
Abstract
Background Chronic heart failure (CHF) is associated with progressive muscle atrophy and reduced local expression of insulin-like growth factor I (IGF-I).
Design The present study was designed to test the hypothesis that the local deficiency of IGF-I in the skeletal muscle of patients with CHF would respond to a 6-months aerobic training intervention. Therefore, 18 patients [mean age 52.4 (SD 4.8) years, left ventricular ejection function (LVEF) 27 (SD 6)%] were prospectively randomized to either 6 months of training or sedentary lifestyle.
Methods Serum levels of growth hormone (GH) were measured by immunofluorometric assay, IGF-I by competitive solid phase immunoassay. IGF-I expression was assessed in vastus lateralis biopsies by real-time PCR.
Results Exercise training led to a significant increase in peak oxygen uptake by 26% [from 20.3 (SD 3.3) ml/kg per min to 25.5 (SD 5.7) ml/kg per min, P=0.003 versus control]. Local expression of IGF-I increased significantly after exercise training by 81% [from 6.3 (SE 0.8) to 11.4 (SE 1.4) relative units, P=0.007 versus control] while IGF-I receptor expression was reduced by 33% [from 20.0 (SE 2.1) to 13.8 (SE 1.7) relative units, P=0.008 versus control]. Serum growth hormone (GH) rose modestly from 0.12 (SE 0.07) to 0.65 (SE 0.37) ng/ml in the training group (P=0.043 versus baseline), however, this change was not significant compared to the control group (P=0.848). IGF-I serum levels remained virtually unchanged.
Conclusions Exercise training improves local IGF-I expression without significant changes of systemic parameters of the GH/IGF-I axis. These findings indicate that exercise training has the therapeutic potential to attenuate peripheral skeletal muscle alterations in particular with respect to local IGF-I expression in patients with moderate CHF.
Keywords
Introduction
The catabolic syndrome associated with heart failure progression has so far escaped most therapeutic strategies. Despite a growing knowledge of the factors involved in its pathogenesis – among them serum cytokines, catecholamines, cortisol/dihydroepiandrosterone imbalance – the search for an effective therapeutic intervention to halt or even reverse the process of progressive muscle wasting continues.
Recently, we described that local expression of insulinlike growth factor I (IGF-I) is reduced in skeletal muscle biopsies of patients with chronic heart failure (CHF) independent from systemic levels of growth hormone (GH)/IGF-I and is related to muscle cross-sectional area [1]. These findings indicate that the imbalance between catabolic and anabolic factors depends not only on an increase in pro-catabolic cytokines/catecholamines but might also be influenced by a deficiency in local anabolic hormones, most notably IGF-I.
In animal models exercise has been found to be the most important intrinsic stimulus for local IGF-I production and skeletal muscle hypertrophy [2]. Based on this finding and on previous studies supporting the beneficial effect of training in patients with CHF [3, 4] we assumed that exercise training may modulate systemic and/or local IGF-I levels and measured systemic and local parameters of the GH/IGF-I axis of CHF patients randomized to either 6 months of exercise training or usual sedentary lifestyle as part of the ongoing Leipzig Heart Failure Training Trial [5].
Methods
Patient selection
During the study period 18 male patients ≤ 70 years old, with stable chronic heart failure as a result of dilated cardiomyopathy (DCM) or ischemic heart disease (IHD) (New York Heart Association – NYHA – functional class II–III) were enrolled in the ongoing prospective randomized Leipzig Heart Failure Training Trial [5]. CHF patients were prospectively randomized to either 6 months of aerobic training intervention or normal lifestyle.
All CHF patients had clinical, radiological and echocardiographic signs of chronic heart failure and a severely reduced left ventricular ejection fraction (LVEF of ≤ 40%) as assessed by left ventriculography. Physical work capacity at baseline had to exceed 25 watts (W). Before entry into the study, patients had to be clinically stable for at least 3 months.
Significant valvular heart disease, uncontrolled hypertension, diabetes mellitus, hypercholesterolemia (≥ 240 mg/dl, ≥ 6 mmol/l), peripheral vascular disease, pulmonary disease or musculoskeletal abnormalities precluding exercise training were regarded as exclusion criteria.
The protocol of this study was approved by the Ethics Committee of the University of Leipzig, and written informed consent was obtained from all patients and healthy subjects prior to enrolment.
Exercise testing and respiratory variables
Exercise testing was performed on a calibrated, electronically braked bicycle in an upright position with work load increasing progressively every 3 min in steps of 25 W beginning at 25 W. Respiratory gas exchange data were determined continuously throughout the exercise test as previously described [6].
Measurement of parameters of the GH/IGF-I axis and TNF-α
Blood samples were collected from both patients and healthy subjects in the morning after a fasting period of 12h. Growth hormone was measured by immunofluorometric assay using the AutoDELFIA System (Wallac, Turku, Finland). Serum levels of IGF-I were measured after acid ethanol extraction by a competitive solid phase immunoassay according to the method of Kratzsch et al. [7]. Serum levels of IFG binding protein 3 (IGFBP-3) were determined using a commercially available ELISA (DSL, Sinsheim, Germany). All samples were run in duplicates and the average value of the two measurements is reported. The sensitivity of the assays as well as the intra-assay and inter-assay coefficients of variation have been previously published [1]. All technicians were blinded for patient status (i.e. study entry or finish) and assignment (i.e. training or control group).
Serum concentrations of tumor necrosis factor-α (TNF-α were measured by a specific high sensitive enzyme-linked immunoadsorbent assay kit (Quantakine, R&D Systems, Minneapolis, Minnesota, USA) with a sensitivity < 0.18 pg/ml. All samples were run in duplicates and the average value of the two measurements is reported.
Measurement of local skeletal muscle IGF-I expression
Skeletal muscle biopsies
Percutaneous needle biopsies were obtained from the vastus lateralis muscle at least 2 days before exercise testing as described previously [4]. Biopsies were repeated at the end of the 6-month intervention period. All biopsies were snap frozen in liquid nitrogen and stored at −80°C.
Quantification of IGF-I mRNA
To quantify IGF-I and IGF-I receptor mRNA real time PCR with the Light Cycler System (Roche Diagnostics GmbH, Mannheim, Germany) was used. Briefly, aliquots (1 μg) of isolated total RNA were reverse transcribed in a volume of 25 μl into cDNA using random hexamers. cDNA (1 μl) was added to the PCR reaction containing the following specific primers: IGF-I-U: 5′-CACCATGTCCTCCTCGCATCT-3′, IGF-I-L: 5′-ATCCACGATGCCT GTCTGAGG-3′, IGF-IR-U: 5′-GGAAGCGGAGAGATGTCATG-3′ and IGF-IR-L: 5′-ATGGATGCGGTACAATGTGA-3′.
The results for IGF-I and IGF-I receptor expression are reported as ratio over 18SrRNA, which was amplified as house keeping gene using the following primers: 18S-rRNA-U: 5′-TAGAGGGACAAGTGGCGTTC-3′ and 18S-rRNA-L: 5′-TGTACAAAGGGCAGGGACTT-3′. The variability for triplicate measurements was less than 5%.
Quantification of IGF-I protein content
The concentration of IGF-I protein was analyzed by Western-blot using a monoclonal anti-IGF-I antibody (clone Sm 1.2; Upstate Biotechnology, Lake Placid, New York, USA) followed by densitometry. Briefly, 30 μg of skeletal muscle proteins were separated on a 15% sodium dodecyl sulfate (SDS)-polyacrylamide gel electrophoresis (SDS–PAGE), followed by electrotransfer to a polyvinylidene fluoride membrane (PVDF; Roth GmbH, Karlsruhe, Germany). The transferred proteins were incubated with a 1:500 dilution of the anti-IGF-I antibody at 4°C overnight. The bound antibody was detected by a peroxidase-coupled anti-mouse antibody followed by a chemiluminescent reaction using luminol (SuperSignal West Pico, Pierce Rockford, Illinois USA). To quantify IGF-I protein the blots were analyzed by densitometry with a one-dimensional analysis software package (One-Dscan; Scanalytics, Billerica, Massachusetts, USA). To compensate for blot-to-blot variations an internal standard was loaded on each SDS–PAGE, and the densitometry results were expressed as ratio between sample and standard intensity.
Statistical analysis
Data were tested for normal distribution using the Kolmogorov–Smirnov test and for homogeneity of variances by Levene's test. Mean value ± standard deviation (SD) was calculated for all clinical variables (e.g. age, ejection fraction, peak oxygen uptake). In addition, 95% confidence intervals (CI) are given for changes in peak oxygen uptake, left ventricular end-diastolic volume, and body mass index. Biochemical measurements are presented as mean values ± standard error, indicated as SE.
Inter- and intragroup comparisons (beginning versus 6 months) were performed using the two-way repeated measures ANOVA followed by the Tukey post-hoc test. A P-value of less than 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 18 CHF patients [mean age 52.4 (SD 4.8) years, LVEF 27 (SD 6%)] were prospectively randomized to a training (n = 9) or a control group (n = 9). The majority of patients were in NYHA functional class II (16/18, 88.9%) and had a moderately reduced peak oxygen uptake [19.4 (SD 2.7) ml/kg per min]. As judged by the body mass index all patients were non-cachectic at study entry [26.9 (SD 2.1) kg/m2] (Table 1).
Seventeen patients (94.4%) received angiotensin converting enzyme inhibitors, 10 (55.6%) were on digitalis, 12 (66.7%) on diuretic medications, and six (33.3%) on beta receptor blockers.
Baseline characteristics of patients with chronic heart failure

LVEF, left ventricular ejection fraction; EDD, left ventricular end-diastolic diameter; VO2max, maximal oxygen uptake; BMI, body mass index; DCM, dilated cardiomyopathy; IHD, ischemic heart disease; NYHA, New York Heart Association functional class.
Influence of exercise training on clinical parameters
As expected, exercise training caused a 26% increase in peak oxygen uptake [from 20.3. (95% CI 17.8–22.8) ml/kg per min to 25.5 (95% CI 21.1–29.9) ml/kg per min, P = 0.003 versus control] while no change was observed in the control group [18.5 (95% CI 14.9–22.1) ml/kg per min versus 18.6 (95% CI 16.1–21.1) ml/kg per min, P = NS]. At the same time, left ventricular end diastolic volume decreased significantly by 26% in the intervention group [from 220 (95% CI 207–232) ml to 163 (95% CI 151–178) ml, P = 0.011 versus baseline]. Surprisingly, a small but significant reduction in BMI of −0.7 (SE 0.9) kg/m2 was observed in the training group [from 26.5 (95% CI 23.8–29.2) kg/m2 at study baseline to 25.8 (95% CI 23.6–28.1) kg/m2 after 6 months, P = 0.035 for change versus control].
Influence of exercise training on systemic levels of GH, GH-BP, IGF-I, IGFBP-3, and TNF-α
At baseline the serum levels of GH [0.12 (SE 0.07) in the training group versus 0.95 (SE 0.58) ng/ml in the control group, P = 0.858], IGF-I [168 (SE 19) versus 190 (SE 19) ng/ml, P = 0.370], and IGF-BP3 [3.5 (SE 0.2) versus 4.2 (SE 0.2) μg/ml, P = 0.142] were not different from healthy controls previously examined [1]. The serum levels of GH-BP, however, were significantly lower in the training group as compared to the control group [543 (SE 37) versus 1222 (SE 232) pmol/l, P = 0.019]. The reasons for this baseline difference are unclear.
As evidenced by the serum TNF-α levels, both intervention groups were in a similarly mild stage of CHF [1.9 (SE 0.2) versus 1.8 (SE 0.2) pg/ml, P = 0.818]. All the serum parameters (with the exception of serum GH in the training group) remained virtually unchanged during the training or control intervention (Table 2).
Influence of exercise training on local expression of IGF-I/IGF-I receptor
As compared with the previously published data on healthy subjects (HS) [1] local skeletal muscle IGF-I mRNA expression and protein levels were significantly reduced at baseline [IGF-I mRNA 5.9 (SE 0.5) versus 14.0 (SE 0.9), P < 0.001. IGF-I protein 0.49 (SE 0.07) relative units versus 1.29 (SE 0.15) relative units, P < 0.001].
Effects of a 6-month training program on serum and local parameters of the growth hormone/IGF-I system
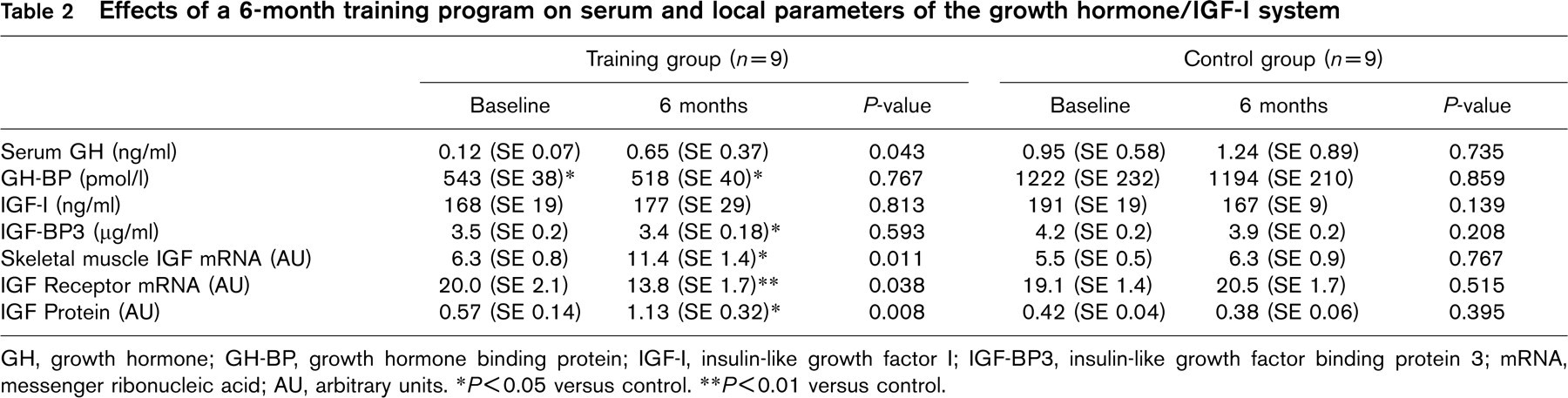
GH, growth hormone; GH-BP, growth hormone binding protein; IGF-I, insulin-like growth factor I; IGF-BP3, insulin-like growth factor binding protein 3; mRNA, messenger ribonucleic acid; AU, arbitrary units. ∗ P<0.05 versus control. ∗∗ P<0.01 versus control.
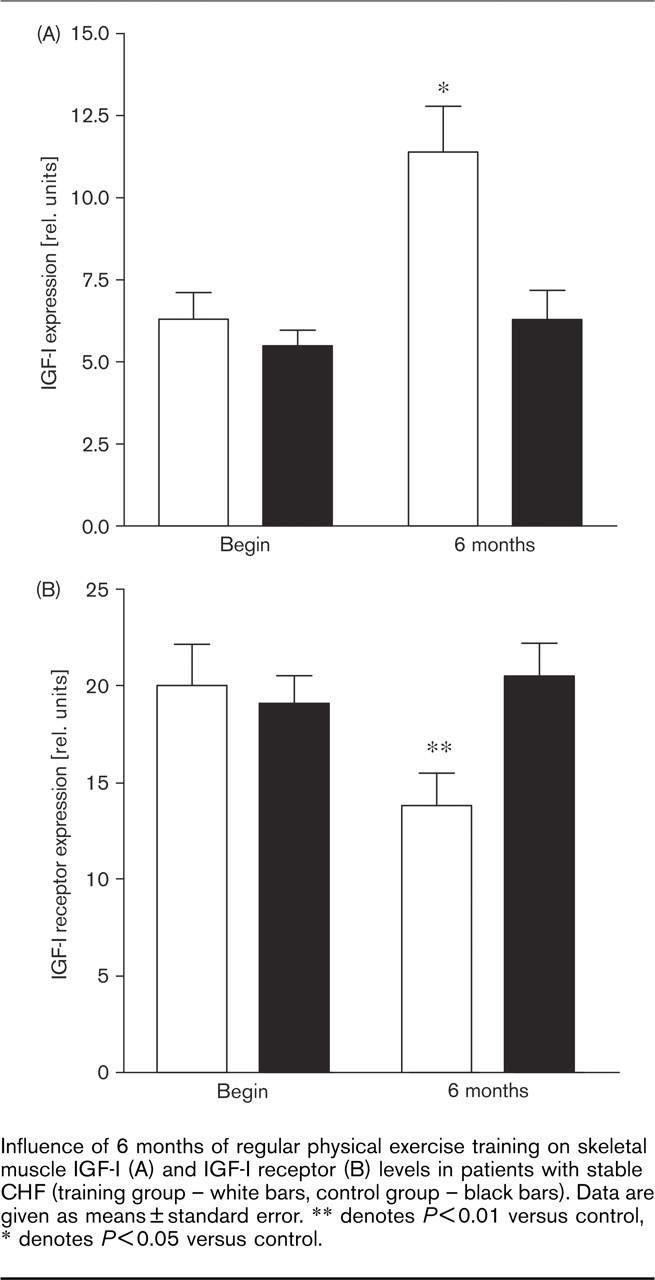
Influence of 6 months of regular physical exercise training on skeletal muscle IGF-I (A) and IGF-I receptor (B) levels in patients with stable CHF (training group – white bars, control group – black bars). Data are given as means±standard error. ∗∗ denotes P<0.01 versus control, ∗ denotes P<0.05 versus control.
Regular physical exercise training over a period of 6 months did not alter serum concentrations of either IGF-I, IGFBP3, or GH. Local skeletal muscle IGF-I expression, on the other hand, was significantly increased by 81% after training as quantified by real-time PCR [from 6.3 (SE 0.8) to 11.4 (SE 1.4) relative units, P = 0.007 versus control] – a finding corroborated by the 98% increase in IGF-I protein content [from 0.57 (SE 0.14) relative units to 1.13 (SE 0.32) relative units, P = 0.001 versus control]. IGF-I receptor mRNA was reduced by 33% [from 20.0 (SE 2.1) relative units to 13.8 (SE 1.7) relative units, P = 0.008 versus control] (Fig. 1, Table 2).
In the training group a significant correlation between change of local IGF-I protein content and change of maximal oxygen uptake (VO2max) was confirmed (r = +0.79, P = 0.011).
Discussion
IGF-I deficiency was first described as a potential catabolic factor in CHF patients with advanced heart failure and cardiac cachexia. In the meantime, however, evidence has accumulated that skeletal muscle dysfunction and loss of lean muscle bulk already starts in non-cachectic patients with CHF [8–10]. It is therefore appropriate to initiate therapeutic interventions to prevent peripheral muscle wasting in patients with stable CHF long before overt cardiac cachexia has developed. Accordingly, we enrolled non-cachectic patients with stable CHF in this first clinical trial investigating the effects of exercise training on systemic and local IGF-I levels. The current concept of the interaction between serum and local growth hormones is extended in several important ways by the current study:
Six months of aerobic exercise training were effective in nearly doubling the local IGF-I expression in skeletal muscle biopsies from patients with stable CHF – a finding which confirms the results of previous studies in healthy subjects and animal experiments in the clinical context of heart failure therapy.
The local expression of the IGF-I receptor was upregulated in stable CHF indicating a situation of ‘cellular stress’ in which the myocyte increases its sensitivity for anti-apoptotic and anabolic signals (as previously described in cardiac myocytes subjected to increased wall-stress [11]). The reduction of IGF-I receptor expression after the training intervention could be interpreted as a sign of cellular recovery and/or reduction of local catabolic/cytotoxic factors (i.e. oxidative stress, proinflammatory cytokines).
The changes in local IGF-I protein content were significantly correlated with changes in peak oxygen uptake indicating that local anabolic stimuli may contribute to the augmented exercise tolerance after exercise training.
Effects of exercise training on local skeletal muscle IGF-I levels
In a previous study we observed a significant local IGF-I decrease in patients with normal systemic GH/IGF-I levels [1]. The concept that serum and local IGF-I levels are regulated independently in CHF was corroborated in the present study by our finding that training did not alter any serum parameter of the GH/IGF-I axis while dramatic effects were seen on the local IGF-I expression. These findings suggest that local rather than systemic factors are important for the regulation of IGF-I expression in CHF.
Skeletal muscle IGF-I expression is modulated in response to either systemic growth hormone levels or alterations in muscle use. In animal experiments it has been shown that muscle unloading resulted in growth retardation and decreased skeletal muscle IGF-I expression in neonatal rats. While IGF-I overexpression alone was ineffective in preventing hindlimb suspension-induced muscle atrophy [12], a combination of GH/IGF-I supplementation and resistance exercise preserved skeletal muscle mass [13]. McKoy et al. [2] recently confirmed that 4 days of muscle stretch induced a significant upregulation of IGF-mRNA starting as early as 12h after the stimulus [14]. These findings are consistent with the hypothesis that both muscle loading/stretch and IGF-I are required to avert skeletal muscle atrophy.
In the present study we observed a more than two-fold increase in local IGF-I expression after 6 months of exercise training in patients with stable CHF. Two other studies in non-CHF populations are available on intramuscular changes of IGF-I expression in response to exercise. One in military trainees documented a higher number of IGF-I immunoreactive cells in skeletal muscle biopsies obtained after 1 week of terrain marching [15]. A second assessed the effect of a combined intervention of nutritional supplementation and resistance training in 26 elderly patients and confirmed a six-fold increase in local IGF-I expression [16]. These studies – despite being conducted in subjects without CHF and/or local inflammatory activation – provide the only available scientific basis on changes in local IGF-I expression in response to training in humans.
Our data are well in line with these previous studies. For the first time it has been confirmed that local IGF-I levels are reduced well before any systemic changes are apparent. The local IGF-I deficient state associated with CHF responds to a long-term aerobic training intervention indicating that the catabolic state in the skeletal muscle is at least partially reversible by adequate rehabilitation. It remains unclear, however, whether these beneficial effects of exercise training may also be achieved in a more advanced stage of CHF associated with a pronounced cytokine activation and local inflammatory reactions.
Exercise training had opposite effects on the expression of local IGF-I and of the local IGF-I receptor. While IGF-I increased significantly the IGF-I receptor expression was found to be reduced after training. Enhanced expression of the IGF-I receptor may be characterized as a kind of cellular survival signal which has been described, for example, in cardiomyocytes, as early as 12 h after an acute myocardial infarction [11]. The reduction of IGF-I receptor expression after the training intervention could be interpreted as a sign of cellular recovery and/or reduction of local catabolic/cytotoxic factors (i.e. oxidative stress, proinflammatory cytokines).
Role of systemic IGF-I in catabolic syndromes
The concept of a possible interaction between IGF-I levels and skeletal muscle wasting in patients with CHF was introduced by Niebauer et al. [8] who observed an association between low serum IGF-I levels and loss of lean muscle mass as well as increase in catecholamines, cortisol/dehydroepiandro-sterone ratio, and GH. This is consistent with the hypothesis that decreases in systemic levels of IGF-I occur with advanced stages of heart failure. With advanced CHF the reduced systemic IGF-I levels often fail to respond to GH application indicating a peripheral GH-resistance [17]. Therefore, the value of external GH-substitution may be doubtful in many CHF patients. Training interventions, on the other hand, potentially augment local IGF-I expression via GH-independent mechanisms and may thereby circumvent the problems of GH-resistance.
Intervention studies with IGF-I have only been conducted in animal models, yet exogenously administered growth hormone and insulin-like growth factor-I improved both cardiac [18, 19] and skeletal muscle contractility [20] by altering myofilament Ca2+ responsiveness.
In humans, however, only the short-term effects of a systemic IGF-I administration have been examined: It has been reported that acute IGF-I infusion decreases systemic vascular resistance and increases cardiac output [21]. Although some authors view supplementation of recombinant human IGF-I as a potential therapeutic strategy in patients with advanced CHF [22] possible risks need to be considered: Any systemic administration of growth factors carries a certain risk of increasing the rate of neoplasia. Long-term dose-finding studies in animal models are needed to minimize this potential adverse effect before any clinical application should be tested.
Clinical implications
This study provides first-time evidence that exercise training has the potential to attenuate peripheral skeletal muscle alterations in particular with respect to local IGF-I expression in patients with moderate CHF.