
Abstract
Aims
Overweight, obesity and smoking are well-established risk independent factors for cardiovascular diseases. The combination of overweight or obesity with smoking may modify other cardiovascular disease risk factors. We examined the impacts of smoking, overweight and obesity on cardiovascular risk factors: total cholesterol, high-density lipoprotein (HDL)-cholesterol, non-HDL-cholesterol, C-reactive protein and fibrinogen.
Methods and results
Data from 5460 adults who participated in the cross-sectional Scottish Health Survey 1998 were analysed. In multivariable analysis body mass index and smoking were the most important risk factors for cardiovascular disease. Smoking was independently associated with higher C-reactive protein and fibrinogen concentrations in both sexes, and lower HDL cholesterol and higher non-HDL cholesterol in females (P<0.001). Overweight or obesity (body mass index 25–30 or ≥ 30 kg/m2) were independently associated with higher C-reactive protein, total cholesterol, non-HDL-cholesterol and lower HDL-cholesterol in both sexes, and higher fibrinogen in females (P<0.001). Overweight or obese current smokers had higher C-reactive protein and fibrinogen and lower HDL-cholesterol concentrations than the reference group of never-smokers with body mass index below 25 kg/m2 (P<0.001). Obese current smokers had the highest mean value and odds ratio (OR) for the risk factors across the categories, particularly for lower HDL cholesterol (OR = 11) and elevated C-reactive protein (OR = 9) (P<0.001).
Conclusion
The combination of smoking and overweight or obesity aggravates cardiovascular disease risk factors, particularly HDL-cholesterol and C-reactive protein. These results justify early intervention for overweight/obese current smokers.
Introduction
Cardiovascular disease (CVD) is a leading cause of morbidity and mortality contributing 16.6 million (29.2%) of all global deaths [1]. Multiple risk factors contribute causally to CVD, with either separate or synergistic effects. Cigarette smoking, overweight or obesity, unhealthy diet and inactivity are major lifestyle risk factors [2], associated with clinical risk factors including raised blood pressure, plasma lipids, coagulation factors and measures of inflammation. Many biochemical risk factors are attributable to overweight or obesity, especially with a central fat distribution.
Smoking promotes CVD, respiratory disease and several cancers [3] leading to premature death and ill health [4], but obesity is rapidly approaching smoking as the leading preventable cause of CVD and death [5–7]. Overweight or obese smokers thus have at least two independent risk factors for CVD and there may be synergistic effects between them [5]. Obese smokers have about twice the mortality of the obese non-smoker and four times higher than non-smokers of healthy body mass index (BMI) (22–24.9 kg/m2) [8].
Overweight/obesity and smoking both contribute to inflammation, to promote atherosclerosis and CVD [9, 10]. C-reactive protein (CRP), a non-specific marker of inflammation, and fibrinogen, an inflammatory marker and coagulation protein, both predict CVD [9, 11, 12]. It has been suggested that the inflammation markers may explain some of the link of obesity with CVD since inflammatory cytokines like tumor necrosis factor-α (TNF-α) and interleukin (IL)-6 are produced by adipose tissue [13–15]. Indeed, up to 30% of the circulating IL-6 may arise from adipose tissue [16]. Smoking generates free radicals that can activate inflammatory pathways directly, but is also associated with diets lower in fruit and vegetables as sources of antioxidants. Thus both direct and indirect mechanisms link smoking with enhanced inflammation and smoking may further interact with overweight and obesity indirectly by modulating other risk factors such as lipid profiles.
This study aimed to define the impacts of smoking status and overweight or obesity on CVD risk as determined by total cholesterol, high-density lipoprotein (HDL)-cholesterol, non-HDL-cholesterol, a secondary target of the Adult Treatment Panel III guidelines, CRP and fibrinogen in a large representative sample of adults with high prevalence of cigarette smoking, overweight and obesity.
Methods
Study subjects
The Scottish Health Survey (SHS) 1998 is a cross-sectional nationally representative survey, designed to provide a comprehensive picture of the health of the Scottish population. Full survey methods have been published elsewhere [17]. Of the total 9047 adults (3941 men and 5106 women) who participated, total numbers of valid blood measurements obtained were total cholesterol 5924, HDL-cholesterol 5891, C-reactive protein 5988 and fibrinogen 5460.
Anthropometric measures
Weight and height were measured using standard techniques by trained staff [17]. Height was measured with a portable stadiometer standing in bare feet and body weight to the nearest 0.1 kg in bare feet and light clothes with the Soehlne scales. BMI was calculated as weight divided by height squared (kg/m2). Overweight and obesity were defined as a BMI of 25–29.9 and ≥ 30 kg/m2 respectively [18].
Cigarette smoking status was classified as follows: regular cigarette smokers, those who said they smoked cigarettes at all at the time of the interview; ex-smokers, those who smoked cigarettes regularly in the past but did not currently; and non-smokers: those who had never smoked cigarettes regularly and were not current smokers. Reported physical activity was measured by a questionnaire that asked about the frequency, duration and intensity of four major types of activity: activity at home, walks of 15 min or more, sports and exercise activities, and activity at work in the 4 weeks before the interview. These activities were then compiled to calculate an estimated overall physical activity, divided into five categories based on different levels of physical activity recommendations [19, 20]. These five categories were reduced into three main levels: active, those who reached at least one of the two guideline levels (either three occasions of 20 min vigorous activity per week or five occasions of 30 min moderate activity per week or both); less active, those were not active enough to meet either guideline level but were active on at least 1 day a week; and inactive, those respondents who reported less than 1 day per week of moderate or vigorous activity of at least 20 min duration.
Habitual alcohol consumption over the previous 12 months was assessed using questions on frequency, type, average number of days per week on which alcohol was drunk, the usual quantity consumed on any one day and the finally the ‘usual’ weekly units of alcohol consumed was calculated. This was then divided into four groups of weekly alcohol intake for both men and women. For men, these quantities were under 1 unit, 1–10 units, 10–21 units and over 21 units. For women these were under 1 unit, 1–7 units, 7–14 units and over 14 units.
Information on dietary habits was obtained by a short dietary questionnaire (Dietary Target Monitor) [21]. This questionnaire included questions relating to type and frequency of major food items and recently has been validated in three key food groups [21]. In this study we used total fruit and vegetables consumption as a categorical variable divided in three groups, low consumers (<200 g per day), moderate consumers (200 to < 400 g per day) and achievers of current targets (≥ 400g per day) [22].
Social class was based on the Registrar General's Standard Occupation Classification using the current or last occupation of the chief income earner within informant's household, in one of four categories: professional and intermediate, skilled (non-manual), skilled (manual), partly skilled and unskilled [17].
Blood samples
Non-fasting venous blood samples were obtained, as described by Shaw et al. [17]. CRP was measured using the N Latex CRP mono immunoassay on the Dade Behring (Deerfield, Illinois, USA) Nephelometer II Analyzer. Total cholesterol was measured using the DAX Cholesterol Oxidase assay method calibrated to US Centers for Disease Control and Prevention (CDC) guidelines. HDL-cholesterol was measured using the DAX Cholesterol Oxidase assay method calibrated to CDC guidelines after phosphotungstic acid precipitation. Fibrinogen was measured using the Organon Teknika (Durham, North Carolina, USA) MDA 180 analyser and a modification of the clauses thrombin clotting method. Non-HDL-cholesterol, which contains cholesterol in low-density lipoprotein (LDL) and very low-density lipoprotein (VLDL) calculated by subtracting HDL-cholesterol from total cholesterol [23]. Coefficients of variation were in the range 0.9–11% for all parameters measured.
Age-adjusted geometric means of cardiovascular disease risk factors by some lifestyle factors in men
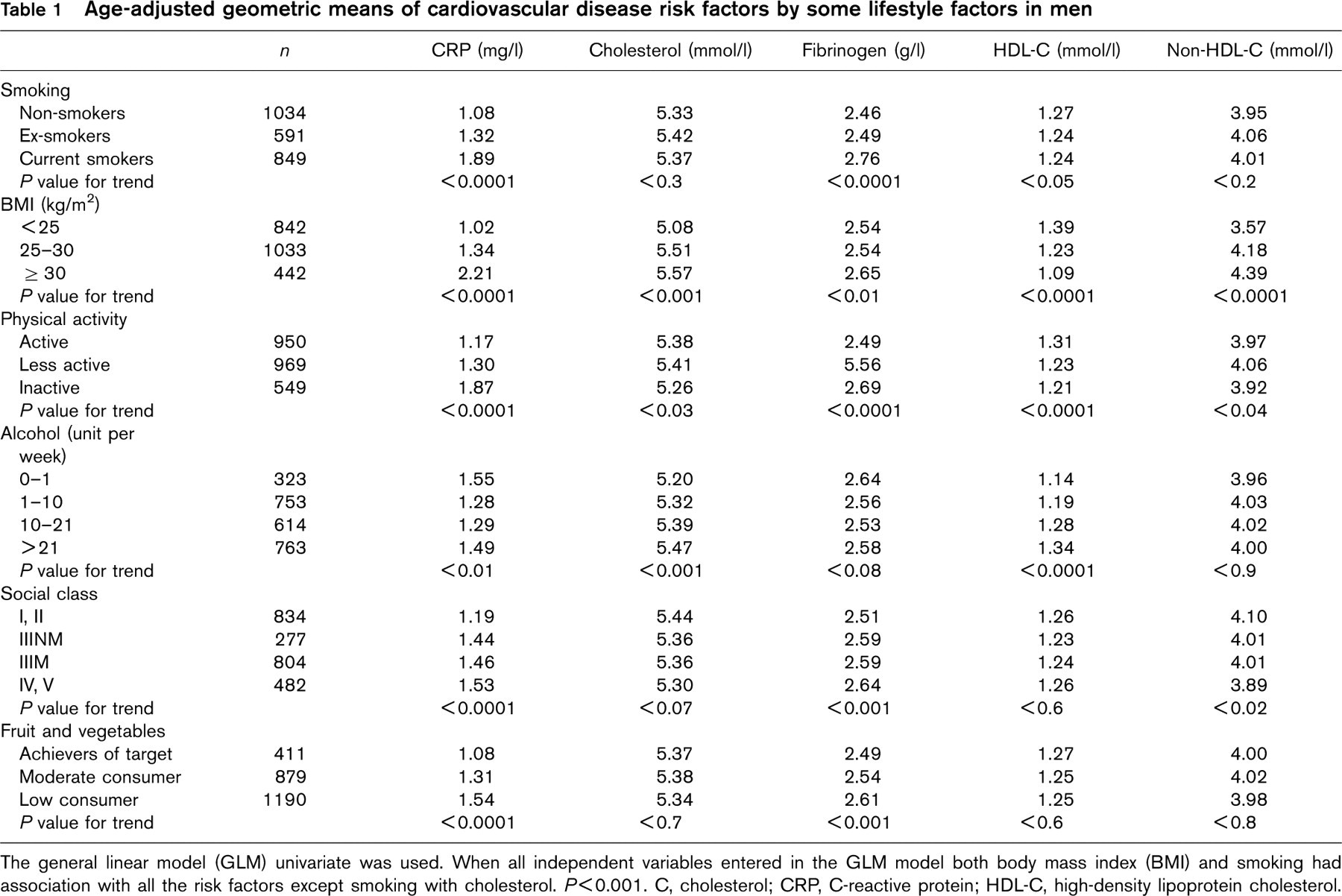
The general linear model (GLM) univariate was used. When all independent variables entered in the GLM model both body mass index (BMI) and smoking had association with all the risk factors except smoking with cholesterol. P<0.001. C, cholesterol; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol.
Data analysis
Analysis was carried out using the statistical package, SPSS 11.0 (SPSS Inc., Chicago, Illinois, USA). As data were not normally distributed, log-transformed values of dependent variables were used for improving the normality of distributions.
A general linear model (GLM) was used to compare the adjusted geometric means of the five measured risk factors among different independent lifestyle factors. This analysis was stratified by sex and controlled for age as a covariate in the univariate GLM. To evaluate the combined impacts of smoking status and BMI, cigarette smoking status and BMI were combined into nine categories and non-smokers with BMI below 25 kg/m2 were defined as the reference category. GLM incorporating the Bonferroni post-hoc test was used to compare the adjusted geometric means of the risk factors within the combined BMI and smoking variable. In this analysis age was used as a covariate and, social class, physical activity, combined smoking and BMI, alcohol consumption and fruit and vegetable consumption as fixed factors. The logistic regression model was used to compute the odds ratio (OR) and 95% confidence interval (CI) for the probability of having a high value for CRP (≥ 3 mg/l), fibrinogen (≥ 3 g/l), total cholesterol (≥ 6.2 mmol/l), non-HDL-cholesterol (> 4 mmol/l) and a low HDL-cholesterol (≤ 1 mmol/l) among the sub-groups of the combined smoking and BMI with the reference category, non-smokers with BMI below 25 kg/m2. A value of P < 0.05 was used for statistical significance.
Results
Approximately 34% of male and 33% of female subjects were current smokers, 64% of men and 54% of women were either overweight or obese and almost 18% of men and 16% of women were either overweight or obese and were current smokers.
Age-adjusted geometric means of cardiovascular risk factors by some lifestyle factors in women
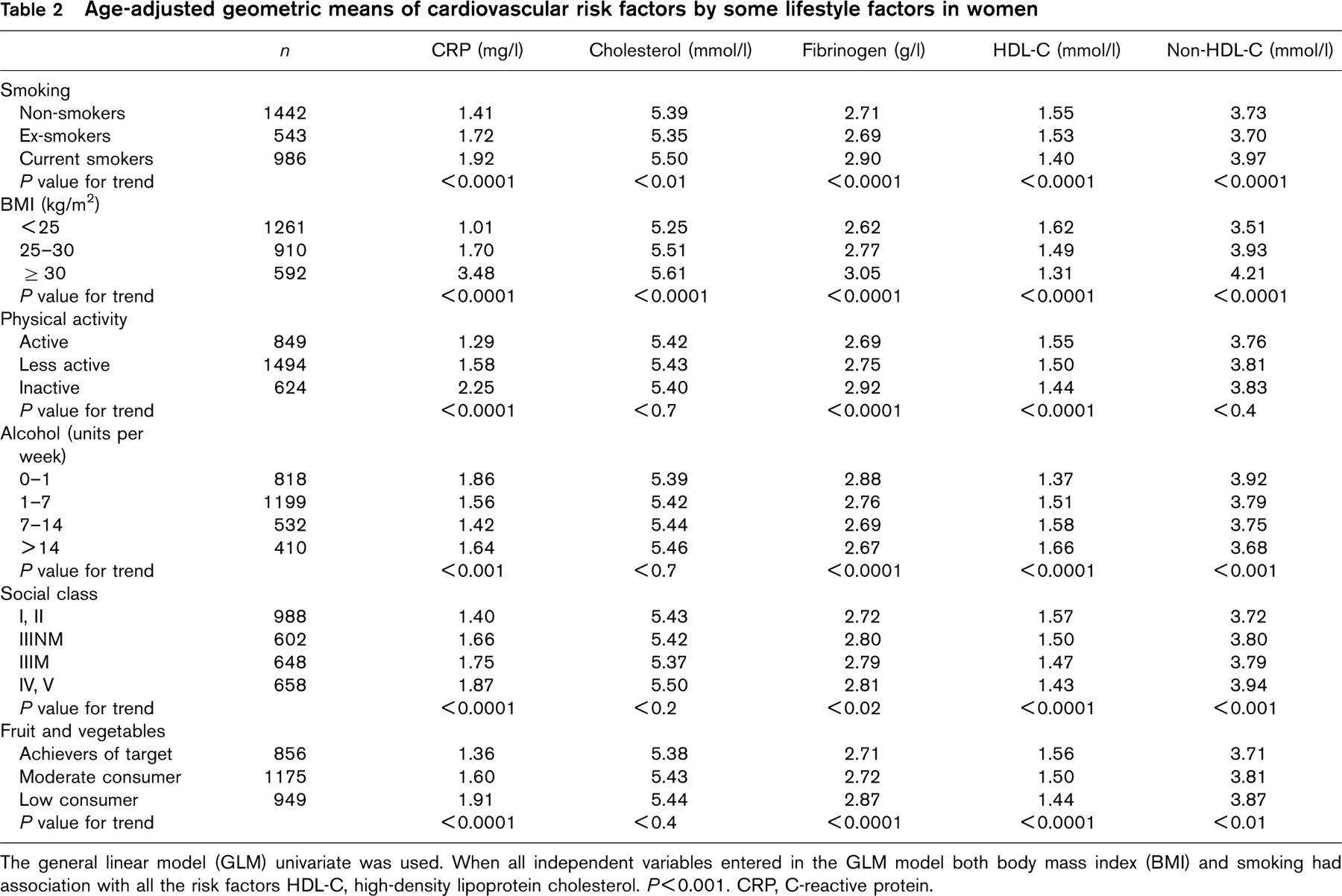
The general linear model (GLM) univariate was used. When all independent variables entered in the GLM model both body mass index (BMI) and smoking had association with all the risk factors HDL-C, high-density lipoprotein cholesterol. P<0.001. CRP, C-reactive protein.
Tables 1 and 2 show the age-adjusted means of CVD risk factors based on different lifestyle factors in men and women. Mean CRP and fibrinogen were higher among current smokers in both sexes (P < 0.0001). Women current smokers had higher total cholesterol concentrations (P < 0.01), non-HDL-cholesterol and lower HDL-cholesterol concentrations (P < 0.0001). BMI was significantly associated with all risk factors in both sexes as obese subjects had the highest CRP concentrations, total and non-HDL-cholesterol and fibrinogen and the lowest concentrations of HDL-cholesterol.
In both sexes, those who were inactive had the highest concentrations of CRP and fibrinogen and lowest concentrations of HDL-cholesterol (P < 0.0001). Total and non-HDL-cholesterol concentrations were lowest in inactive men (P < 0.05).
Men who consumed 1–21 units of alcohol per week and women who consumed 7–14 had lower CRP concentrations (P < 0.01). Total cholesterol rose with increasing alcohol consumption, but this relationship was significant only in men (P < 0.001). Alcohol consumption was inversely associated with fibrinogen in women (P < 0.0001). HDL-cholesterol increased with increasing alcohol consumption in both sexes (P < 0.0001). Alcohol consumption showed a significant inverse association with non-HDL-cholesterol in women (P < 0.001).
Those in the lowest social class had highest mean CRP in both sexes (P < 0.0001), fibrinogen in men (P < 0.001) and in women (P < 0.02), non-HDL-cholesterol in women (P < 0.001), and lowest HDL-cholesterol in women (P < 0.0001) and non-HDL-cholesterol in men (P < 0.02).
For both men and women who achieved the recommended target for fruit and vegetable consumption, CRP and fibrinogen were lowest (P < 0.001). Women who consumed larger quantities of fruit and vegetables had higher HDL-cholesterol (P < 0.001) and lower non-HDL-cholesterol concentrations (P < 0.01).
When all independent variables (Tables 1 and 2) were entered simultaneously in the GLM model, both BMI and smoking status had significant associations with all CVD risk factors except smoking with cholesterol in males (P < 0.001).
Figures 1 and 2 show adjusted geometric mean values of CRP and HDL-cholesterol among different categories of smoking and BMI. Cigarette smoking, overweight and obesity were associated with higher CRP concentration compared with non-smokers with BMI less than 25 in both sexes (P < 0.001). The obese and regular smokers had markedly higher concentrations of CRP in both sexes (Fig. 1). Smoking alone was significantly associated with lower HDL-cholesterol and higher non-HDL-cholesterol in females (P < 0.001) compared with non-smokers. Overweight and obese, smokers had significantly reduced HDL-cholesterol concentration and increased non-HDL-cholesterol in both sexes (P < 0.001) (Fig. 2) and obese current smokers had the highest levels of fibrinogen (P < 0.001).
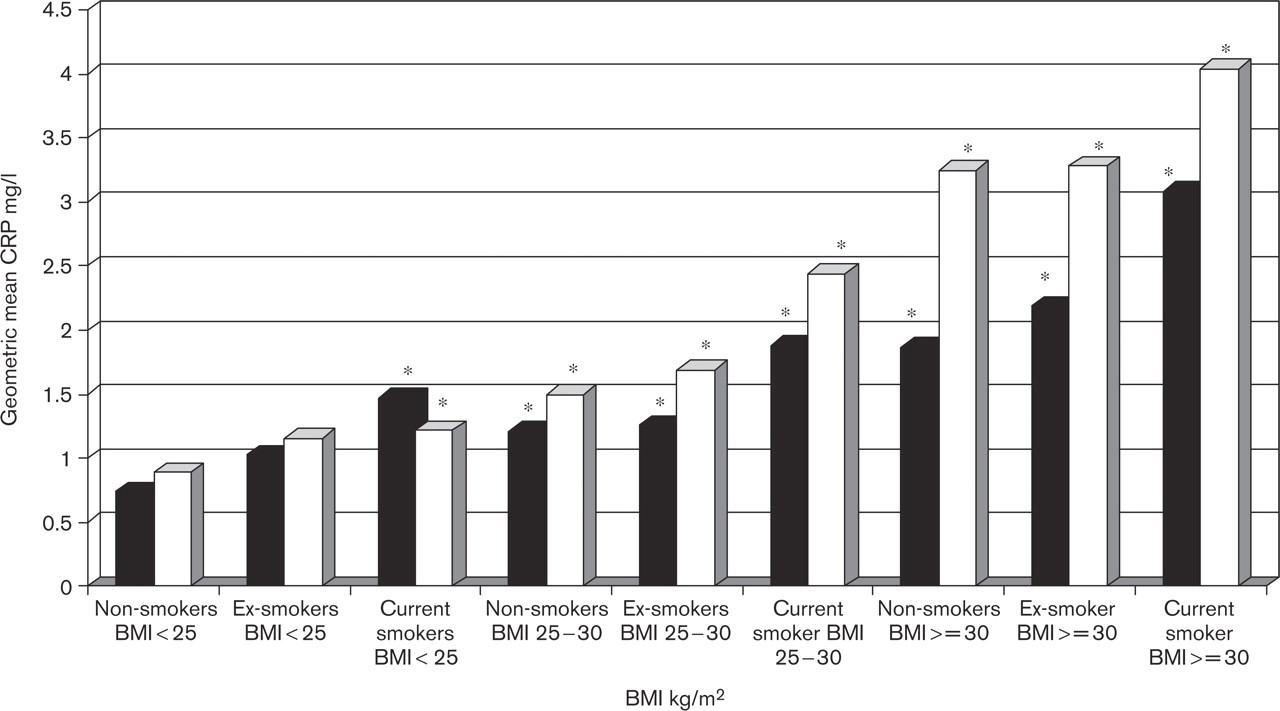
Geometric mean of C-reactive protein (CRP) by smoking and body mass index (BMI). The mean has been adjusted for age, physical activity, alcohol consumption, total fruit and vegetable consumption and social class. Black bars, men; white bars, women. ∗Compared with non-smokers BMI < 25kg/m2; P < 0.001.
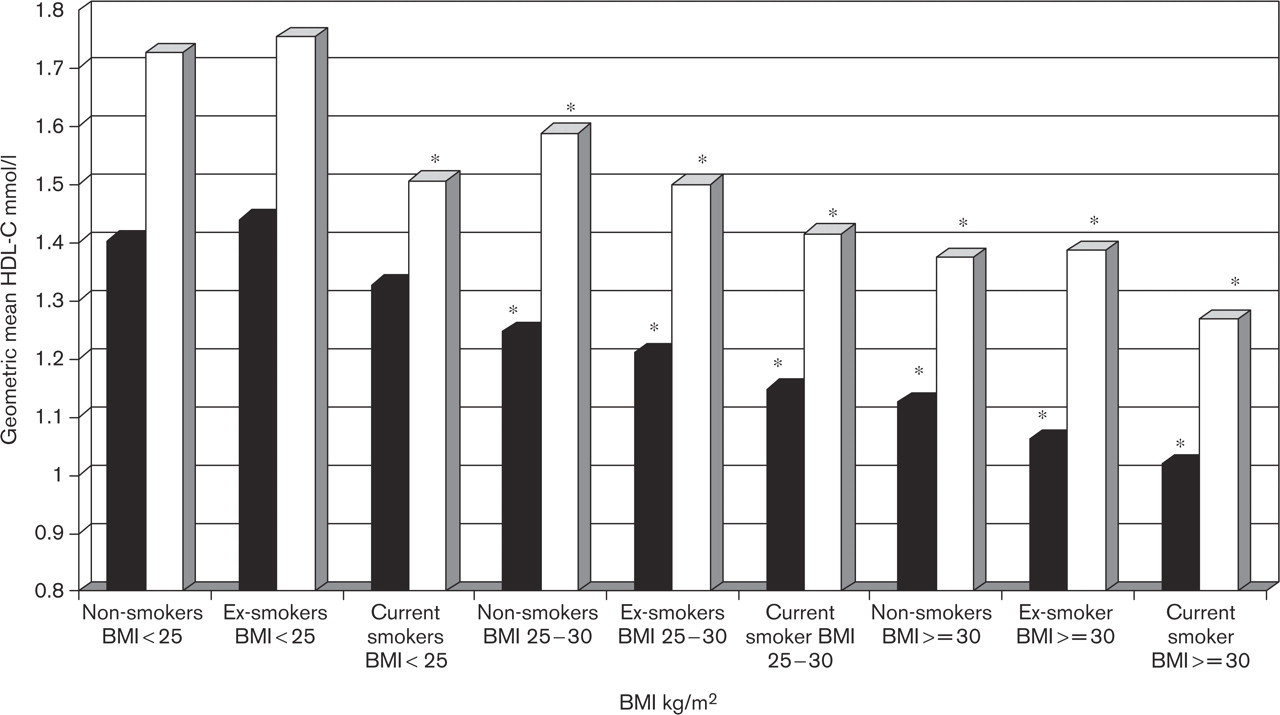
Geometric mean of HDL-cholesterol (HDL-C) by smoking and BMI. The mean has been adjusted for age, physical activity, alcohol consumption, total fruit and vegetable consumption and social class. Black bars, men; white bars, women. ∗Compared with non-smokers BMI < 25 kg/m2; P < 0.001.
Adjusted odds ratio of cardiovascular risk factors by smoking and body mass index
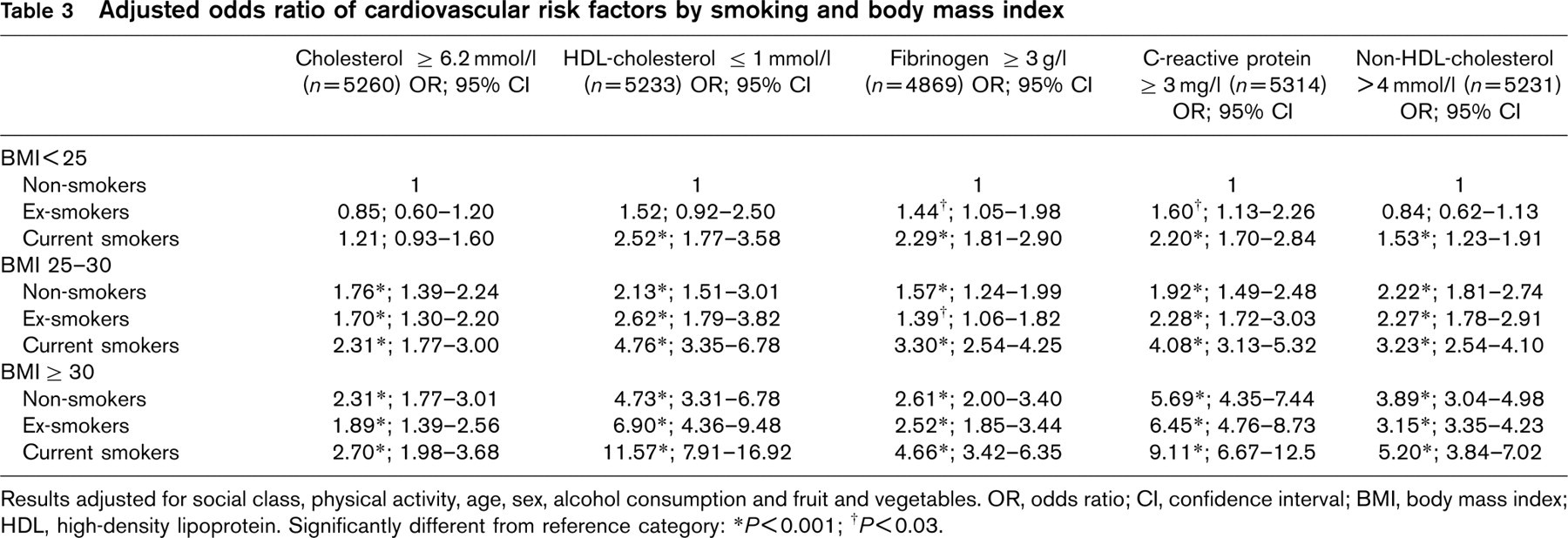
Results adjusted for social class, physical activity, age, sex, alcohol consumption and fruit and vegetables. OR, odds ratio; CI, confidence interval; BMI, body mass index; HDL, high-density lipoprotein. Significantly different from reference category:
∗P<0.001;
† P<0.03.
In total, the proportions of subjects who had CRP ≥ 3 mg/l, fibrinogen ≥ 3 g/l, total cholesterol ≥ 6.2 mmol/l, HDL-cholesterol ≤ 1 mmol/l and non-HDL-C > 4 mmol/l were 30.6, 34.6, 27.2%, 15.6 and 47.7 respectively.
Table 3 shows adjusted ORs of having the CVD risk factors above the cut-off points by smoking status and BMI. Smoking, overweight and obesity were significantly associated with a higher OR of having elevated CRP, fibrinogen, non-HDL-cholesterol and higher OR of having lower concentrations of HDL-cholesterol than non-smokers with normal BMI (P < 0.001). Obese current smokers had particularly high OR for HDL-cholesterol and CRP (P < 0.001). The ORs of having HDL-cholesterol ≤ 1 mmol/l, CRP ≥ 3 mg/l, non-HDL-cholesterol > 4 mmol/l, fibrinogen ≥ 3 g/l and total cholesterol ≥ 6.2 mmol/l in obese smokers were 11.6, 9.1, 5.2, 4.7 and 2.7 times that of the reference category respectively (P < 0.001).
In a separate analysis we excluded subjects with three major existing cardiovascular conditions that might result in secondary behavioural changes (angina, heart attack or stroke) and the results were almost the same as without exclusion of these conditions. In this analysis adjustment was not made for waist circumference because waist circumference and BMI are highly correlated and both are correlated with body fat content. A further analysis using combination of waist circumference and smoking status in nine groups (combination of waist action levels and smoking status both in three categories), however, showed that the combination of waist circumference and smoking predict the risks very similarly to the combination of BMI and smoking. The age stratified analysis in two groups (age < 45 and ≥ 45) showed that smoking had a greater effect on total cholesterol in younger age and on CRP in older age groups. Ex-smokers had lower ORs of the risk factors compared with current smokers in different BMI categories.
Discussion
This study describes links between two well-established CVD risk factors: cigarette smoking and obesity/overweight in a population with high prevalence of all these factors. Jonsson et al. [5] reported the differences in CHD among obese subjects were related to exposure to other risk factors for CVD, of which smoking was the most important. Meyer et al. [8] showed that overall risk associated with obesity increased markedly when combined with smoking. In our study we have determined the strengths of impacts of smoking, and overweight or obesity on other established CVD risk factors. The findings suggested that several other lifestyle factors - physical activity, total fruit and vegetable consumption, alcohol intake and social class - are important independent factors for CVD risk. After controlling for all these independent lifestyle factors, however, BMI and smoking remained important CVD risk factors; only these two factors related independently to all five measured risk parameters.
Association between smoking and elevated body mass index with inflammatory markers
Epidemiological and clinical studies have indicated strong associations between inflammatory markers, insulin resistance [24, 25] and the risk of CVD [9, 10]. It has been frequently shown that CRP and fibrinogen are both independent predictors of risk of myocardial infarction, stroke, peripheral arterial disease and sudden cardiac death [26–29]. Although the mechanisms responsible for elevated CRP in obese subjects are uncertain, there is a strong relationship between adipocytokines, cytokines secreted by adipose tissue, such as IL-6, TNF-α and leptin and inflammatory markers including CRP [30]. Thus the secreted cytokines from adipose tissue in obese patients may play a role in hepatic production of inflammatory proteins like CRP [30, 31].
Bazzano et al. [15] found strong positive associations between cigarette smoking, CRP and fibrinogen in a large representative sample of the US population. The third MONICA Augsburg survey 1994/95 showed strong positive associations between smoking and various markers of systemic inflammation including CRP and fibrinogen in men, but not women and smoking cessation was associated with decreased inflammation markers [32]. In a cross-sectional study in women Bermudez et al. [33] found that five markers of systemic vascular inflammation including CRP were associated with smoking. Thus the association of cigarette smoking and atherosclerosis may partly be modulated through inflammation and smoking may initiate or accelerate atherosclerosis through this process.
After adjusting for lifestyle factors, our results are in line with previous findings and demonstrate that both smoking and obesity are independently associated with inflammation markers in both sexes and smoking cessation is associated with a decreased inflammatory response. Although prior studies demonstrate that obesity influences CRP [13, 14, 30] and others that smoking also does so [15, 32, 33], ours is one of the first to document the cumulative effects of smoking together with obesity on such markers.
Association between smoking and elevated body mass index with plasma lipids
Elevated total plasma cholesterol is a vitally important risk factor for coronary heart disease [34, 35]. Both obesity and smoking are associated with various lipid abnormalities including elevated total cholesterol, triglycerides and lower HDL-cholesterol [36, 37]. After controlling for lifestyle factors, overweight and obesity were strongly and independently associated with lipid abnormalities. Although cigarette smoking had no independent association with lipid abnormalities in men and a weak association in women with BMI less than 25, combination of overweight and obesity with smoking increased the risk of lipid abnormalities.
Native American Indians participating in the Strong Heart Study showed that HDL-cholesterol was decreased in obese men and women [37]. Data from 27 populations in the WHO MONICA project also showed a statistically significant positive association between hypercholesterolaemia (defined as cholesterol ≥ 6.5 mmol/l) and BMI [38]. Norwegians surveyed over an 8-year period showed BMI was associated with elevated total cholesterol and triglycerides, and decreased HDL-cholesterol [39].
A meta-analysis defining the associations between smoking and plasma lipoproteins revealed that smokers had significantly higher plasma concentrations of cholesterol, triglyceride, VLDL-cholesterol, LDL-cholesterol and lower serum HDL-cholesterol than non-smokers [40]. Smoking acutely impairs glucose tolerance and insulin sensitivity, and enhances plasma cholesterol and triglyceride concentrations [41]. A study on British women revealed that current smokers had higher plasma concentrations of LDL-cholesterol, total/HDL-cholesterol, triglyceride and lower HDL-cholesterol than non-smokers [42]. Eliasson et al. [43] demonstrated that smokers were insulin resistant and had some disorders related with insulin resistance syndromes such as lower HDL-cholesterol, raised fasting triglyceride with lipid intolerance and impaired elimination of triglyceride from a mixed meal, potentially enhancing atherosclerosis [44].
The present results are thus in line with the literature and confirm that overweight, obesity and smoking are important and independent risk factors for atherogenic lipid profiles. The stronger relationships between obesity, lipids and smoking in women may be explained by greater central fat accumulation [45] in women smokers than in men.
How exactly smoking affects plasma lipid concentrations remains unclear. Several mechanisms have been suggested. Cigarette smoking has multiple effects including elevation of cathecholamines, growth hormone, cortisol, and insulin levels, which in turn might induce changes in lipolytic enzymes and in lipoprotein metabolism in the liver [44]. We have already reported that in spite of lower BMI in current smokers, they had higher central adiposity than non-smokers, especially in women [45] and central deposition of body fat is associated with dyslipidaemia, hypertension, type 2 diabetes and cardiovascular diseases [46].
Lifestyle behaviours including physical activity, diet, smoking, and drinking habits are major modifiable factors that affect CVD and the metabolic syndrome. Zhu et al. [47] using data from the Third National Health and Nutrition Examination Survey (NHANES III) reported that the risk of having the metabolic syndrome is substantially lower in individuals who are physically active, non-smoking, consume a relatively low carbohydrate intake, have a moderate alcohol consumption, and who maintain a BMI in the non-obese range. This study also revealed that subjects who had all of these low risk behaviours combined with BMI <30kg/m2 had a much lower risk of having metabolic syndrome. Overweight, obesity, physical inactivity and an atherogenic diet are major underlying risk factors for coronary heart disease (CHD) and metabolic syndrome [23]. Lifestyle changes have been shown to be the most cost-effective means to reduce CHD and metabolic syndrome [23]. In England and Wales between 1981 and 2000 modest reduction in major risk factors principally smoking, cholesterol, and blood pressure levels led to four times greater gains in life years than did cardiological treatments [48]. The authors concluded that effective policies to promote healthy diets and control tobacco use might yield substantial additional years of life. Almost the same result was reported in Scotland between 1975 and 1994 [49].
Longitudinal studies are ideally needed to confirm the causal relationships of the interaction between the lifestyle factors with overweight or obesity on CVD risk factors. The present results extend the rather consistent evidence base and the recognition of combined impacts of smoking and overweight/obesity on some of the components of metabolic syndrome and justifies early intervention for overweight/obese smokers. Smoking cessation might be valuably incorporated into algorithms for initiating treatment for those at high CVD risk, such as in metabolic syndrome.
In conclusion, cigarette smoking, overweight and obesity are independently associated with CVD risk factors. They increase serum concentrations of CRP, fibrinogen, and plasma total cholesterol, non-HDL-cholesterol and decrease HDL-cholesterol. In addition to these independent effects, the combination of smoking and obesity elevates CVD risk factors especially higher CRP and lower HDL-cholesterol. Early aggressive interventions to tackle weight management and smoking cessation simultaneously are justified in obese and overweight smokers given the present evidence that smoking together with overweight or obesity aggravate CVD risk factors so markedly.
Footnotes
Acknowledgements
The authors would like to thank the Scottish Health Survey Group as the original source of the data and Professor Naveed Sattar and Professor John Reilly for their advice and support.