
Abstract
Background
Reduced arterial compliance is reflective of vascular dysfunction, which promotes the atherosclerotic process, and is therefore an important predictor of vascular disease. In adults, obesity, age, aerobic fitness, oestrogens and race influence arterial compliance. Although stature and blood pressure are known to influence compliance in children, other determinants are less established. This investigation sought to determine the predictors of arterial compliance in children, assess the extent to which aerobic fitness is related to compliance, and compare compliance between girls and boys.
Methods
Participants (99 children aged 9-11 years, 55 boys) were assessed for aerobic fitness, physical activity level, blood pressure, body mass, percentage fat mass, height, maturity and arterial compliance (large and small). Predictors of compliance were determined using stepwise regression. Second, children were divided into quartiles according to fitness, and arterial compliance was compared using analysis of covariance (ANCOVA). Finally, differences in compliance between girls and boys were assessed using ANCOVA.
Results
We found that fitness, blood pressure and height accounted for 37% of the variance in large artery compliance. Mass, fitness, maturity and blood pressure accounted for 44% of the variance in small artery compliance. Children in the highest fitness quartile had greater compliance than children in the two lowest quartiles, by as much as 34%. There were no differences in compliance between girls and boys after adjusting for covariates.
Discussion
These data show that aerobic fitness is associated with arterial compliance in 9-11-year-old children, supporting the concept that physical fitness may exert a protective effect on the cardiovascular system.
Introduction
Relatively new technology has allowed for the non-invasive measurement of pulse wave velocity and the arterial pulse contour to evaluate arterial compliance [1]. In the adult literature, arterial compliance is reduced in individuals with major risk factors for cardiovascular disease [2] and established cardiovascular disease [3]. Importantly, changes in arterial compliance precede, by years, clinical evidence of chronic disease [4], and as such, arterial compliance is an important early predictor of the risk of chronic vascular diseases. Arterial compliance in adults is affected by multiple variables including age [5], race [6], sex [7], arterial pressure [7] and the presence of the metabolic syndrome [8]. It is also positively related to aerobic fitness [9–11].
In children, arterial compliance is associated with blood pressure (inversely) [12], obesity [13], age [14], sex [15] and race [16]. However, little is known about the relationships between arterial compliance and physical activity and fitness in children. For example, Abbott and colleagues [17] found that habitual physical activity was positively related to the associated flow-mediated dilation in the brachial artery of 5-10-year-old children, whereas Woo and colleagues [18] found that 6 weeks of exercise, combined with diet enhanced endothelial function in obese children. The independent relationship between arterial compliance and cardiovascular fitness in healthy children has not been quantified.
Accordingly, the first objective of this investigation was to determine the relationships between arterial compliance, body fat, anthropometry, physical activity and cardiovascular fitness in elementary school children. The second objective was to explore sex differences when these factors were taken into account. We hypothesize that high levels of physical activity and fitness would be associated with improved arterial compliance. Second, as a result of the levels of sex steroids during this early pubertal period, we hypothesize that girls will have a lower arterial compliance than boys [15].
Methods
This cross-sectional investigation used radial artery applanation tonometry (HDI/Pulsewave CR2000; Eagan, Minnesota, USA), a reliable method of determining large (C1) and small (C2) artery compliance [19]. Compliance values are determined using an internal algorithm based on diastolic decay features of the radial pulse contour using a modified Windkessel model. C1 is derived from an analysis of the diastolic slope decay of the waveform, whereas C2 is derived from the oscillatory component of the diastolic decay. A detailed description of the determination of compliance from the analysis of the waveform has previously been published [3]. Validity has been found to be high compared with other measures of compliance, such as magnetic resonance imaging-based carotid artery distension (r =0.75) [20] and an invasive measurement of compliance (r = 0.82) [3]. Coefficient of variation in our laboratory was 10% for C1 and 13.7% for C2. These estimates are highly comparable with published values [21].
Subjects
We examined 99 children, aged 9-11 years from schools in the Greater Vancouver and Richmond school districts, who were part of a larger study (Action Schools! BC). All children participated in the normal school physical education class and were free of overt disease as assessed by questionnaire, completed by each child's parents. The University of British Columbia's Clinical Research Ethics Board gave ethical approval for the study. The parents of all children provided written informed consent and all children gave verbal consent.
Measurements
Cardiovascular fitness
Cardiovascular fitness was assessed using Leger's 20 m incremental shuttle run [22], designed for use with children. This measurement correlates well with direct measures of oxygen uptake in children (r = 0.72) [23].
Physical activity
The Physical Activity Questionnaire for Children (PAQ-C) was used to estimate physical activity. The questionnaire refers to the previous 7 days, and requires children to recall activities in which they participated over the previous week [24]. Total minutes of physical activity were recorded then averaged to give a daily amount.
Body composition
Total body fat was assessed using dual energy X-ray absorptiometry (Hologic QDR 4500W). The coefficient of variation for soft tissue mass in our laboratory is 0.30% (lean tissue) and 1.42% (fat tissue).
Anthropometry
Stretch stature was measured (to the nearest 1 mm) by applying gently upward traction on the base of the mastoid process. Body mass in light clothing was measured using an electronic scale (SECA, Germany) to the nearest 0.1 kg. Two measures of height and mass were taken and the mean used for analysis.
Arterial compliance
Large and small artery compliance were measured non-invasively by applanation tonometry (HDI/Pulsewave CR2000). After a 5-10 min supine rest period, the radial arterial pressure waveform of the right arm was acquired using the applanation tonometer in conjunction with an automated blood pressure on the left arm. Children were not permitted to exercise or consume a caffeinated beverage 2 h before the test. The pulse wave contour data were analysed using the HDI/Pulsewave CR2000 cardiovascular profiling system. Blood pressure was also determined from this apparatus.
Maturity
Children self-assessed their physical maturity using line drawings and descriptions of pubic hair (boys and girls) and breast stage (girls) based on Tanner staging [25]. Stage 1 represents pre-puberty, stages 2 and 3 indicate early-middle puberty, stage 4 is late puberty, and stage 5 is considered post-pubertal. The self-assessed Tanner stage agrees well with physician ratings [26].
Statistical analysis
Our two outcomes of interest were large and small arterial compliance. Predictors of compliance were determined using stepwise regression modelling. The following covariates were entered into the analysis: height (metres), mass (kilograms), percentage body fat, aerobic fitness (Leger's test), physical activity, maturity, age, and systolic blood pressure. Cumulative r2, zero-order correlations and beta coefficient are provided to show both common variance and the relative importance of each variable in the model. Analysis of covariance (ANCOVA) was used to investigate the association between sex and arterial compliance, controlling for covariates identified in the stepwise regression. ANCOVA was also used to explore the association between aerobic fitness quartiles and arterial compliance. Post-hoc (pairwise) comparisons to determine where group (quartile) differences occurred were corrected (Bonferroni). Covariates were checked for coherence to parametric assumptions. All statistical analyses were conducted using SPSS version 12.0 for Windows (SPSS Inc., Chicago, Illinois, USA) and all testing was done at the 0.05 level of significance.
Results
Participants
The physical characteristics of the 99 children measured are shown in Table 1. The children's ages ranged from 9.6 to 11.1 years. There were no significant differences in age, height, mass or percentage body fat between the boys and girls. Aerobic fitness, measured by Leger's 20 m shuttle was similar between groups. No children reported to be in Tanner stages 4 or 5.
Predictors of large and small arterial compliance
Predictors of compliance varied slightly depending on artery size (small or large). Table 2 provides a summary of the stepwise regression results. C1 was associated with (in order of appearance in stepwise regression) aerobic fitness (laps run in Leger's 20 m shuttle-run), systolic blood pressure and height; C2 was related to mass, aerobic fitness, maturity, and systolic blood pressure.
To explore further the relationship between aerobic performance and arterial compliance, children were divided into quartiles by aerobic fitness (number 20 m laps completed). Quartiles were: 1, lowest – 20 laps; 2, 21-32 laps; 3, 33-43 laps; and 4, 44 – highest laps. Large and small artery compliance was then compared between fitness quartiles, controlling for systolic blood pressure and height (to predict large artery compliance) or mass (to predict small artery compliance). C1 was significantly greater in children in the highest aerobic fitness quartile than children in the lowest two quartiles (P < 0.05) (Table 3). C2 was greater in the children in the highest aerobic fitness quartile compared with children in the second quartile (P < 0.05) (Table 3).
Descriptive characteristics of the subjects, and by sex
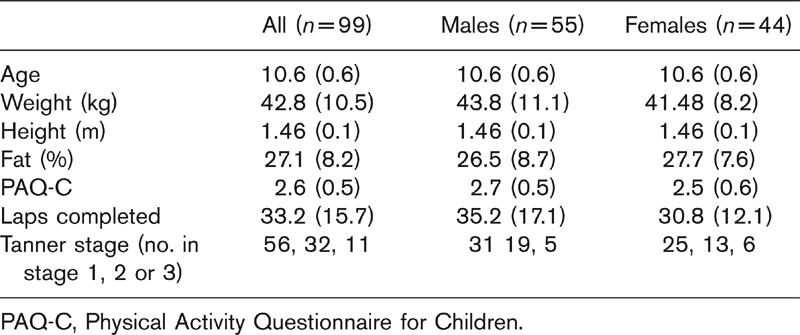
PAQ-C, Physical Activity Questionnaire for Children.
Summary of stepwise regression for large and small arterial compliance
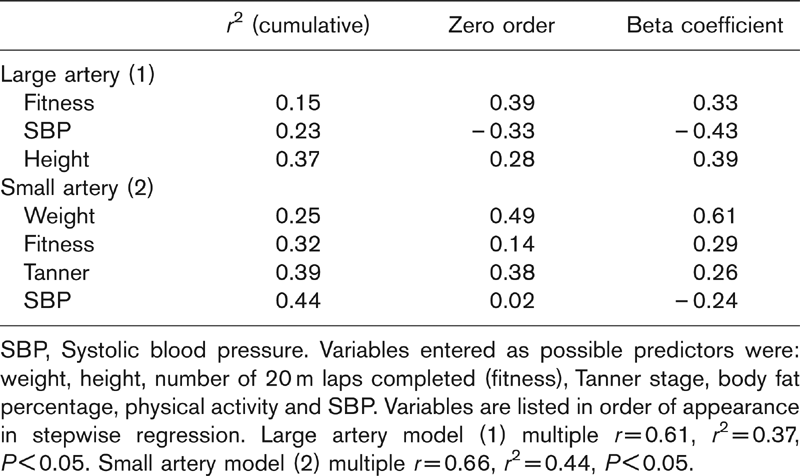
SBP, Systolic blood pressure. Variables entered as possible predictors were: weight, height, number of 20 m laps completed (fitness), Tanner stage, body fat percentage, physical activity and SBP. Variables are listed in order of appearance in stepwise regression. Large artery model (1) multiple r =0.61, r2 = 0.37, P < 0.05. Small artery model (2) multiple r =0.66, r2 = 0.44, P < 0.05.
Large arterial compliance (ml/mmHg × 10) and small arterial compliance (ml/mmHg × 100) of the participants divided into quartiles according to aerobic fitness, calculated by lap number completed on Leger's 20 m-shuttle run
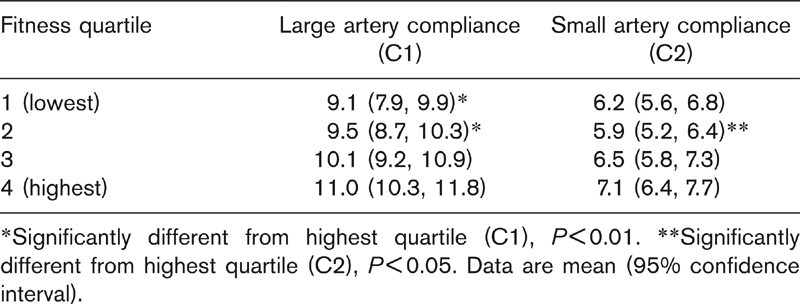
∗Significantly different from highest quartile (C1), P < 0.01. ∗∗Significantly different from highest quartile (C2), P < 0.05. Data are mean (95% confidence interval).
Effect of sex on compliance
In the unadjusted analysis, C1 did not differ between boys and girls but C2 in boys was 14.9% greater than that of girls (P < 0.05) (Table 4). However, there were no sex differences in C1 or C2 after controlling for the covariates determined from the regression model reported in Table 2 (C1, laps, blood pressure, height; and C2, mass, laps, maturity, blood pressure).
Discussion
This is the first investigation to examine the relationship between arterial compliance, measured by applanation tonometry, and aerobic fitness in children. Unique to this investigation was the finding that there is a positive relationship between aerobic fitness and large and small artery compliance in 9-11-year-old children. The predictors of compliance were different for C1 and C2.
Differences in the structure of the large conduit arteries, small arteries and microvasculature may explain many of our findings. The largest arteries are composed mainly of collagen and elastin, and stiffening is caused by changes in collagen. Compliance in these vessels is dependent solely on structure. Importantly, the non-linear pressure/volume relationship in the large arteries results in a high sensitivity of the C1 to pressure. In the present investigation, we found that systolic blood pressure was a strong predictor of C1. Aerobic fitness and height made significant, although lesser, contributions to the prediction equation. Medium-sized conduit arteries, such as the brachial and radial arteries, contain a larger amount of smooth muscle, which via the release of flow-mediated nitric oxide plays a role in their calibre and compliance. The arterioles of the microcirculation, which determine resistance, are critically dependent on smooth muscle to determine tone and stiffness. Compliance in small arteries and arterioles is therefore dependent on a varying combination of structure and function, with the C2 being largely independent of pressure [1]. This is reflected in the present study, where mass, aerobic fitness and maturity were more potent predictors of small arterial compliance than blood pressure.
Effect of aerobic fitness on arterial compliance
In this study of 99 pre-pubertal healthy children, aerobic fitness was a strong predictor of arterial compliance, especially in C1. However, in multiple regressions the influence of fitness was lessened as a result of its shared variance with height and blood pressure. Although C1 is highly influenced by pressure, our findings support theories that physical fitness may influence arterial compliance across the lifespan [5,9,27]. C2 was predicted by mass, fitness, maturity and systolic blood pressure. Here, aerobic fitness had a smaller, yet significant contribution to arterial compliance. The relevance of aerobic fitness is heightened when one considers that some predictors in the equations are not amendable, namely, maturity and height.
Uniquely, we have shown that children in the highest quartile for aerobic fitness had the highest C1, whereas children in the lowest two quartiles had the lowest C1 (Table 4). C2 showed similar patterns. These findings reflect studies in adults that associate aerobic capacity with compliance [5,10,11]. McGavock and colleagues [11] determined that 10 weeks of exercise training increased large artery compliance by 16% in 28 post-menopausal, diabetic women. Similarly, in 12 healthy post-menopausal women, a 3-month exercise programme resulted in increased aerobic capacity and a 40% increase in arterial compliance [10]. Such studies support the theory proposed by Tanaka et al. [9] that training status can attenuate the age-related decrease in compliance in older adults. However, the relationship between arterial compliance and aerobic capacity has not previously been shown in healthy children. The relationship between compliance and blood pressure [12], and compliance and anthropometry [16], determined in previous studies, were also found in the present data.
Compliance of the large and small arteries (non-adjusted) for all subjects and by sex
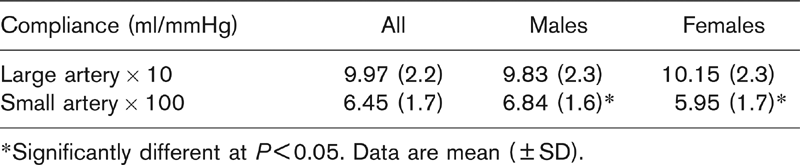
∗Significantly different at P < 0.05. Data are mean (±SD).
We did not find any relationship between physical activity and arterial compliance. Unlike Abbott and colleagues [17], who correlated habitual physical activity (using radio-labelled isotopes) with endothelial function in children, we assessed only deliberate activity, such as sports participation and play, using a self-report questionnaire. This discrepancy in findings could be because questionnaires, especially in children, may provide a less accurate assessment of actual habitual physical activity, compared with direct methods, such as observation or radio labelling. However, a retrospective investigation by the Northern Ireland Young Hearts Study found that the relationship between aerobic fitness and arterial stiffness in young adults was not mediated by physical activity [27]. The relative importance of both physical activity and fitness to health outcomes has been explored [28]. Interestingly, the analysis of data from the Aerobics Centre Longitudinal Study by Blair et al. [28] determined that when activity, fitness and various other factors were included in a multivariate model, only fitness remained strongly associated with mortality. Although Blair et al. [28] provide a rationale for this result, and state that it is not possible to determine which has a greater impact on health, their meta-analysis showed fitness to have a stronger and more consistent dose-response relationship with morbidity and mortality than physical activity. However, the extent to which assessment methods of fitness and physical activity influence this relationship should be considered.
Greater aerobic fitness had been associated with low arterial stiffness (high compliance) in adults using a number of measurement modalities including pulse wave velocity, magnetic resonance imaging and pulse contour analysis [29], but the underlying cause for this relationship has not been established. Several hypotheses exist concerning the relationship between exercise and arterial compliance. The sheer stress on the vessel lining created by exercise may increase the bioavailability of nitric oxide in the endothelium resulting in vasodilation [30]. This increase in nitric oxide may also counterbalance the activity of nitric oxide-inhibiting oxidants, such as super-oxide [31]. Alternatively, habitual physical activity may cause chronically lowered sympathetic activity, resulting in decreased vascular tone [32]. These factors would have a large influence on C2 in particular. Kingwell [29] devised a cyclical model, linking increased arterial stiffness, increased pulse pressure, reduced coronary perfusion and myocardial performance with decreased exercise capacity and fitness. The question of whether a predisposition to stiff arteries or a low physical fitness instigated the cycle was posed. Although evidence from several intervention studies in adults would suggest that the increase in fitness may initiate the cycle, the present study does not allow us to infer causality as to whether the high aerobic capacity results in physiological changes causing a higher compliance, or vice versa. However, we have shown that the positive association between arterial compliance and aerobic fitness, which is now fairly established in adults, is present in children as young as 9 years of age. Furthermore, the inclusion of children in such studies is of great importance as they are relatively unaffected by many of the variables that influence adult cardiovascular systems, for example, smoking, illness or prolonged exposure to poor diet and inactivity.
Effect of sex
In this study, after adjusting for the important covariates, compliance values were similar for boys and girls. The influence of sex is likely to be dependent on the levels of sex steroids and these were not assessed in the current study. The difference between boys and girls would occur or diminish during times when these steroid peak or fall, namely, puberty and menopause [15]. As similar numbers of girls and boys reported being in each Tanner stage, but as most children were pre-pubertal, any sex differences may not yet have become evident. In the current study, maturity was a weak but significant predictor of C2.
Conclusions
We acknowledge some limitations of the study. Aerobic fitness was ascertained from a field-based test as opposed to a direct measurement; however, a reliable and valid shuttle-based test was used [23]. Second, the maturational stage was established by self-report and not direct measures of steroid level, meaning that the influence of pubertal stage cannot be determined conclusively. Tracking these children as they advanced through puberty would provide us with a clearer picture of the influence of hormones on arterial compliance. Finally, an assessment of the effect of an exercise intervention on arterial compliance in normal mass, healthy children is warranted.