
Abstract
In 927 biologically unrelated Caucasian patients with coronary artery disease it was investigated whether the NcoI restriction fragment length polymorphism of the muscle-specific creatine kinase (CKMM) gene is associated with aerobic power and with the response to physical training. Physical training significantly (P<0.001) increased peak oxygen consumption in the GG, AG and AA NcoI genotypes. Covariate-adjusted peak oxygen consumption at baseline, after training and the response to training were not different across CKMM NcoI genotypes.
Introduction
The genetic make-up of individuals strongly contributes to the individual variation in aerobic power [1] and its response to physical training [2]. In patients with coronary artery disease (CAD) this variation remains largely unexplained [3].
The muscle-specific isoform of creatine kinase (CKMM) generates high concentrations of adenosine triphosphate near the myosin heads [4]. Increased resistance to fatigue was observed in CKMM gene knockout mice in comparison with wild-type controls [5]. Sequence variation of the CKMM gene may thus influence performance and the adaptation to training. In Caucasian families of the HERITAGE Family Study an NcoI restriction fragment length polymorphism (RFLP) in the 3′ genomic region of the CKMM gene was associated with aerobic power and the response to physical training in parents [6], and was weakly (P = 0.04) linked with the response to training [7]. The presence of this NcoI restriction site generates fragments of 985 base pairs (bp) and 185 bp (A allele), whereas an A to G transition disrupts the NcoI site, resulting in a 1170 bp fragment (G allele). Whether the NcoI RFLP affects aerobic power, however, remains questionable. An association with aerobic power was not demonstrated in adult offspring [6], neither with performance level in elite endurance athletes [8].
The aim of the present study was to test whether the CKMM NcoI RFLP is associated with aerobic power or the response to physical training in patients with CAD included in the CAREGENE (CArdiac REhabilitation and GENetics of Exercise performance) Study.
Methods
Patients
Biologically unrelated Caucasian patients with CAD, who had achieved maximal exhaustion [9] during graded cycle ergometer testing before and after 3 months of exercise training from 1990 to 2001 (n = 1095), were eligible for inclusion. A total of 937 patients took part and in 927 (852 men and 75 women) the CKMM NcoI RFLP could be analysed. Patients were referred after acute myocardial infarction (68%), coronary artery bypass grafting (40%) and percutaneous transluminal coronary angioplasty (50%). The average age at testing was 56 ± 0.3 years.
Exercise testing and training
The methods for graded exercise testing and training have been described in detail previously [3]. In short, exercise tests were performed on a cycle ergometer. Respiratory data were measured through breath-by-breath analysis. Peak oxygen consumption (VO2) was defined as the highest 15-s average of VO2 obtained at the end of the test, and was expressed as millilitres per minute. Three exercise sessions per week (90 min per session) were offered.
Genotype determinations
DNA was extracted from white blood cells. Polymerase chain reaction amplification of a 1170 bp fragment was performed as described [10]. Polymerase chain reaction products were digested using NcoI (Roche Diagnostics, Mannheim, Germany) at 37°C for 2h and subjected to electrophoresis in an ethidium-bromide stained 1% agarose gel.
Statistical methods
Data are reported as means ± SE. A χ2-test with 1 degree of freedom was used to test whether the observed genotype frequencies were in Hardy–Weinberg equilibrium. Distributions were checked for normality using the Shapiro–Wilk statistic. A comparison of means at baseline versus after training was performed by paired Student's t-test; comparisons of the raw and adjusted means across the three NcoI genotypes were performed by analysis of variance and analysis of covariance, respectively. Categorical data were tested by χ2 or Fisher's exact test when appropriate. All tests were two-sided at a significance level of 5%.
Peak oxygen consumption (ml/min) at baseline and after physical training and the percentage response according to CKMM NcoI genotypes for 927 biologically unrelated Caucasian coronary artery disease patients in the CAREGENE study
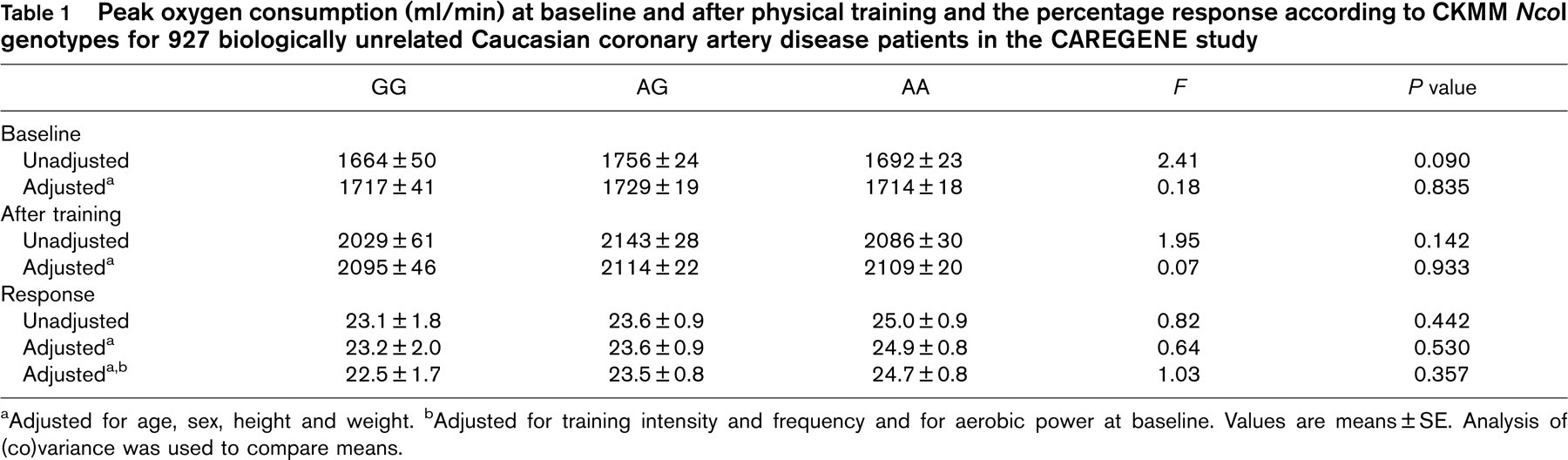
a Adjusted for age, sex, height and weight.
b Adjusted for training intensity and frequency and for aerobic power at baseline. Values are means±SE. Analysis of (co)variance was used to compare means.
Results
CKMM-NcoI genotype
Frequencies of the minor G-allele and of the common A-allele in all patients were 0.30 and 0.70, respectively. Allelic frequencies were similar between men and women, 0.31 versus 0.24 and 0.69 versus 0.76, respectively. Frequency of the GG, AG and AA NcoI genotype (f = 0.09, f = 0.42 and f = 0.49, all patients) was also comparable between both sexes, 0.09 versus 0.07, 0.43 versus 0.35 and 0.48 versus 0.59, respectively. Allelic and genotype frequencies of the NcoI RFLP are comparable to those previously observed in Caucasian individuals [6–8, 10]. Genotype distributions in all patients and within sex were in agreement with the prediction by Hardy–Weinberg equilibrium. Given the similar allelic and genotype frequency distributions in men and women, the data for both sexes were pooled for statistical analysis. Age, sex, body mass index, history of diabetes or hypertension, smoking habits, ejection fraction, cardiac pathology or intervention and drug intake were not different across the NcoI genotypes.
Aerobic power and response to training
Aerobic power at baseline averaged 1716 ± 16 ml/min and increased with physical training by 24.2 ± 0.6% (P < 0.001). Unadjusted and covariate-adjusted peak VO2 at baseline, after 3 months of training and the response to training were not different across CKMM NcoI genotypes (Table 1).
Discussion
The present study is the first to test the hypothesis of an association between the NcoI RFLP of the CKMM gene and aerobic power and the response to physical training in CAD. The results presented in this report on 927 patients with CAD who took part in the CAREGENE Study led to the rejection of the hypothesis of such an association.
Whereas previous studies [6, 7] suggested an association and linkage, the lack of association in the present report is not surprising. The NcoI polymorphism lies in the 3′ genomic region, outside the coding and 5′ regulatory sector of the CKMM gene. Therefore, this particular mutation has no consequences for CKMM protein structure, expression or functionality, and would therefore be unlikely to be the direct cause of association with any phenotype.
The different outcome in this study compared with previous reports [6, 7] may be related to methodological discrepancies, such as study design, sample size, subject selection strategies, training programme, phenotype measurement, etc.
Whereas polymorphisms of the CKMM gene other than the NcoI RFLP or the TaqI RFLP, which is in strong linkage disequilibrium with the former [8, 10], may be associated with aerobic power or endurance performance in CAD, only the functional correlate on protein level should help to decide whether genetic variation of the CKMM gene has a possible influence in future studies. A homogenous cohort consisting only of Caucasian patients with CAD was used; our findings should therefore not be generalized.
Footnotes
Acknowledgements
The authors would like to thank Professor E. Legius, Department of Human Genetics, K. U. Leuven, Belgium, for his experience and advice. J.D. is research assistant of the F.W.O. Vlaanderen. L.V. is holder of the faculty chair ‘Health and Lifestyle’ of the Faculty of Health Care, Professional University of Utrecht, Utrecht, The Netherlands.