we have found that cardiorespiratory fitness levels are inversely associated with CRP levels in a community cohort of young adults independently of obesity. Physical fitness may decrease the risk of cardiovascular events by an anti-inflammatory action. These findings emphasize the importance of physical fitness as part of a comprehensive approach to reducing cardiovascular disease risk.
Footnotes
Acknowledgements
The authors would like to thank the study members, their families and friends, unit research staff, Air New Zealand, and the study founder Phil Silva.