
Abstract
Atherothrombotic disease is now the leading cause of mortality in the world and there are only a few methods available to estimate risk of vascular disease. Vascular disease risk assessment methods have been developed from a variety of population based studies and the most frequently used approaches include algorithms developed by Framingham (USA), Munster (Germany), and SCORE (Europe). The field of risk estimation is dynamic and inclusion of newer factors and populations is under active consideration and methods such as discrimination and calibration are now available to evaluate the use of risk assessment tools across different world regions.
Introduction
Atherothrombosis, which may be defined as atherosclerotic plaque disruption with superimposed thrombosis, is the underlying condition that results in events leading to myocardial infarction, ischaemic stroke and vascular death [1]. It is now the leading cause of mortality worldwide [2]. Of the estimated 55 694000 people who died in 2000, 28.7% of fatalities were due to atherothrombosis, manifested mainly as cardiovascular/cerebrovascular death. This disease considerably outranks all other major causes of death, including AIDS (5.1%), pulmonary disease (6%), injuries (9.1%), cancer (12.6%), and infectious and parasitic diseases (17.8%) [2].
The manifestations of the disease are varied and manifold: stenosis in an atherosclerotic artery may give rise to angina, a transient ischaemic attack (TIA) or intermittent claudication, while atherothrombosis in the coronary arteries is the major cause of acute coronary syndrome (ACS), defined as unstable angina (UA) and non-ST segment elevation myocardial infarction (MI). Atherothrombosis of the cerebral arteries can result in TIA or ischaemic stroke, or it can contribute to the progression of peripheral arterial disease (PAD), producing intermittent claudication, ischaemic necrosis and, potentially, loss of the limb. Importantly, a person suffering from any one manifestation of atherothrombosis is at risk of future disabling or life-threatening events caused by the same underlying disease process, as evidenced by the substantially higher risk for stroke following MI [3].
Restrictions in surveys of cardiovascular disease
Reviewing surveys of cardiovascular disease (CVD) performed during the past two decades, it can be seen that these have been restricted in one or more ways. Although many have investigated the incidence of CVD in large populations, they have not specifically evaluated the broad population at risk of atherothrombotic events. Studies such as The Framingham Heart Study [4], The World Health Organization's Multinational Monitoring of trends and determinants in Cardiovascular disease (MONICA) [5], The United States' National Health and Examination Survey (NHANES) III [6], and large European surveys such as those carried out in Scandinavia [7,8], have generally had only a regional or national focus [9]. Although the Framingham population represents that most intensively studied for cardiovascular risk factors and outcomes, it is composed primarily of Caucasians. It is not certain that absolute risk for this group is similar to that for other populations [4]. Other study subject groups have suffered from similar geographical or ethnic restrictions, such as the Malmo Preventive Project (MPP), which was conducted in a single Swedish city [7], the Finnish Kuopio Ischaemic Heart Disease Risk Factor Study, based on a single region [8], (both these studies were also restricted to males). In addition, even though black, white, and Hispanic Americans participated in the NHANES III survey, this study has limited outcome information [6].
Large-scale studies have often examined only one manifestation of atherothrombosis. The Global Registry of Coronary Events (GRACE) focused on the management of acute coronary syndromes (ACS) on a transcontinental level [10–13] as did its European counterpart, the European Network for Acute Coronary Treatment (ENACT) study [14]. The CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines) registry is following up on these efforts, enrolling ACS patients in the USA only [15]. In addition, ACS was the primary interest for the Organization to Assess Strategies for Ischaemic Syndromes (OASIS) investigators when comparing invasive cardiac procedures and outcomes [16], as were the studies on the use of tissue plasminogen activator and reperfusion therapy, which were recorded by the National Registry of Myocardial Infarction (NRMI) [17,18]. Although some studies have investigated the influence of diabetes mellitus on clinical and sub-clinical cardiovascular disease [19], surveys have generally been restricted either to a pre-defined patient group or hospital setting [10,13,16,17]. Since most studies have concentrated on selective subject classes (mainly from the USA and Europe), the ability to generalize from the experience in these locales is moot.
Use of Framingham risk factor algorithms in USA populations
In 1998, the Framingham coronary heart disease (CHD) risk approach was simplified, to include categories of blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, and simple groupings for smokers and diabetes mellitus. The recommendations followed the blood pressure levels set forward (and still followed) by the Joint National Committee on High Blood Pressure, and the cholesterol and HDL cholesterol levels used lipoprotein levels set by the National Cholesterol Education Program [20,21]. In 1999, acknowledging concern as to whether the predictions derived from the white Framingham population could be generalized, a National Heart, Lung, and Blood Institute (NHLBI) workshop was organized to address the validity of Framingham CHD risk functions to other groups. The Framingham CHD prediction scores were subsequently validated using a large number of observational data sources, representing multiple ethnic groups [22]. This scientific effort was restricted to American studies and most of the data came from observational studies of whites, including the Atherosclerosis Risk in Communities ([ARIC] three white cohorts, one black cohort), the Physicians Health Study, the Honolulu Heart Program (Japanese-American men), the Puerto Rican Heart Study (Puerto Rican residents), the Strong Heart Study (Native Americans), and the Cardiovascular Health Study [22]. External calibration of CHD risk estimation was undertaken to test whether equations developed from an individual site could reliably predict CHD outcomes in other locales. The Framingham equations were evaluated in each site and showed good predictive capabilities in outcomes for the various ethnic groups and ages represented.
However, there were some exceptions, and the Framingham CHD risk equations systematically overestimated CHD risk in the Hawaiian men. Marked improvement was achieved when the risk equations were adjusted for the overall CHD rates in Hawaii using the means of the risk factor levels from the Hawaiian participants [22]. Similar effects were observed in a recent collaboration between Framingham investigators and Chinese scientists, in the estimation of absolute risk for initial CHD events in Chinese volunteers [23]. In this study, the Framingham CHD risk functions were compared with the performance of functions derived from the Chinese Multi-provincial Cohort Study (CMCS), involving 30 121 adults, aged 35-64 years at baseline, followed for a 10-year period. The original Framingham functions were found to overestimate systematically the absolute CHD risk in the CMCS, predicting a rate of CHD death of 20% in the top decile of risk for men, when the measured rate was 3%. Once more, the performance of the Framingham functions in the Chinese cohort was substantially improved when recalibrated with the mean values of risk factors and mean CHD incidence rates of the Chinese cohort [23].
On the other hand, the Framingham equations have been shown to be able to reliably predict CHD risk in black men and white men who participated in the ARIC study, and good predictive capability was also shown for the ARIC white women and black women, without any need for adjustments, suggesting these equations provided reasonable estimates for CHD risk in black American population groups [22]. Although these data for black American population groups suggest that Framingham risk estimations are reasonably predictive of cardiovascular outcomes, it has been suggested that a variety of factors may lead to a greater degree of risk misclassification in this ethnic group [24]. These include differences in blood pressure treatment and predisposition towards left ventricular hypertrophy and greater left ventricular mass, in addition to different distributions of HDL cholesterol and lipoprotein (a), a greater tendency toward end-organ kidney damage, and less arterial calcification among black Americans [24].
Application of Framingham algorithms in Europe
Concerns in Europe about the prediction of CHD risk using Framingham prediction equation led to the Systematic Coronary Risk Evaluation (SCORE) project, which was initiated in 1994 as a joint effort originally between the European Societies of Cardiology and Hypertension and the European Atherosclerosis Society. (Later the International and European Societies of Behavioural Medicine, the European Society of General Practice, the European Heart Network, and the International Diabetes Foundation also became contributing participants.) It has been reported that the Framingham risk score overestimated risk of cardiovascular events in the lower-risk populations of Southern Europe. The SCORE project assembled datasets from 12 European cohort studies, mainly carried out in general population settings, involving more than 200 000 individuals, and representing 2.7 million person-years of follow-up [25]. Fatal cardiovascular disease was estimated as the vascular disease outcome, because there was insufficient data to assess CHD morbidity.
Estimation of total cardiovascular risk, rather than risk of coronary heart disease, was the aim of this study. The SCORE Project reported that risk of CVD death could be estimated with good discrimination, although risk of death from heart attack or stroke varies widely across Europe. It was found that CHD mortality risk in Europe was related to latitude; greater risk was seen in the North and lower risk was found in the South of Europe. Consequently, two CVD death risk estimating algorithms were developed – a high-risk algorithm for persons from the high CVD risk countries of Russia, Sweden and the UK; and a different CVD risk algorithm for regions where CVD risk was lower, such as France and Southern Germany. Unexpectedly, SCORE scientists also reported that HDL cholesterol information did not markedly improve the capability of CHD risk estimation in their data, a result that differed from the North American experience. After extensive evaluation, using two parallel systems comparing the effect of cholesterol alone with that of cholesterol/HDL ratio, it was concluded that both systems had a remarkably similar ability to estimate risk of CHD death [25].
The large number of countries, the different collection methods, and difficulty in assuring accuracy in CHD events across the different regions led to limitations within the SCORE Project. The charts produced are limited in vascular disease risk estimation by use of measurements from a single clinic visit and the potential effects of regression-dilution bias, as statisticians have noted that prognostication is improved when more than one measurement is used to characterize an individual's risk of later vascular events. In addition, the charts consider principal risk factors only, and other factors that modulate risk, such as family history of premature CVD, milder degrees of impaired glucose regulation, triglycerides, and fibrinogen were not included. Arguably, the use of CVD mortality experience only and the restricted representation of minority groups in SCORE may limit its utility outside of Europe.
A suggestion that the Framingham risk estimation is not universally applicable comes from an analysis of a large cohort of middle-aged European patients with hypertension [26]. This prospective cohort survey compared the actual risk with that predicted by either the Framingham equations or models derived from the International Nifedipine GITS Study: Intervention as a Goal in Hypertension Treatment (INSIGHT study) [27]. This study found large between-country differences in the actual incidence of CVD events, which ranged from 3% in France to 7% in the UK, whereas the Framingham model showed small between-country differences and overestimated CVD risk in all countries (two-fold higher for the UK to four-fold higher for France), but did not overestimate the risk for stroke compared with the actual risk [26]. The decline in CHD mortality over the past few decades and improvements in control of hypertension and other risk factors are likely explanations for these systematic overestimations. The report does point up the need for contemporary regional data to help make accurate estimations of CHD risk.
Bastuji and colleagues concluded that Framingham models should not be used to predict absolute CHD risk in the European population as a whole. Such prediction models might be used within each country, provided that cut-off points defining high-risk patients have been determined within each country. However, the authors of this analysis acknowledged a number of shortcomings of its own, including study of a selection population and that follow-up that was limited to 4 years may be too short for decision-making purposes [26].
Extending our knowledge of atherothrombosis
Although relative and absolute risk estimates have been derived for coronary heart disease from Framingham and European populations, fewer studies have been conducted into factors for stroke. Body mass index (BMI), obesity, diabetes mellitus, metabolic syndrome, chronic heart failure, ankle brachial index (ABI), and C-reactive protein (CRP) are all considered CHD risk factors by deduction from combined end-points from cardiovascular studies. However, much less information is available to estimate stroke risk. For example, BMI has only recently been identified as a stroke risk factor in men [28], and no such data are available in women. Using data derived from male medical practitioners participating in the Physicians' Health Study, and evaluating BMI as a continuous variable, each unit increase in BMI was associated with a significant 6% increase in the adjusted relative risks of total, ischaemic, and hemorrhagic stoke [28]. The study authors point out a possible limitation, in that participants were mainly white in origin, all of the same profession, and leaner than the average USA population, again arguing against easy generalization.
Ethnic diversity would be expected to be a relevant factor when considering variation in risk pattern for cerebrovascular disease. Among Asians the risk of cerebrovascular disease exceeds risk of CHD. The reasons for this strong ethnic differentiation remain unclear, although a number of studies have been recently reported examining risk factors for CVD and stroke in Chinese and Japanese population groups [29–31]. Stroke is the most common manifestation of CVD among Chinese men, and accounts for three times the number of deaths as CHD [32]. In a 13.5-year follow-up study of 5092 Chinese males, hypertension was demonstrated to be a greater risk factor for Asians than Caucasians, but did not appear to explain the differing spectrum of CVD among Asians [29]. BMI was also noted to be a risk for ischaemic, but not hemorrhagic stroke [29]. In Japan, a population strategy to reduce blood pressure has been suggested following a 14-year follow-up cohort study that high blood pressure increased risk for death from all causes, CVD, and stroke [30]. Interestingly, mortality due to CHD was significantly related to hypertension for men, but not for women [30]. Although the Japanese have witnessed a significant decline in stroke mortality in their country, especially between 1960-1980, a slowdown in the decline of CVD mortality has been observed more recently. Increased CHD in the elderly, possibly due to insufficient control of hypertension and increased metabolic disorders has been suggested as a reason for this trend [31].
By way of contrast, and as an indication of the atherothrombotic milieu in Europe, a cross-sectional study of 6880 German unselected primary care patients aged 65 years or older, revealed that 19.8% in men and 16.8% in women had PAD, as indicated by an ABI measurement of < 0.9 [33]. In addition to being a distinct atherothrombotic disease, PAD is associated with an elevated risk of cardiovascular and cerebrovascular events, including MI, stroke, and death [1]. The German study showed that presence of an ABI < 0.9 was related to a 70% greater risk for a coronary event and 98% greater risk for a cerebrovascular event (97%), when compared to patients with an ABI ≥ 0.9 [33]. The high prevalence of PAD in this German sample suggests that sub-clinical vascular disease is a significant public health issue that has been underestimated by surveys that only assessed symptoms and did not use newer assessment methods. Comparison of such PAD rates with populations in other geographical areas, such as Japan, would indeed be of particular interest. A recently reported study of civil servants in the UK, which included white participants and those of South Asian origin, suggested that differences in access to medical care were unlikely to explain the social and ethnic differences in CHD revealed in this study group [34]. The reporting investigators called for population-based cohort studies, in which subjects are recruited regardless of contact with medical care, to examine differences in incidence of disease [34].
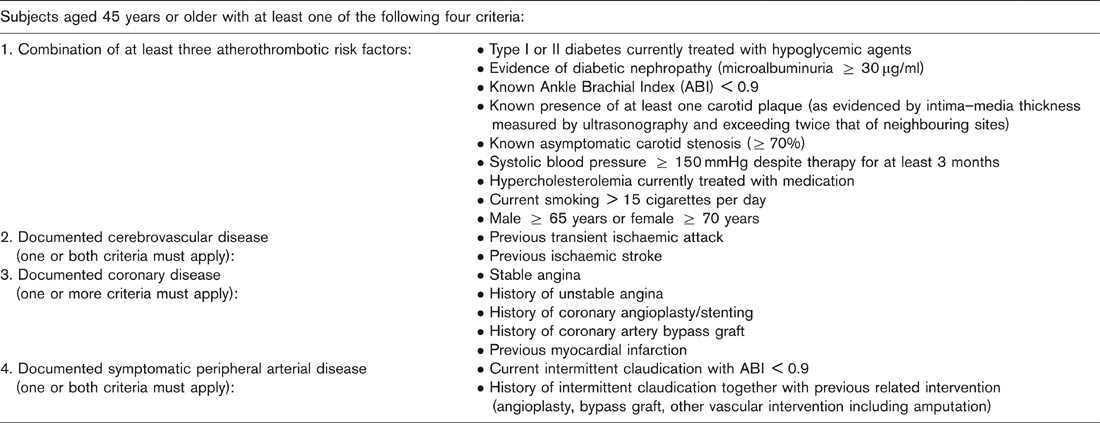
For us to gain valuable insights into the factors that influence the risk of atherothrombotic disease, we need studies that include participants from many regions around the globe, considering adequate representation according to race and ethnicity. Data that were obtained prior to the advent of modern treatments for lipids and blood pressure should be updated with the latest information available, so that we can form the cornerstone of a newer edifice, in order to treat the global epidemic of heart disease that has been predicted for the first quarter of the 21st century. This is the aim of a prospective registry of subjects at high risk of CVD events that was initiated in December 2003. Entitled the Reduction of Atherothrombosis for Continued Health (REACH) Registry, this survey is an international study that has recruited over 63 000 patients in more than 43 countries across Latin and North America, Europe, Asia, The Middle East, and Australia. In order to evaluate long-term risk of atherothrombosis in as broad a spectrum of individuals as possible, participants aged 45 years or older with at least three atherothrombotic risk factors or symptomatic documented cerebrovascular, coronary or PAD were recruited (Table 1). Both those with symptomatic disease and those at risk will be studied for atherothrombotic events, vascular interventions, and death from all causes, for approximately 2 years, in order to give a clear indication of the incidence of morbidity and mortality from atherothrombosis in this population at risk. This survey will allow the assessment of the long-term risk of atherothrombotic events in the total sample and in subgroups. In turn, these comparisons will provide insight into the risk for atherothrombotic events. Socio-economic influences will also be addressed, considering education, access to care, and disease management.
Inclusion criteria for the REACH Registry
Future of risk estimation and disease prevention
Estimation of risk for CVD events is a dynamic field, and the approaches and methods may be modified as newer information is obtained. Novel risk factors stimulate interest in the pathophysiology of the disease, but their use diagnostically may be limited. Often we lack standardized testing, there is large variability in the measurements, newer tests may have a high correlation with existing risk factors, and we may lack validation across multiple studies. Also, cost and benefit for any new test must be carefully considered. Methods to predict and reduce the incidence of atherothrombotic events should be carefully evaluated. It has been estimated that nearly one in two patients presenting for the first time with clinical heart failure dies within 2 years, and that deaths within the first 3 months often occur during initial hospitalization, despite appropriate use of modern medical and other therapies [35]. Thus, preventing or postponing the development of heart failure arising from coronary artery disease by addressing the determinants of atherothrombosis and its complications, would be a more appropriate strategy [35]. Registries, such as REACH, have the ability to raise awareness of atherothrombosis amongst a wide range of physicians, provide a significant opportunity to increase understanding of its prevalence and consequences, and aid the development of effective preventive strategies. Therefore, more effective ‘prophylactic' interventions can be instituted. It has been suggested that incidence of new cases of clinical heart failure could be decreased by 50% or more, by reducing the incidence of new and recurrent chronic coronary artery disease and the underlying determinants of atherothrombosis in the population [35]. Improved risk assessments algorithms provided by a broad spectrum, global study of high-risk individuals, would therefore be expected to provide a pathway to more appropriate therapeutic regimens which will take note of population and ethnic differences.