
Abstract
Background
Cardiovascular disease is already the leading cause of death in many Asian populations. Relationships between vascular risk factors and cardiovascular disease may differ in Asian and western populations. Previously, a lack of prospective data has prevented the reliable quantification of such differences, which, if they were shown to exist, would suggest that novel cardiovascular prevention and treatment strategies are required for Asia.
Design
An individual participant data meta-analysis of 32 studies from the Asia-Pacific region involving 331 100 subjects (75% from Asia; 25% from the predominantly Caucasian populations of Australia and New Zealand).
Methods
Outcomes were death from coronary heart disease, ischaemic and haemorrhagic stroke. Hazard ratios were estimated from Cox models for systolic blood pressure (SBP), total cholesterol, triglycerides, body mass index, diabetes and current cigarette smoking, stratified by study and sex and adjusted for age, the other risk factors and regression dilution.
Results
After an average period of follow-up of 4 years there were 2082 deaths from coronary heart disease, 600 from haemorrhagic stroke and 420 from ischaemic stroke. The direction and strength of the associations between risk factors and cardiovascular outcomes were similar in the two regions, although in two cases there were significant differences. Triglycerides were more strongly associated with coronary heart disease in Australia and New Zealand (P = 0.03), whereas SBP showed a stronger relationship with haemorrhagic stroke in Asia (P = 0.04).
Conclusions
Classical vascular risk factors act similarly in Asian and Caucasian populations; prevention and treatment strategies should thus be similar. Blood pressure reduction should be particularly effective in Asia.
Introduction
Many studies have compared cardiovascular disease (CVD) or its risk factors between ethnic, or regional, groups, such as racial groups in America [1] and European populations [2]. The World Health Organization MONICA project [3] used a standardized protocol to record levels of CVD risk factors and the incidence of CVD in 21 countries. It is well recognized that differences in CVD risk factors are likely to explain differences in the incidence of CVD between regions. However, it is not well recognized that such differences in risk factors have two (summary) components: the average level, or the prevalence, may differ and the way the risk factor works (often evaluated using the relative risk) may differ. If regional differences in CVD incidence are only caused by differences in the distribution of risk factors, then treatment and preventative strategies proved in one region should be equally effective (notwithstanding cultural and cost issues) elsewhere. However, if there are additional differences in relative risks, different approaches to treatment and prevention are required.
By far the greatest amount of evidence for the treatment and prevention of CVD has come from the west, with very limited evidence from Asia. However, Asia is a huge region, where China alone accounts for approximately a fifth of the world's population. If western evidence is to be used as a basis for cardiovascular medicine in Asia, it is crucial to establish that the risk factors act at least in a qualitative sense in Asia just as they do in western populations. There are well-known differences in CVD between Asia and the west. In Asia, among all CVD events, stroke is proportionately more common; in some Asian countries (such as China) stroke is more common than coronary heart disease (CHD), the predominant form of CVD in the west. Among all stroke events, haemorrhagic stroke, which is more likely than ischaemic stroke to be fatal, is proportionately more common in Asia than in the west. There are also some differences in the distribution of major CVD risk factors. For example, people in Asia tend to have lower values of cholesterol and body mass index (BMI) than do people in Europe and north America. To be able to claim that the differences in CVD outcomes are probably caused by differences in risk factor levels, we need to ascertain that the risk factors act in the same way in Asia and the west.
Few precise data about the effect of CVD risk factors in Asia are available from prospective studies, those studies that give the most reliable estimates [4]. Precise comparisons between Asian and western populations, Australia and New Zealand, come from the Asia Pacific Cohort Studies Collaboration (APCSC), a meta-analysis of prospective studies across the region. Although APCSC has already published results for the major CVD risk factors [5–11], there has previously been no standardized approach to the comparison of Asia and Australia and New Zealand for all these risk factors. Previous papers have presented data in different ways, used different statistical adjustments, and have analysed various outcomes. Furthermore, several of these papers [5–8] used the initial APCSC database, which was later updated with five additional cohorts (172 396 subjects). This paper uses the current APCSC database to answer the question ‘Do the CVD risk factors appear to have the same effect in Asia as in Australia and New Zealand?' Using a standardized approach, the associations between each risk factor and each of CHD, ischaemic and haemorrhagic stroke are compared between the two regions.
Methods
APCSC is an individual participant data meta-analysis of cohort studies in the region, each with at least 5000 person-years of follow-up, age, sex and blood pressure recorded at baseline and cause of death recorded, when appropriate, during follow-up [12]. Studies were classified as Asian if they were based in mainland China, Hong Kong, Japan, Korea, Singapore, Taiwan or Thailand; other studies in the collaboration came from Australia and New Zealand. Details of the methods used for recording each of the risk factors are given in the earlier specialist papers [5–11]. The outcomes analysed in this paper were death from CHD (International Classification of Disease version 9 codes 410-414), ischaemic stroke (433.0434.9) and haemorrhagic stroke (431.0-432.9). Strokes of undetermined type are not considered.
Hazard ratios (approximate relative risks) for systolic blood pressure (SBP), serum total cholesterol, triglycerides, BMI, diabetes and smoking were estimated from Cox proportional hazards regression models, stratified by study and sex and adjusted for age, SBP, total cholesterol, BMI and smoking. Analyses were thus restricted to those subjects with data on all these five adjustment variables; however, age and SBP were available for all subjects in APCSC, by design [12]. All continuous risk factors were analysed as linear effects, thus assuming a log-linear relationship between the risk factor and each of the outcomes. In the case of BMI, we excluded individuals with values below 12 kg/m2, and for triglycerides we transformed to the log scale to account for outliers. Each of these decisions is justified by our earlier analyses [5,6,8–10]. The log-linear relationships were adjusted for regression dilution bias error using MacMahon-Peto attenuation coefficients [4]. These were computed from all studies with repeat measures as 1.7 for SBP, 1.7 for total cholesterol, 1.9 for log triglycerides and 1.2 for BMI. Diabetes was recorded as positive if the individual had self-reported an earlier doctor's diagnosis of diabetes or if they had indications from glucose measurement at baseline [7]. Smoking was analysed by comparing self-reported current smokers with current non-smokers. For each risk factor, the null hypothesis, that those in Asia and Australia and New Zealand have equal hazard ratios, was tested by adding an interaction term to the Cox model.
The funding sources played no role.
Results
After excluding individuals who did not have recorded values for serum total cholesterol, BMI and smoking, 331 100 subjects were available for analysis (55% of the entire APCSC), from 32 studies (Table 1). Of all subjects, three-quarters were from Asia and 41% were women. In an average of 4 years follow-up, 2082 fatal coronary attacks, 600 fatal haemorrhagic strokes and 420 fatal ischaemic strokes were observed.
There were differences (P < 0.0001) in age/sex-adjusted baseline values between the regions for all six risk factors studied (Table 2). Australia and New Zealand had higher values of blood pressure, total cholesterol, triglycerides and BMI than Asia, but smoking and diabetes were each more prevalent among Asians than those from Australia and New Zealand. In the case of smoking, this was caused by extremely high prevalences of smoking among men in China, Japan and Korea.
Study characteristics
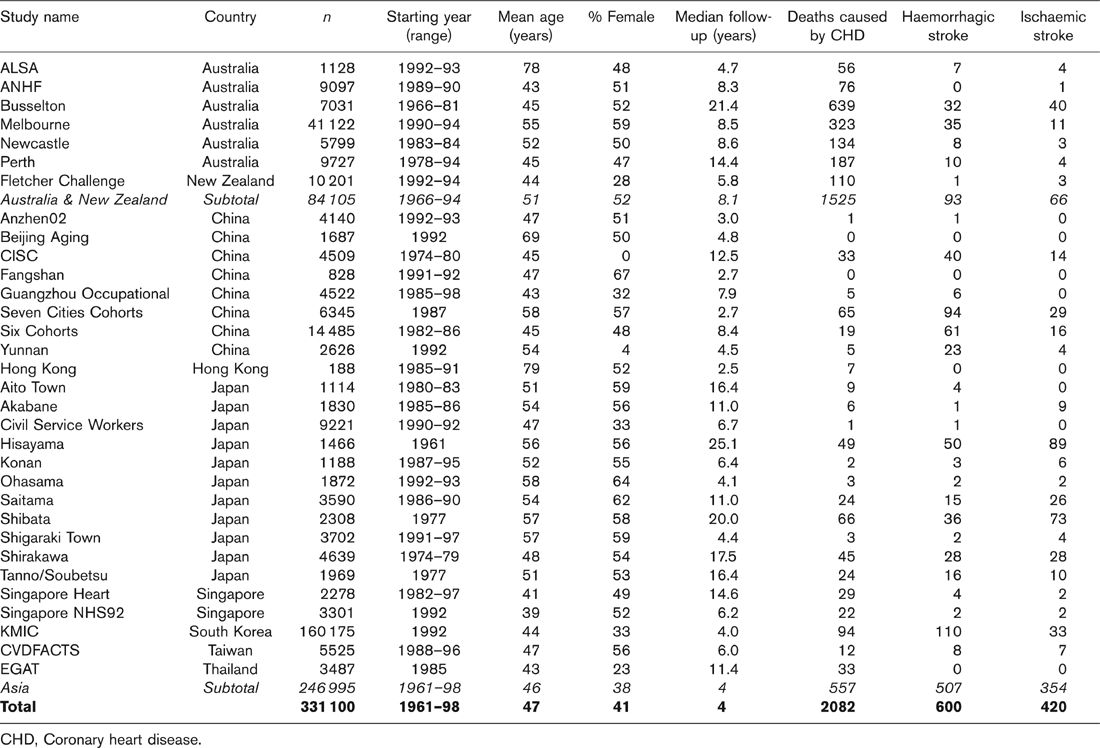
CHD, Coronary heart disease.
Age/sex-adjusted means or prevalences (with 95% confidence intervals) for cardiovascular risk factors in Australia or New Zealand and Asia

CI, Confidence interval. The P value for difference in mean (or %) value between regions was always < 0.0001. aBack-transformed after analysis on the log scale.
All six risk factors were significant (P < 0.05) independent predictors of CHD (Fig. 1) in the overall data set. There was a significant regional difference (P < 0.05) only for triglycerides (even though this had, by far, the smallest sample size; see Table 2), for which the relationship with CHD was stronger in Australia and New Zealand. SBP and BMI showed marginally nonsignificant regional differences (P = 0.06 and P =0.09), in these adjusted analyses, with Asia having higher hazard ratios than Australia and New Zealand in both cases. There was no evidence of any regional differences for total cholesterol, diabetes or smoking (P ≥ 0.43).
For haemorrhagic stroke (Fig. 2), significant adjusted relationships (P < 0.05) were found for blood pressure, smoking and total cholesterol (although the latter was negatively related). Diabetes was of borderline non-significance (P = 0.06). A regional difference was seen only for SBP (P = 0.04), in which Asia had a higher hazard ratio.
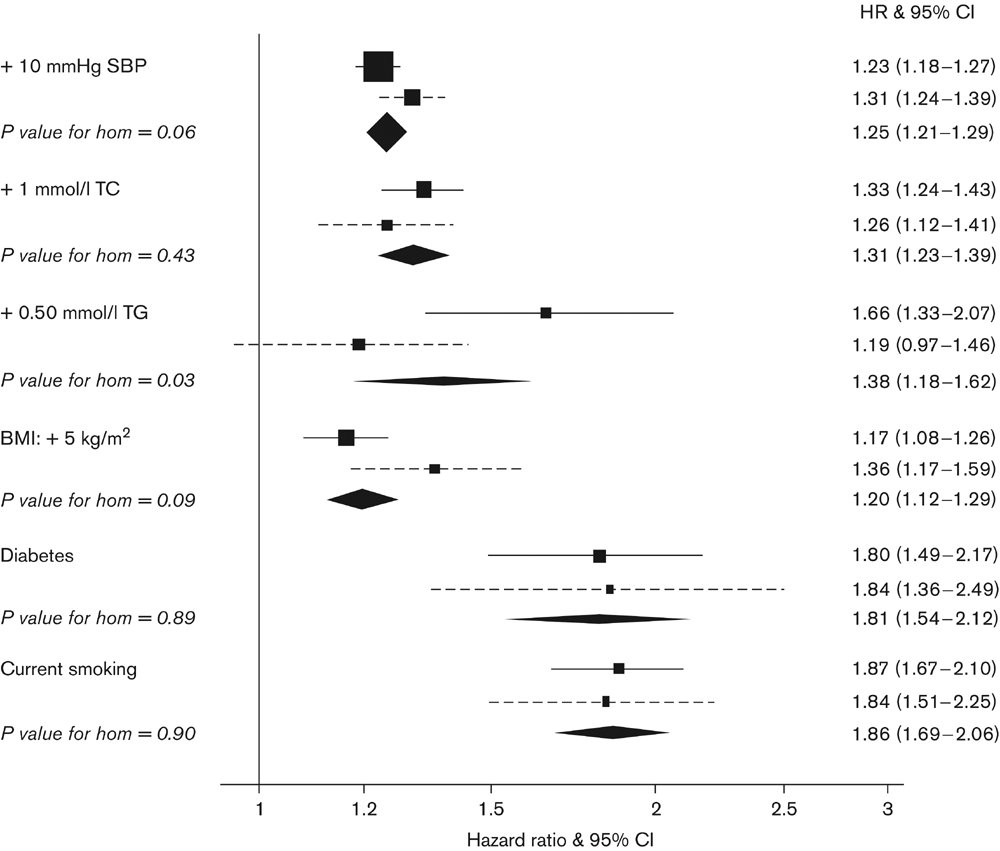
Hazard ratios with 95% confidence intervals (CI) for death from coronary heart disease in Australia or New Zealand (square and solid line), Asia (square and dotted line) and overall (diamond). P values are for tests of homogeneity between these two regions. Hazard ratios for systolic blood pressure (SBP), total cholesterol (TC), body mass index (BMI) and smoking are adjusted for each other and for age; hazard ratios for diabetes and triglycerides (TG) are adjusted for SBP, TC, BMI, smoking and age. All the Cox models are stratified by sex and study. Continuous relationships are adjusted for regression dilution error. The horizontal lines and width of diamond are 95% confidence limits.
For ischaemic stroke (Fig. 3), there were overall significant independent relationships for SBP, diabetes and smoking, and a marginally non-significant result (P = 0.06) for total cholesterol (this time in a positive direction). There were no significant regional differences (P ≥ 0.11), although the non-significant differences for blood pressure and BMI went in the same direction as for CHD and haemorrhagic stroke, in which the numbers of events were greater – see Table 1.
Discussion
This study represents one of the few opportunities to examine prospectively whether there are regional variations in the nature and size of the associations between classic risk factors and CVD. The relevance of this issue becomes apparent when considering that, by 2020, the annual mortality from CVD will reach 25 million and will have the greatest impact on populations from the lower and middle-income countries of the Asia-Pacific region [13]. Identifying regional differences in the strength and nature of the relationships between risk factors and CVD mortality may assist in the allocation of limited resources for the primary prevention of CVD in countries in which health systems are often severely under-funded and over-burdened.
Overall, the nature and strength of the associations between the majority of risk factors and CHD, ischaemic and haemorrhagic stroke were relatively consistent across populations from Asia and Australia and New Zealand. However, there were noteworthy exceptions. Increases in SBP were more strongly associated with haemorrhagic stroke and CHD in Asian populations compared with Australia and New Zealand (for ischaemic stroke, the trend was the same without approaching statistical significance). A 10 mmHg higher SBP was estimated to be associated with a 72% greater risk of having a haemorrhagic stroke in cohorts from Asia, compared with 49% in Australia and New Zealand. For CHD, the corresponding values were 31 and 23%. These findings are supported by observations from INTERHEART [14], a case-control study of over 15 000 cases of acute myocardial infarction (AMI) from 52 countries, which showed similar regional heterogeneity for the risk of AMI associated with self-reported hypertension: odds ratio (95% confidence interval) of 1.9 (1.4-2.7) in Australia and New Zealand, 2.4 (2.1-2.8) in China and 5.6 (1.3-7.2) in south-east Asia. The case-control design used by INTERHEART is, however, less reliable for examining causality than the prospective design used in APCSC [4].
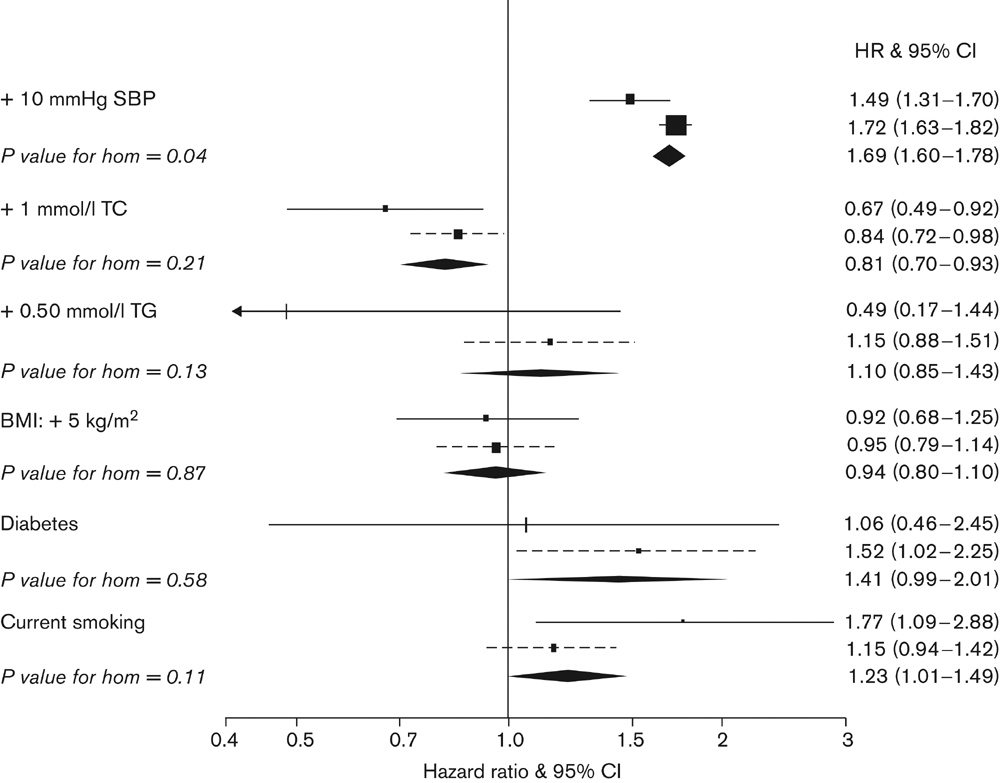
Hazard ratios with 95% confidence intervals (CI) for death from haemorrhagic stroke in Australia or New Zealand (square and solid line), Asia (square and dotted line) and overall (diamond). Hazard ratios are adjusted as in Figure 1. BMI, Body mass index; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides.
The relationship between triglyceride levels and CHD was stronger in populations from Australia and New Zealand compared with those from Asia, after adjustment for age, SBP, total cholesterol, BMI and smoking. However, this may be a chance finding; given the number of significance tests performed, we would expect some false positives [4]. In earlier analyses [9], adjustment for other lipids removed the regional heterogeneity between triglycerides and CHD. In contrast, there was no evidence that the adjusted associations between total cholesterol and cardiovascular outcomes showed any significant regional variation; findings which are, again, consistent with INTERHEART [14], which reported similar odds ratios for the association between the apolipoprotein B : apolipoprotein A1 ratio and AMI across populations from Asia and Australia and New Zealand. Similarly, there was no evidence that current cigarette smoking was less strongly associated with CVD in Asian populations, as has previously been speculated [15]. Neither was there any suggestion that diabetes was more strongly associated with CVD among Asian cohorts compared with Australia and New Zealand.
The intriguing question of whether the strength of the association between adiposity and CVD varies by region is the focus of much debate [16]. It has been proposed that, for a given BMI, Asians have a higher degree of adiposity and consequently a greater cardiovascular risk than Caucasian individuals [17]. This has led to the suggestion that the BMI cutpoints defining overweight and obesity should be lowered for Asian populations [16]. The current study suggests that a 5-unit increase in BMI, which is very substantial, will be associated with only a modest increase in the risk of CHD, after accounting for other risk factors. There was no evidence to suggest a stronger association among Asian populations compared with Australia and New Zealand. However, the possibility remains that associations between other, more sensitive, markers of obesity, such as waist circumference [18] and waist to hip ratio [19], and cardiovascular outcomes may vary across regional groups [14,20].
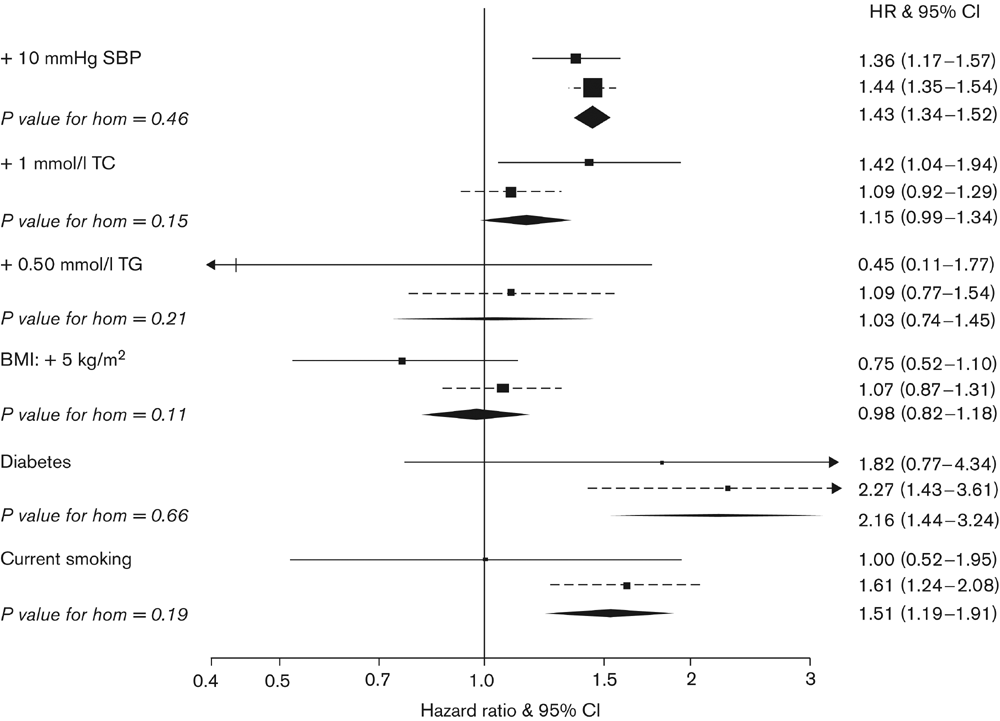
Hazard ratios with 95% confidence intervals (CI) for death from ischaemic stroke in Australia or New Zealand (square and solid line), Asia (square and dotted line) and overall (diamond). Hazard ratios are adjusted as in Figure 1. BMI, Body mass index; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides.
Our results have been derived from the largest database of its kind ever assembled in the Asia-Pacific region. Even so, results of significance tests must, as ever, be viewed with caution. In particular, we do not have sufficient events to rule out the likelihood of a regional difference when P values are greater than, but close to, the conventional 5% level. Another advantage of this study is the use of statistical correction for regression dilution error, which avoids the underestimation of effect endemic to cohort studies that only employ baseline risk factor values [4].
The current study is a comparison by regions, rather than ethnic groups. Although these categorizations are likely to overlap to a large extent, they are clearly not identical. For example, Australia and New Zealand have substantial Asian, Aboriginal, Maori and Pacific Island communities. Differences in the strength of effect by ethnic group may thus have been diluted. For those associations in which the test for regional heterogeneity was of borderline significance (e.g. blood pressure and BMI with CHD), there may still be real differences according to ethnicity. Although APCSC covers a substantial part of Asia, many countries, most notably on the Indian subcontinent, are not represented in our collaboration. Therefore our results do not necessarily have implications for all of Asia.
It is possible that random error in the measurement of the risk factors, in particular blood pressure and lipids, may have varied by country, which could have underestimated any true regional differences. Furthermore, smoking is measured in a crude, dichotomous, way here, as a result of limitations in the data available. Again, this may have led to an underestimation of any difference between Asia and Australia and New Zealand. On the other hand, as the popularity of cigarette smoking in Asia is a relatively recent phenomenon [21], there is likely to be a significant time-delay before the impact of smoking on cardiovascular mortality in Asia becomes fully apparent. This would tend to exaggerate the regional differences.
In summary, our findings serve to reinforce the importance of known risk factors for CVD across the Asia-Pacific region. Importantly, they help to dispel previous suggestions that some risk factors, such as cigarette smoking, are less relevant to CVD among Asian populations, compared with Caucasians. We find that blood pressure is more strongly related to CHD and stoke in Asia than in Australia and New Zealand, and is a key risk factor for haemorrhagic stroke, which is relatively more common in Asia than Australia and New Zealand. Therefore, population-wide measures to lower blood pressure, such as reducing the consumption of salt [22], should be of particular benefit in Asian populations.
Footnotes
Appendix
Writing committee: M. Woodward, R. Huxley, T.H. Lam, F. Barzi, C.M.M. Lawes, H. Ueshima.
Executive committee: D.F. Gu, T.H. Lam, C.M.M. Lawes, S.W. MacMahon, W.H. Pan, A. Rodgers, I. Suh, H. Ueshima, M. Woodward.
Participating studies and principal collaborators: Aito Town: A. Okayama, H. Ueshima; H. Maegawa, Akabane: N. Aoki, M. Nakamura, N. Kubo, T. Yamada; Anzhen02: Z.S. Wu; Anzhen: C.H. Yao, Z.S. Wu; Australian Longitudinal Study of Aging (ALSA): G. Andrews; Australian National Heart Foundation (ANHF): T.A. Welborn; Beijing Aging: Z. Tang; Beijing Steelworkers: L.S. Liu, J.X. Xie; Blood Donors' Health: R. Norton, S. Ameratunga, S. MacMahon, G. Whitlock; Busselton: M.W. Knuiman; Canberra-Queanbeyan: H. Christensen; Capital Iron and Steel Company (CISC): X.G. Wu; CISCH: J. Zhou, X.H. Yu; Civil Service Workers: A. Tamakoshi; CVDFACTS: W.H. Pan; East Beijing: Z.L. Wu, L.Q. Chen, G.L. Shan; EGAT: P. Sritara; Fangshan: D.F. Gu, X.F Duan; Fletcher Challenge: S. MacMahon, R. Norton, G. Whitlock, R. Jackson; Guangzhou: YH. Li; Guangzhou Occupational: T.H. Lam, C.Q. Jiang; Hisayama: M. Fujishima, Y. Kiyohara, H. Iwamoto; Hong Kong: J. Woo, S.C. Ho; Huashan: Z. Hong, M.S. Huang, B. Zhou; Kinmen: J.L. Fuh; Konan: H. Ueshima, Y. Kita, S.R. Choudhury; KMIC: I. Suh, S.H. Jee, I.S. Kim; Melbourne: G. Giles; Miyama: T. Hashimoto, K. Sakata; Newcastle: A. Dobson; Ohasama: Y. Imai, T. Ohkubo, A. Hozawa; Perth: K. Jamrozik, M. Hobbs; Saitama: K. Nakachi; Seven Cities: X.H. Fang, S.C. Li, Q.D. Yang; Shanghai Factory Workers: Z.M. Chen; Shibata: H. Tanaka; Shigaraki Town: Y. Kita, A. Nozaki, H. Ueshima; Shirakawa: H. Horibe, Y. Matsutani, M. Kagaya; Singapore Heart: K. Hughes, J. Lee; Singapore NHS92: D. Heng, S.K. Chew; Six Cohorts: B.F. Zhou, H.Y. Zhang; Tanno/Soubetsu:: K. Shimamoto, S. Saitoh; Tianjin: Z.Z. Li, H.Y. Zhang; Western Australia AAA Screenees: P. Norman, K. Jamrozik; Xi'an: Y. He, T.H. Lam; Yunnan: S.X. Yao.
The italicised studies provided data used in this paper.