
Abstract
Background
Smoking cessation is probably the most important single action after a coronary event. In order to increase the effectiveness of smoking cessation programs, it is important to have knowledge of the predictors of smoking cessation. Further, it is unknown whether smoking cessation programs have impact on these predictors.
Methods
Data were obtained from a randomized controlled trial of smoking cessation intervention in 240 smokers aged less than 76 years admitted for myocardial infarction, unstable angina, or cardiac bypass surgery. Baseline characteristics were prospectively recorded. Smoking cessation was determined by self report and biochemical verification at 12 months follow-up.
Results
In multivariate logistic regression analysis, a high level of nicotine addiction, low level of self-confidence in quitting and having previous coronary heart disease were significant negative predictors of smoking cessation at 12 months follow-up. Having previous coronary heart disease and a diagnosis other than acute myocardial infarction as a reason for admission were important negative predictors of abstinence in the usual care group, in contrast to the intervention group, although this did not reach a level of significance in the subgroup interaction analyses. A high level of nicotine addiction was a strong negative predictor in both groups.
Conclusion
A high level of nicotine addiction is an important negative predictor of smoking cessation, even within an individualized smoking cessation program. Smoking cessation intervention seems to be especially effective in patients with previous coronary heart disease and in patients with unstable angina or coronary artery bypass surgery, compared to usual care.
Keywords
Introduction
Smoking cessation in patients with coronary heart disease is associated with a relative mortality reduction of 3545% after 3 to 5 years [1], and this reduction increases further with several years of follow-up [2]. After a coronary event, 30-40% of patients stop smoking spontaneously [3,4]. Randomized investigations of smoking cessation programs in patients with coronary heart disease have obtained mixed results [4–17]. Studies with brief smoking intervention periods and lifestyle intervention studies where smoking cessation issues only were a part of the total intervention, have not shown any statistically significant effects on smoking cessation rates [4–13]. Smoking cessation programs with long intervention periods (4-6 months) have been shown to increase cessation rates significantly [14–17], and is very cost-effective compared to other treatment modalities [18]. However, even with intensive individual programs, 3545% of patients are still smoking at follow-up [14–17]. Only a few studies have assessed the predictors of smoking cessation in patients with heart disease, and the results have been inconsistent [13,19–22].
A better characterization of smokers may help to improve the intervention programs, possibly by delivering personally tailored individualized interventions. We assessed the predictors of smoking cessation in a randomized controlled trial of smoking cessation intervention in patients admitted for acute coronary heart disease.
Methods
Recruitment methods, study methodology and the intervention program have previously been explained in detail [17]. From February 1999 to September 2001, nurses recruited patients 2 to 4 days after admission for coronary heart disease (acute myocardial infarction, unstable angina or recent coronary bypass). Among eligible patients 77% were included in the study. After providing written informed consent and answering baseline questionnaires, the patients were randomly allocated to usual care (control group) or intervention. Doctors were not involved in the programme.
Control group
All patients were offered group sessions in the ward twice a week, where the importance of smoking cessation was mentioned. During these sessions a video was shown and a booklet handed out that contained general information on coronary heart disease and advice on quitting smoking. The control group received no further specific instructions on how to stop smoking.
Intervention group
One of three study nurses consulted the patients once or twice during hospitalization. After discharge, nurses contacted participants by telephone at 2 days, 1 week, 3 weeks, 3 months, and 5 months. Those with special needs (e.g., those who continued smoking or relapsed to smoking) were telephoned monthly thereafter. The intervention was based on a 17-page booklet specially produced for the trial. This booklet emphasized the health benefits of quitting smoking after a coronary event. The booklet also contained information on how to prevent relapse, how to stop smoking for those who had relapsed or not stopped while hospitalized, and how to use nicotine replacements. How to identify and cope with high-risk situations for relapse was also explained. Spouses who smoked were also asked to give up.
Explanatory and outcome measures
The study nurses prospectively recorded medical history and socio-demographic data. The participants filled in three questionnaires before randomization, containing information on smoking habits, nicotine addiction and self-efficacy in smoking cessation. The Fagerstom Tolerance Questionnaire was used to provide an index of physical nicotine addiction [23]. This questionnaire cover eight items of various aspects of smoking behaviour (number of cigarettes smoked per day, time of day most smoking occur, brand smoked, ability to control smoking in non-smoking areas, smoking while laying in bed because of sickness and whether the smoke is inhaled).
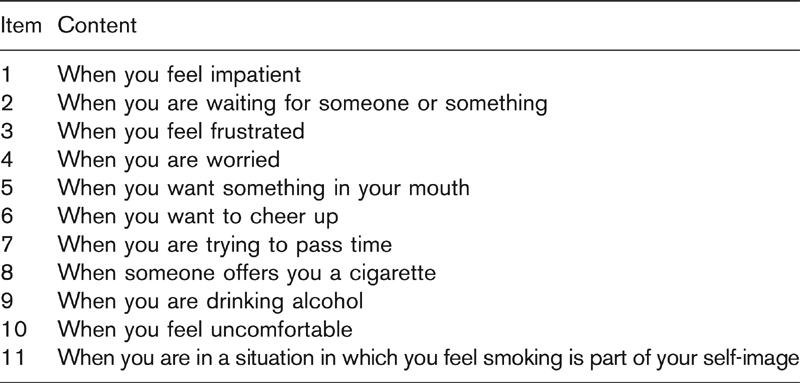
The level of nicotine abstinence while hospitalized was assessed with a scale ranging from none (1) to very much (5). To measure the patients' level of confidence in their ability to quit smoking, a self-efficacy questionnaire as developed by Yates and Thain, was employed (Table 1) [24]. A Likert scale was used with judgements ranging from completely unsure (1) to completely sure (7) that the subjects could resist smoking in each of 11 situations. In addition, their overall confidence to quit and their overall intention to quit smoking were assessed with a discrete numerical scale ranging from 1 (in doubt) to 10 (very strong).
At 1-year follow-up, those who claimed to be quitters and had a nicotine metabolite concentration in their urine below a cut-off value consistent with abstinence, were classified as non-smokers. All others were classified as smokers. The patients' use of nicotine substitutions and their partners' smoking status were also registered at 12 months follow-up.
Statistical methods
The χ2 test was used to assess the differences between groups when variables were categorical. The differences in means were assessed with independent samples t-tests, after confirming that the continuous variables were normally distributed by the Lilliefors' test. All tests were two-tailed, with a significance level (alpha) of 0.05 and confidence interval of 95%. Univariate and multivariate logistic regression models were used to test the relations between baseline characteristics (covariates) and the nicotine-validated smoking cessation rates at 12 months (dependent variable). Continuous variables were assessed as continuous covariates if not stated otherwise. Variables showing significant correlation in univariate analysis were included in the multivariate tests. Interaction terms were added to the logistic regression analyses to examine if the influence of the covariates on the dependent variable differed significantly in the control and intervention groups (subgroup interaction analysis). The covariates ability to predict the percentages of abstainers were assessed using the best combination of the covariates as suggested by the SPSS matrix. When calculating the Fagerstrom tolerance score and the self-efficacy score, single missing values in the questionnaires were replaced by case means (the mean of the other answered questions by the same patient) if no more than two answers in a questionnaire were missing. If more than two values were missing, cases were excluded. Except for the intention to treat analyses, drop-outs were excluded from analysis due to lack of outcome data. SPSS for Windows (version 12.0; SPSS Inc., Chicago, Illinois, USA) was used for all analyses.
The self-efficacy questionnaire The patients were asked how confident they were to resist smoking in the following situations. The pre-printed alternatives for answering were ranked from 1 (completely unsure) to 10 (completely sure)
Results
Details regarding the participants' flow through the trial have been shown elsewhere [17]. Two hundred and forty patients were assigned either to the intervention (n = 118) or the usual care/control group (n = 122). One hundred patients in the intervention group and 118 patients in the control group were available at 12 months follow-up, giving a total drop-out rate of 9%.
Baseline characteristics
Apart from working status, there were no statistically significant differences between the two groups at baseline (Table 2).
Smoking cessation rates
The validated smoking cessation rates at 12 months were 57% in the intervention group and 37% in the control group [absolute risk reduction 20%, 95% confidence interval (CI) 6-33%].
Predictors of abstinence
Univariate logistic regression analyses were applied to all baseline characteristics shown in Table 2, analyzing control and intervention groups combined without adjustment for treatment allocation. Being employed, absence versus occurrence of previous coronary heart disease, having myocardial infarction as reason for admission, number of days spent in the intensive care unit, the self-efficacy score and confidence to quit smoking were statistically significant positive predictors of abstinence at 12 months follow-up. The Fagerstrom Tolerance score and smoking first cigarette within 30 min of waking were significant negative predictors.
Having a partner who smoked at baseline did not predict smoking cessation in univariate analysis. However, if the partner was still smoking at 12 months follow-up, this was significantly associated with continued smoking (odds ratio 1.9; 95% CI 1.1-3.3; univariate analysis). Nicotine abstinence while hospitalized was not associated with smoking cessation.
Among the eight questions in the Fagerstrom Tolerance score, only ‘smoking first cigarette within 30 min of waking' and ‘smoking more in the morning than later in the day' were significantly associated with smoking cessation in multivariate analysis. Not smoking first cigarette within 30 min of waking had higher significance level than ‘smoking more later in the day' (odds ratio 2.3; 95% CI 1.3-4.1; and odds ratio 2.0; 95% CI 1.0-3.8; respectively), and predicted as many abstainers as the Fagerstrom Total score (61.5 and 61.0%, respectively). Among the 11 items in the self-efficacy questionnaire, none reached any level of statistical significance in the multivariate tests. Further, the total self-efficacy score was not better than the single question of how confident the patients were in stopping smoking, in predicting smoking cessation (63.0 and 62.9%, respectively). Thus, for simplicity (two questions instead of 19) we chose the items ‘smoking first cigarette within 30 min of waking' as a measure of nicotine addiction, and the single question of how confident the patients were in stopping smoking as a measure of self-confidence, in further analyses.
Baseline characteristics of patients with coronary heart disease assigned to a smoking cessation program or usual care (control group). Values are numbers (percentages) of patients unless stated otherwise
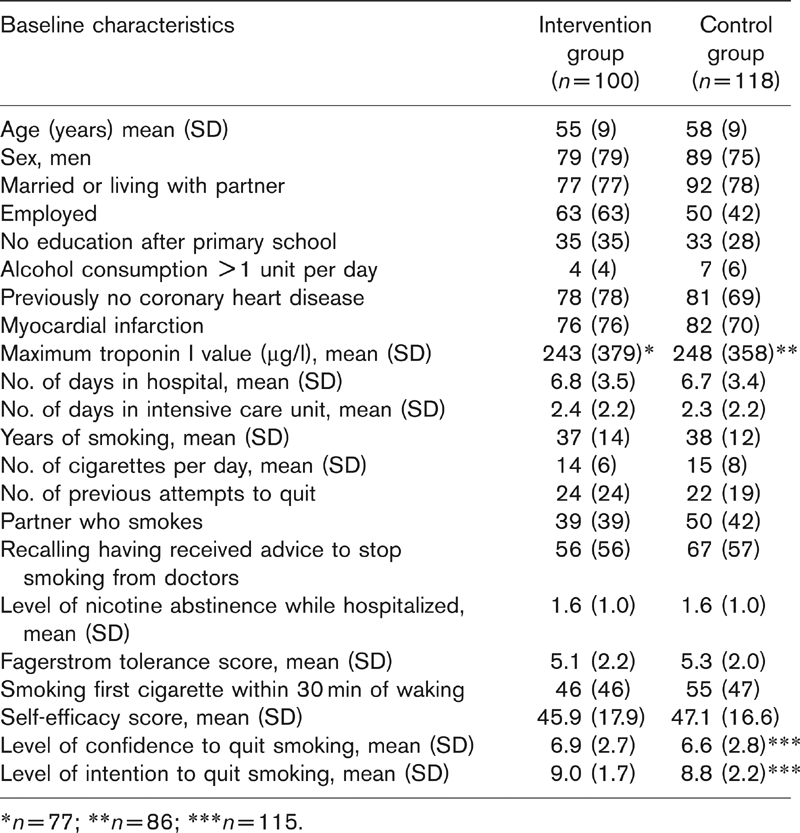
∗n = 77; ∗∗n = 86; ∗∗∗n = 115.
In the multivariate logistic regression analysis, having no previous coronary heart disease, not smoking the first cigarette within 30 min of waking, and confidence to quit smoking were statistically significant positive predictors of smoking cessation at 12 months (Table 3). Using the best combination of these three variables, smoking status at 12 months could be predicted in 66% (70% of those who relapsed and 62% of the abstainers). In patients scoring less than seven on confidence to quit smoking, having previous coronary heart disease and smoking their first cigarette within 30 min of waking, none (0/12) managed to be free of smoking at 12 months follow-up, compared to 80% (41/51) of patients with none of these three predictors.
Predictors of smoking cessation 12 months after admission for coronary heart disease. Multivariate analysis of baseline characteristics being significant in univariate analyses is presented
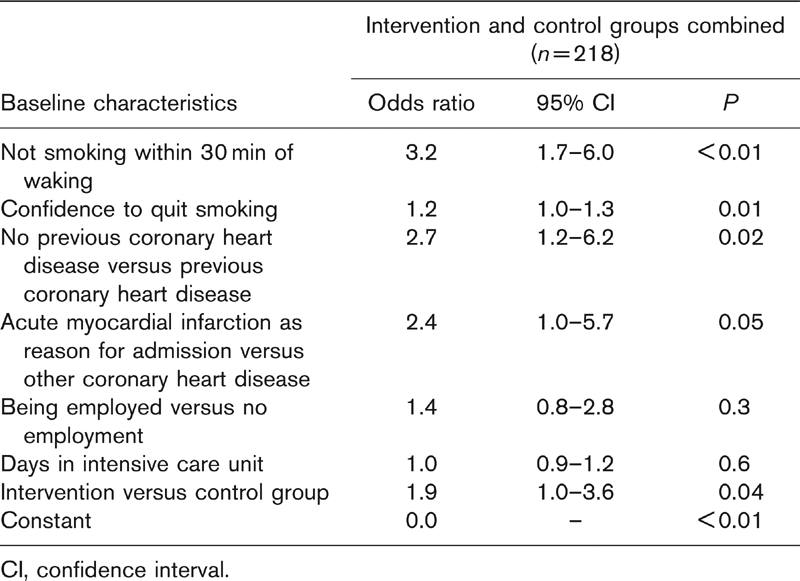
CI, confidence interval.
In an intention to treat analysis, excluding those who died or changed address (n = 7), assuming all other drop-outs returned to smoking, smoking first cigarette within 30 min of waking and confidence to quit smoking, both remained significantly associated with smoking cessation in multivariate analysis (n = 233).
Predictors in intervention versus control group
Additional logistic regression analyses were performed in the control and intervention groups separately. Having previous coronary heart disease and a diagnosis other than myocardial infarction as the reason for admission were strong negative predictors for 12 months smoking cessation in the control group, both in univariate and multivariate analyses, but not in the intervention group, where the odds ratios being about three times higher in the control group than the intervention group. If having previous coronary heart disease and/or a diagnosis other than myocardial infarction as reason for admission, only 18% managed to quit in the control group compared with 42% in the intervention group. However, when analyzing previous coronary heart disease and/or myocardial infarction as a reason for admission in the subgroup interaction analyses, none reached level of significance, possibly due to small group sizes.
Regarding the other predictors, there were only small differences in adjusted odds ratios between the two groups. Smoking a first cigarette within 30 min of waking was a strong negative predictor in both groups (adjusted OR 3.3 and 2.4 in the intervention and control groups, respectively).
Discussion
In this randomized controlled trial of patients with acute coronary heart disease, we have shown that three parameters can be used as predictors of smoking cessation: previous coronary heart disease, the level of nicotine addiction and the level of self confidence in smoking cessation. Further, we hypothesize that these predictors can be assessed by three simple questions on these topics:
having previous coronary heart disease
smoking first cigarette within 30 min of waking and
scoring less than seven on confidence to quit smoking (scale 1-10).
When analyzing the intervention and control groups combined, 80% of patients with none of these negative predictors stopped smoking. A high level of nicotine addiction seemed to be the strongest overall negative predictor, while having previous coronary heart disease and another diagnosis other than myocardial infarction as a reason for admission were especially important in the control group.
Previous studies have confirmed that the level of self confidence in smoking cessation (as assessed by total self-efficacy score) [14,15,25], low level of nicotine addiction [10], having no previous heart disease [21], and having myocardial infarction versus other coronary diseases [10] are significant positive predictors of abstinence. Whether a smoking cessation program has any impact on these predictors has not previously been investigated. Our results indicate that such a program may influence some of these predictors (e.g., having previous coronary heart disease and myocardial infarction as reason for admission).
No socio-demographic features at baseline (including having a smoking partner) could significantly predict smoking cessation. However, having a partner who still smoked at 12 months follow-up was significantly associated with decreased cessation rates, underscoring the importance of including partners in intervention programs. Interestingly, the physicians' involvement did not seem to matter, since recalling versus not recalling to have received advice to stop smoking from doctors during the acute coronary episode did not predict abstinence at 12 months follow-up. Further, in contrast to others [4,10,13], we did not find intention to quit smoking as a significant predictor.
In patients with high levels of nicotine addiction, as assessed by smoking their first cigarette within 30 min of waking, the cessation rates were low in both groups (41 and 27% in the intervention and control group, respectively). Bupropion as a single agent has recently been shown to be safe in cardiac patients [26]. Bupropion was not available at the start of our study, and only one-third of patients used nicotine replacements. Giving nicotine replacements and/or bupropion to all patients with high levels of nicotine addiction could maybe have increased the quit rates in this high-risk group.
In our trial, the baseline characteristics were recorded before randomization, and most were abstainers while these data were recorded (only one of five was smoking while hospitalized). Therefore, neither the outcome nor the randomization status have flawed the baseline recordings. Most smoking patients were included in the study, and the total drop-out rate of less than 10% was lower than in comparable studies [14,15]. The results should therefore be applicable to an ordinary clinical setting. However, the drop-out rate was higher in the intervention group than in the control group. This may have been a result of the intervention itself, even though half of the patients stated they had stopped smoking at time of withdrawal. In the intention-to-treat analyses, assuming all drop-outs returned to smoking, the predictors were slightly changed. When analyzing predictors it is important to have accurate knowledge of the outcome. Therefore, our conclusions are based on the analyses of those available at 12 months follow-up with biochemically-validated cessation rates.
To summarize, our study has shown that having previous coronary heart disease, having a low level of self confidence in quitting and having a high level of nicotine addiction are important negative predictors of smoking cessation in patients admitted for coronary heart disease. A smoking cessation program with emphasis on fear arousal and with several months of intervention seems to be especially effective in patients with previous coronary heart disease and in patients with unstable angina or coronary artery bypass surgery. We need more studies on patients with high levels of nicotine addiction or low levels of self confidence in giving up in order to explore what kind of programs are best suited for these patients. Possibly, personally tailored, individualized interventions with formal use of nicotine replacements would increase cessation rates in these patients.
Footnotes
Acknowledgements
Paal Friis, Kjetil Drangsholt, Finn Tore Gjestvang, Tone Baeck, Eva Boroey and Anders Wahlstedt for contributing to the planning of the study. Tone Baeck, Eva Boroey and Anne Kari Kjellesvik for delivering the intervention and collecting data. The main result of the trial (the smoking cessation rates) has already been published [![]() ]. Funding was from Vest-Agder Council for Public Health, the charity ‘Sykehuset i vaare hender' and Sorlandet Hospital HF.
]. Funding was from Vest-Agder Council for Public Health, the charity ‘Sykehuset i vaare hender' and Sorlandet Hospital HF.