
Abstract
Background
Smoking cessation is probably the most important action to reduce mortality after a coronary event. Smoking cessation programs are not widely implemented in patients with coronary heart disease, however, possibly because they are thought not to be worth their costs. Our objectives were to estimate the cost effectiveness of a smoking cessation program, and to compare it with other treatment modalities in cardiovascular medicine.
Methods
A cost-effectiveness analysis was performed on the basis of a recently conducted randomized smoking cessation intervention trial in patients admitted for coronary heart disease. The cost per life year gained by the smoking cessation program was derived from the resources necessary to implement the program, the number needed to treat to get one additional quitter from the program, and the years of life gained if quitting smoking. The cost effectiveness was estimated in a low-risk group (i.e. patients with stable coronary heart disease) and a high-risk group (i.e. patients after myocardial infarction or unstable angina), using survival data from previously published investigations, and with life-time extrapolation of the survival curves by survival function modeling.
Results
In a lifetime perspective, the incremental cost per year of life gained by the smoking cessation program was ∊280 and ∊110 in the low and high-risk group, respectively (2000 prices). These costs compare favorably to other treatment modalities in patients with coronary heart disease, being approximately 1/25 the cost of both statins in the low-risk group and angiotensin-converting enzyme inhibitors in the high-risk group. In a sensitivity analysis, the costs remained low in a wide range of assumptions.
Conclusions
A nurse-led smoking cessation program with several months of intervention is very cost-effective compared with other treatment modalities in patients with coronary heart disease.
Keywords
Introduction
Smoking cessation after a coronary event is associated with a 35–45% relative mortality reduction after 5 years [1], and this reduction increases further with longer follow-up periods [2]. Only 30–40% stop smoking spontaneously after a coronary event [3–5]. Despite randomized trials have shown significantly increased quit rates when applying a smoking cessation programs with several months of intervention [3–5], many hospitals do not provide such programs as part of routine care, possibly because they are thought not to be worth their costs.
To our knowledge, no cost-effectiveness analysis on smoking cessation programs after coronary revascularization have been published. In patients suffering myocar-dial infarction, a 12-year-old analysis found a smoking cessation program to be relatively cost effective, but their analysis was based on an investigation sponsored by the tobacco industry and a smoking cessation program using a complicated psychological approach [6].
We recently conducted a randomized smoking cessation intervention trial in patients admitted for coronary heart disease [4]. The purpose of the present analysis was to determine the incremental cost effectiveness of the smoking cessation program in patients with low (i.e. stable coronary heart disease) and high (i.e. after myocardial infarction) cardiovascular risk, and to compare it with other treatment modalities in patients with coronary heart disease. The gain in life expectancy in quitters was estimated on the basis of survival data from studies with a large number of patients and with several years of follow-up [2, 7].
Methods
The smoking cessation program
From 1999 to 2001, 240 smokers under 76 years of age were randomly allocated to a smoking cessation program or usual care after admission for acute myocardial infarction (n = 176), unstable angina (n = 36) or recent coronary bypass surgery (n = 28). The smoking cessation program was based on a booklet especially made for the purpose of the trial. The intervention focused on fear arousal messages and positive feedback, and was delivered by cardiac nurses without special training in smoking cessation. The intervention was initiated in hospital, and the patients were telephoned regularly for at least 5 months. Doctors were not involved in the program. Smoking cessation rates were determined by self-report and biochemical verification at 12 months follow-up. Further details regarding enrolment, the intervention program and outcome measures have been explained elsewhere [4].
Cost of the program
The costs were calculated on the basis of Norwegian prices in 2000 and were converted to Euros at the 2000 mean exchange rate (∊1=8.1 Norwegian Krones, NOK). The nursing costs were estimated from the average salary of specialized nurses in Norway with more than 10 years of seniority (190 NOK/h). Because cardiac nurses without special training in smoking cessation counseling were used, no educational costs were included. A booklet was especially made for the trial, and only the printing costs (17 NOK per booklet) were included, because once made the booklet can be used nationwide without further production costs. The office rental was set to 1500 NOK per square meter per year (including overhead costs such as heating, electricity, cleaning and maintenance, obtained from the Foundation for Scientific and Industrial Research at the Norwegian Institute of Technology). The premises were used in many other objectives, and only the average time devoted to each patient participating in the smoking cessation program was included in the rental estimation. The costs of telephoning were calculated using the prices of the telephone company Telenor (0.89 NOK per call +0.49 NOK per minute). Because the expenses of the program only lasted for less than a year, discounting was not performed regarding the costs.
Indirect costs (i.e. time lost from work while participating in the program) were not included in analysis because the intervention after discharge from hospital were brief and mostly by phone. As there were no significant differences between the control group and intervention group regarding the use of nicotine replacements, they were not included in analysis [4].
Life expectancies, low-risk model
We modeled the cost effectiveness of the smoking cessation program in a low-risk setting using survival data from the van Domburg investigation [7]. In this study, the average annual mortality rate was 1.7% at 10 years follow-up, which is similar to the mortality rate in the Scandinavian simvastatin survival study (4S) of patients with stable coronary artery disease [8]. Van Domburg et al. [7] retrieved smoking habits with a questionnaire sent by mail a median of 2.8 years after the surgery in 985 patients who underwent coronary bypass surgery during the 1970s. No biochemical verification of the quitters was performed. The mean age of the patients who were smokers at time of bypass surgery (n =556) was 51 years. The differences in mortality between the persistent smokers and the quitters increased throughout the follow-up period and after a median follow-up period of 20 years, 46% had died among the 238 quitters versus 64% among the 318 persistent smokers. This relative risk reduction of 28% was lower than in comparable investigations [1]. The Kaplan–Meier method was used for analyzing the survival data for the first 20 years [7]. We extrapolated the survival curves further using the Gompertz parametric survival function [9] adjusted to agree with the survival at the 10-year and 20-year follow-up points (Fig. 1).
Life expectancies, high-risk model
Patients suffering myocardial infarction or unstable angina were chosen as the high-risk group. There are no recent studies with a long follow-up period and with proper verification of quitters, investigating the mortality benefit of quitting smoking in these patients. Therefore, the Daly investigation [2] was chosen when calculating the survival differences in quitters and sustained smokers in a high-risk setting. In this study, the mortality was similar to the annual mortality rate of 4.5% found in patients after thrombolysis for myocardial infarction [10]. Only patients (n = 498) surviving the first 2 years after myocardial infarction or unstable angina were included. The mean age was 51 years, and the mean follow-up period was 7.4 years. Smoking status was verified annually, and biochemically validated on a sub-sample. Survival curves were estimated for 13 years using life table methods. The mortality in those who continued to smoke was 82%, versus 37% in those who stopped smoking (a 55% relative risk reduction). The mortality rates among quitters were stable between 11 and 13 years in the Daly data (Fig. 2), and in order not to overestimate the survival benefit in quitters, we estimated survival curves beyond 11 years, instead of 13 years, by calculating the average mortality from years 5.5 through 11, and assuming the survival followed an exponential function with this mortality thereafter (the declining exponential approximation of life expectancy [11]).
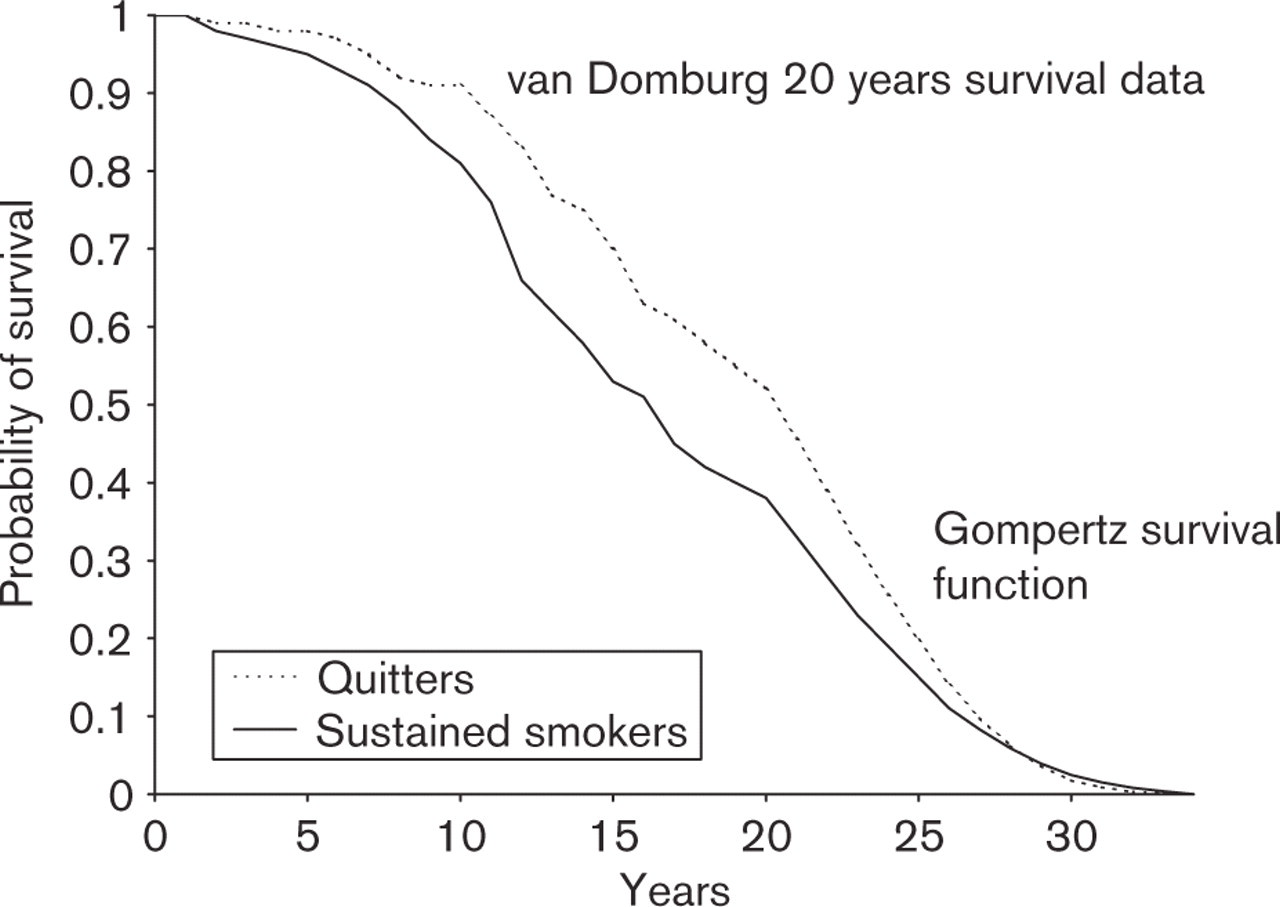
Low-risk model. Probability of survival after coronary bypass surgery in patients who quit smoking (quitters) and in patients who continue to smoke (sustained smokers). The survival curves are based on data from van Domburg et al. [7] for the first 20 years, and Gompertz parametric survival function [9] for the period after 20 years.
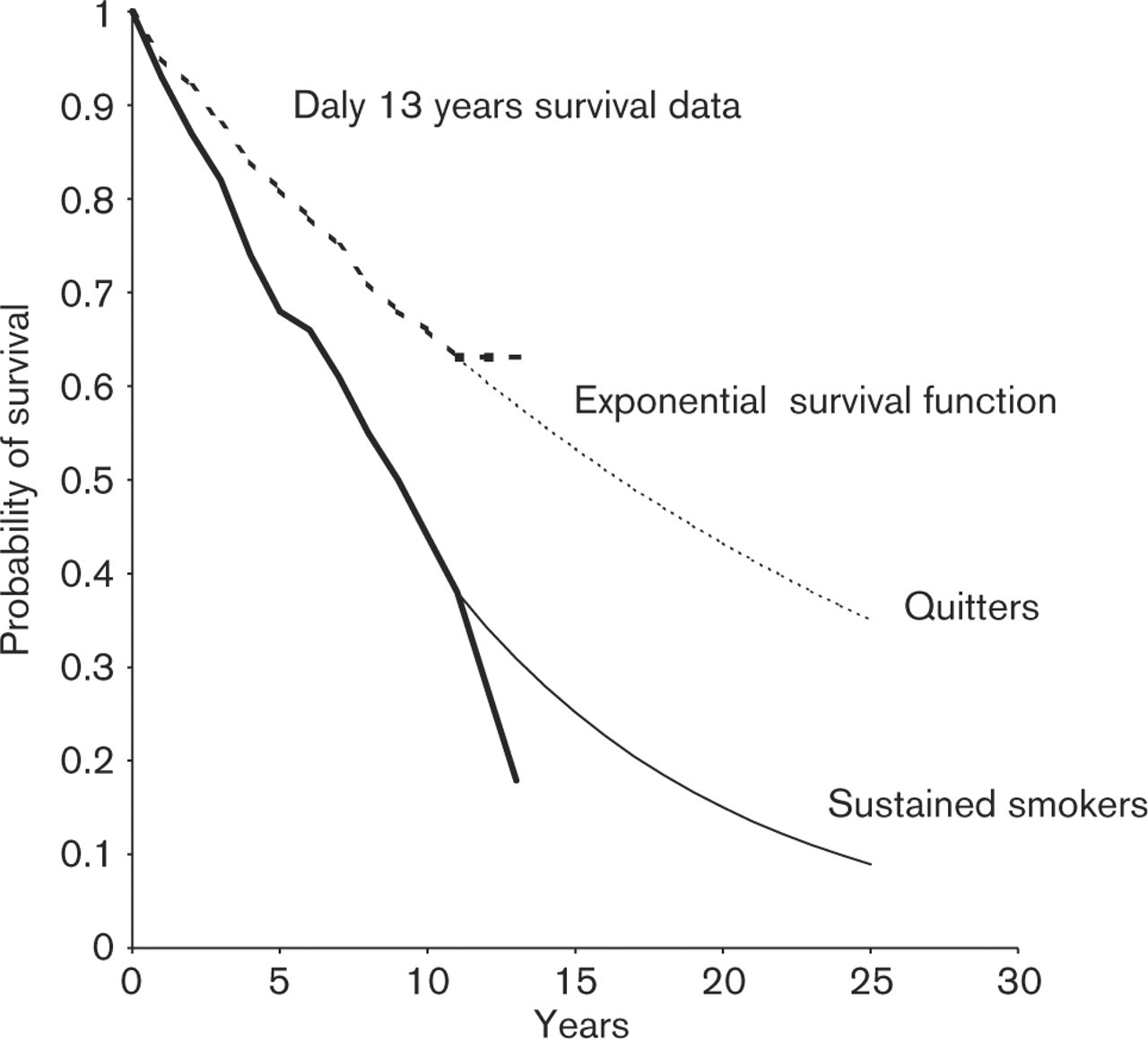
High-risk model. Probability of survival after myocardial infarction or unstable angina in patients who quit smoking (quitters) and in patients who continue to smoke (sustained smokers). The survival curves are based on data from Daly et al. [2] for the first 11 years, and the exponential survival function [11] from 11–25 years (lifetime).
Calculation of cost effectiveness
The incremental cost effectiveness of the program was assessed as the cost per life year gained, and was calculated using the following formula: cost of program per patient × number needed to treat (NNT) ÷ gain in mean discounted life years per patient.
The number needed to treat (NNT) to get one additional quitter from the smoking cessation program was assumed to be equal in the low and high-risk groups, and was derived from the absolute risk reduction (ARR) in smoking rates in the intervention group compared with the usual care group at 12 months follow-up (NNT = 100/ARR) [4]. The gain in mean discounted life year per patient in quitters compared with sustained smokers was obtained from the differences in integrals between the survival curves of quitters and sustained smokers from year i to year i + 1, multiplying that by 1/1.05 i (5% discounting per year [12]) and summing for i values of 1 to 40 in the low-risk model and i values of 1 to 25 in the high-risk model. A short time perspective (5 years) was also set up, summing for i values of 1 to 5.
A sensitivity analysis was performed in the low-risk model by increasing the calculated cost of the program, by increasing the NNT to get one additional quitter from the smoking cessation program, and by reducing the estimated gain in life expectancy in quitters.
Results
As previously published [4], the 12 months abstinence rates were 37% (44/118) and 57% (57/100) in the usual care group and intervention group, respectively (P = 0.004), and the NNT to get one additional patient to quit smoking was 5.0 (95% confidence interval 3–16). Among the patients undergoing coronary bypass surgery, five of eight patients were abstinent in the intervention group compared with two of 18 in the usual care group (P = 0.006). The average time devoted to each patient, including time to fill in questionnaires for the purpose of the trial, was 147 min (SD 50, 42 min while hospitalized and 105 min after discharge). The mean number of telephone calls was 8.5 (SD 3.2) per patient.
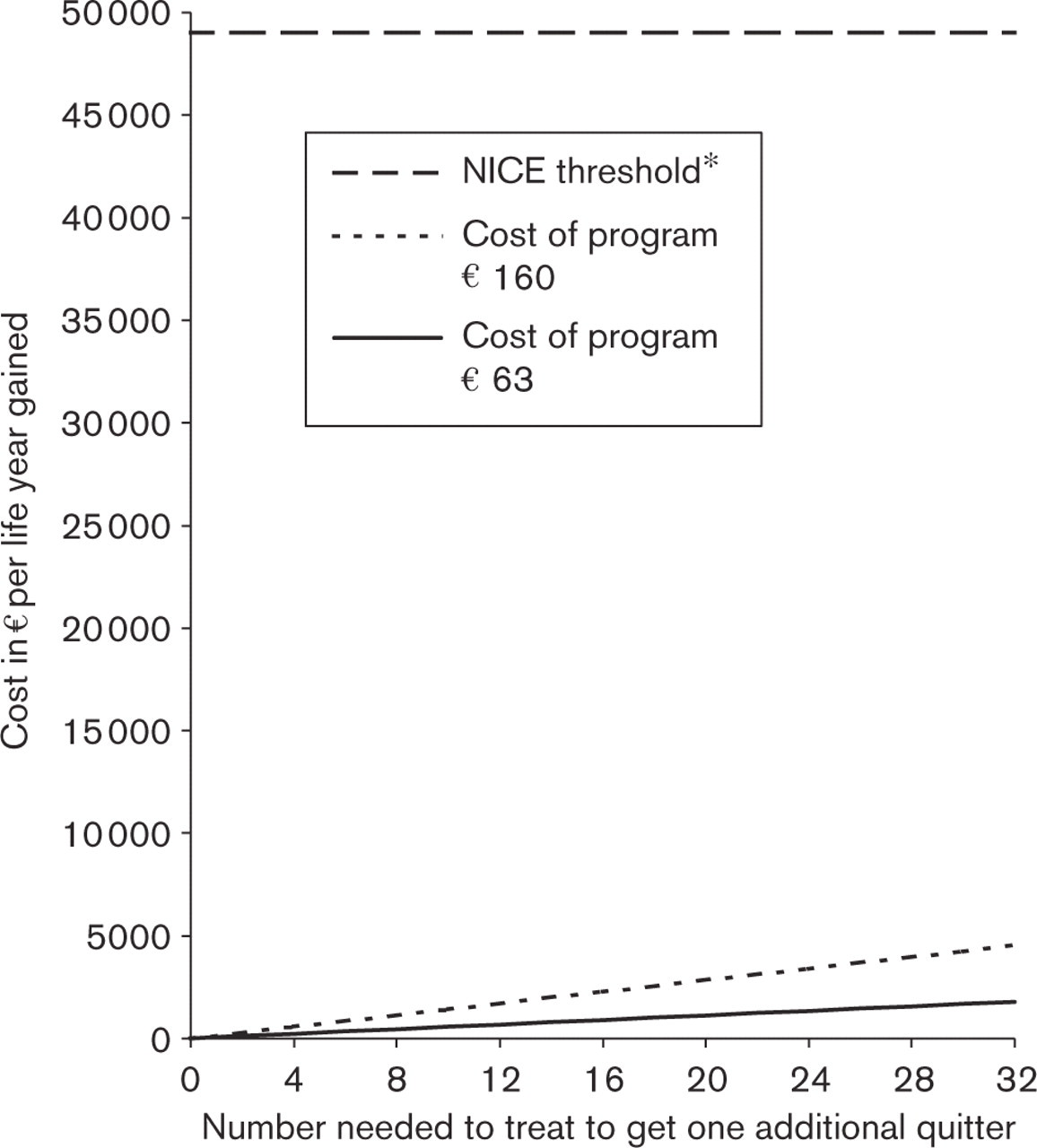
A sensitivity analysis of the cost effectiveness of the smoking cessation program in the low-risk group, and in the life-time perspective. Even if the number needed to treat to get one additional quitter from the program is 32 (two times the upper limit of the 95% confidence interval) and the cost of program 160 (baseline assumption ∊63), the program remains very cost-effective compared with the threshold of what has been proposed to be an acceptable cost per life year gained by the policy makers. ∗The acceptable cost per life year gained as proposed by the UK National Institute for Clinical Excellence (NICE) [15].
The direct cost of the program per patient was derived from the salary to study nurses (465 NOK), the cost of telephoning (8 NOK), the cost of office rental (20 NOK), and the cost of the booklet (17 NOK), summing to 510 NOK (∊63).
Low-risk group
The mean discounted life years gained per patient in quitters compared with sustained smokers in the low-risk model were 0.06 at 5 years (van Domburg data), 0.97 at 20 years (van Domburg data), and 0.16 for the period from 20–40 years (Gompertz's survival function), summing to 1.13 in the lifetime perspective (until all patients were dead at 40 years follow-up). In the baseline assumption (NNT=5.0 and cost of the program = 510 NOK (∊63) per patient), the incremental cost effectiveness of the program became 42 500 NOK (∊5230) and 2300 NOK (∊280) per life year gained at 5 years and in the lifetime perspective, respectively.
In the lifetime perspective, the cost of saving one additional year from the program was approximately 1/22 of statins in patients with stable coronary heart disease [13], and 1/44 of aspirin in patients with coronary artery disease (Fig. 4) [14].
Sensitivity analysis, low-risk group
Even if the NNT were set to the upper limit of the 95% confidence interval (i.e. NNT 16), and the cost of the program was increased to 1300 NOK (∊160), the cost per life year gained remained low at 1/20 the threshold of what has been proposed to be an acceptable cost per life year gained by the UK National Institute for Clinical Excellence (NICE) (Fig. 3) [15].
If no further gains in life expectancy in quitters compared with sustained smokers were assumed after 20 years (i.e. from the extrapolated parts of the survival curves), the program remained very cost effective at 2600 NOK (∊320) per life year gained.
Using the 3.5% discount rate as proposed by the latest guidelines from NICE [16], instead of the 5% used in the baseline assumption, the cost per life year gained in the low-risk model was reduced from ∊280 to ∊230.
High-risk group
The mean discounted years of life gained per patient in quitters compared with sustained smokers in the high-risk model were 0.26 at 5 years (Daly data), 0.95 at 11 years (Daly data), and 1.83 for the period from 11 to 25 years (exponential survival function), summing to 2.77 in the lifetime perspective (25 years). This gave an incremental cost for each additional year of life saved of 9800 NOK (∊1200) and 900 NOK (∊110) in the 5-year and lifetime perspective, respectively.
Compared with other treatment modalities in patients after myocardial infarction the cost per life year gained from the program in the lifetime perspective was 1/28, 1/35 and 1/55 the cost of angiotensin-converting enzyme inhibitors [17], cardiac rehabilitation [18] and β-blockers [17], respectively.
Discussion
The analyses presented in this paper show that a smoking cessation program is very cost effective in terms of cost per life year gained compared with other treatment modalities in patients with coronary heart disease, even when applying a program with simple intervention principles and in a low-risk group.
Three randomized studies in patients admitted for myocardial infarction have documented that the NNT of a smoking cessation program with several months of intervention is approximately five [3–5]. The NNT of similar programs in patients after coronary revascularization and unstable angina is less well documented, but in our study the intervention seemed to be especially effective in these patients compared with patients suffering myocardial infarction [19]. In previous smoking cessation trials, a psychological approach with especially trained personnel was used [3, 5]. In order to increase the applicability of the program, we applied simple intervention principles with focus on fear arousal and positive feedback delivered by nurses without special education in smoking cessation [4]. Further, most patients motivated to quit smoking were included in the program [4]. Therefore, we believe the analyses presented in this paper can be generalized to an ordinary clinical setting.
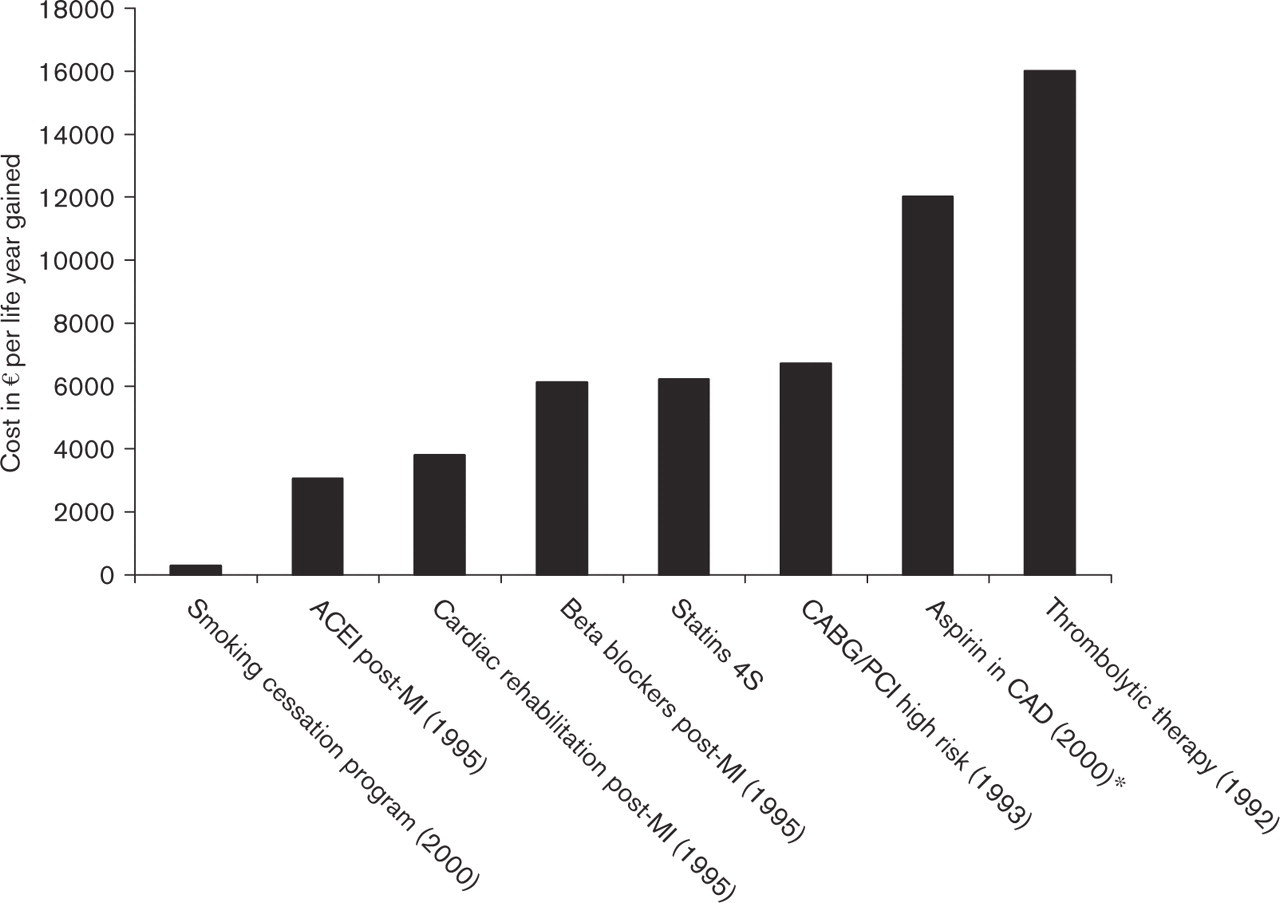
Comparison of the cost effectiveness of the smoking cessation program in the low-risk group with other treatment modalities in patients with coronary heart disease. Estimates are in the life-time perspective and the comparisons do not give an exact picture of today's situation because the prices of most of the pharmaceuticals have fallen since their respective cost-effectiveness analyses were performed. Estimates from studies before year 2000 are in 1995 ECU. MI, myocardial infarction; ACEI, angiotensin-converting enzyme inhibitor; CAD, coronary artery disease; CABG, coronary artery bypass surgery; PCI, percutaneous coronary intervention. ∗Cost per quality adjusted life year gained. Data from Gaspoz et al. [14], Probstfield [17], Ades [18] and Malik [22].
As the years go by, patients may resume smoking and hence diminish the effect of the program. Relapse to smoking is infrequent, however, after 1 year of abstinence [20]. Furthermore, both in the low and high-risk settings the program was cost effective even in a short time perspective (i.e. 5 years), being approximately 1/10 and 1/40, respectively, of the NICE threshold [15].
A substantially reduced rate of readmission due to myocardial infarction and stroke has been reported in quitters compared with sustained smokers after a coronary event [21], and such savings have been included in most cost-effectiveness analyses in cardiovascular medicine [14, 18, 22]. Because estimation of these savings are hampered by uncertainty due to lack of randomized trials, and because the savings may be outweighed by increased medical costs during the years of life gained, they were not included in our analyses.
It is both unethical and impossible to randomize patients to continued smoking or smoking abstinence after a coronary event. Therefore we are left with observational data, which are often misleading. Smokers with their first coronary event tend to be younger and with fewer concomitant cardiac risk factors than non-smokers [23]. Therefore, their initial prognosis may be more favorable than non-smokers (‘smokers paradox') [23]. Thus, significant differences in mortality between quitters and persistent smokers may take several years to develop. Further, many smokers do not tell the truth about their smoking behavior [24], and many return to smoking within a year [20]. These biases tend to underestimate the measured effect of smoking cessation, and the true effect of smoking cessation might be greater than the relative mortality reduction of 36% 5 years after a coronary event found in a meta-analysis of 20 studies [1]. In the van Domburg data [7], smoking status was assessed only once and was not verified biochemically. Further, it was assessed at a median of 2.8 years after the surgery, at which time 6.2% already had died. These factors may have underestimated the survival benefit in quitters. Thus, the low-risk model with a 28% mortality reduction after 20 years is probably a conservative assumption.
Since van Domburg [7] and Daly [2] investigations were performed, new treatment modalities have emerged (i.e. acute percutaneous interventions and statins), which have reduced the overall mortality after a coronary event. Both studies only included a selected group of young patients with a mean age of 50 years, however, and the mortality rates were or similar to more recent trials [10, 25, 26], indicating that the gain in life expectancy if quitting smoking in an unselected group of patients today is similar or higher than in the models used.
As the follow-up period increases, the life years gained in quitters are encumbered with uncertainty. The life expectancies calculated from the extrapolated parts of the survival curves are only rough estimates. Mainly due to discounting, however, the years of life gained derived from these parts of the survival curves only represented a small part of the total life years gained if quitting (i.e. 14% in the low-risk model). Regarding the high-risk model, the exponential approximation of life expectancy did not have a perfect fit to the Daly data. The Gompertz survival function seemed to fit the Daly data somewhat better (figures not shown), but gained higher differences in survival between quitters and sustained smokers. Therefore, in order to avoid overestimation of the survival benefit in quitters, the exponential survival function was chosen. This method has been validated as an appropriate technique in situations in which mortality is dominated by a single disease process [11]. The method assumes a constant mortality rate and tends to overestimate the survival of patients, and thus possibly also overestimated the life years gained in quitters. To avoid this, no further survival benefits were assumed beyond 25 years, even though the probability of still being alive was over 30% among quitters at this point.
For total assessment of a health outcome, it is recommended to adjust life expectancy for quality of life (cost utility analysis) [12]. To our knowledge, no cost utility analysis in patients with coronary heart disease have been performed on smoking cessation programs. At 1-year follow-up we measured life satisfaction by a 10-step ‘ladder of life', showing no significant differences between the sustained smokers and the quitters either before or after adjustments for baseline characteristics (results not shown). This indicates, at least in a short time perspective, that adjustments for quality of life would not alter the results.
For several reasons we believe we may have underestimated the cost effectiveness of the smoking cessation program. First, the cost of the program was probably overestimated by including time to fill in questionnaires for the purpose of the trial. Second, conservative original data were used in the low-risk model. Third, the lifetime was shortened to 25 years in the high-risk model. Fourth, a relatively high discount rate was used [16]. Finally, savings from reduced hospitalizations in quitters were not included. Still, the smoking cessation program was very cost effective, even in a wide range of assumptions, compared with other treatment modalities in patients with coronary heart disease (Fig. 4). In the low-risk group, the cost effectiveness was approximately 1/16 of ramipril in the Heart Outcomes Prevention Evaluation (HOPE) population [22] and 1/22 of simvastatin in patients with stable coronary heart disease [13]. In patients suffering myocardial infarction or unstable angina (the high-risk group), the program was even more beneficial (i.e. 1/55 of β-blockers after myocardial infarction [17]), and the cost per life year gained was somewhat lower than in the study by Krumholz et al. [6]. These comparisons do not give a correct picture of today's situation, however, because the prices of most of the pharmaceuticals have fallen since their respective cost-effectiveness analyses were performed.
Many healthcare providers give brief smoking cessation counseling in hospital or as part of a rehabilitation program. Unfortunately, these types of smoking cessation interventions are of no proven benefit [27, 28]. In order to increase quit rates, a program addressing only smoking cessation and with several months of intervention is necessary [3–5]. On the basis of the analyses presented in this paper, we suggest that such programs should be provided as part of routine care in wards dealing with cardiac patients.
Footnotes
Acknowledgements
Tone Baeck, Eva Boroey and Anne Kari Kjellesvik contributed to the planing of the study, delivering the intervention and collecting data. Paal Friis, Kjetil Drangsholt, Finn Tore Gjestvang and Anders Wahlstedt contributed to the planning of the study. Svein Arild Nyrnes contributed to the analysis of the data.