
Abstract
Background
Reliable, large-scale, population-based data on blood pressure for Australian Aboriginal and Torres Strait Islander populations are limited. This present study aims to describe the blood pressure levels and to explore the clinical risk factors for hypertension among Australian Aboriginal and Torres Strait Islander peoples.
Design
A cross-sectional population survey was conducted in isolated communities in northern and central Australia. Methods Australian Aboriginal people (n = 1088) and Torres Strait Islanders (n = 606) aged 15 years and over were examined between 1993 and 1997. Blood pressure, body mass index, plasma glucose and urinary albumin-creatinine ratio were measured. The association of systolic, diastolic and pulse blood pressure to age was determined and independent associations of hypertension with other clinical variables were tested using logistic regression. Comparisons with results from other Australian data (including AusDiab) were made.
Results
Systolic blood pressure and pulse pressure increased in a linear manner with age but mean diastolic blood pressure leveled off at around 50 years and decreased thereafter, suggestive of arterial stiffening. The age-standardized prevalence of hypertension (blood pressure >140/90 mmHg or medication) for subjects aged 25–54 years was 27%, compared with 9% in non-Indigenous Australians in the Northern Territory and Queensland (AusDiab Survey). Older age, male sex, higher body mass index, albumin-creatinine ratio and diabetes were independently associated with hypertension.
Conclusions
Elevated blood pressure is a public health concern for indigenous people, which again highlights health differentials in Australia. Early detection and management of high blood pressure should be assigned a high priority in Indigenous communities. Eur J Cardiovasc Prev Rehabil 13:438–443 © 2006 The European Society of Cardiology
Keywords
Introduction
Hypertension is a well known modifiable risk factor for stroke, coronary heart disease (CHD), congestive heart failure and renal disease [1]. Antihypertensive therapy can reduce the risk of subsequent morbidity and mortality [2]. There is evidence that good blood pressure control is associated with a significant reduction in cardiovascular events [3]. The prevalence of hypertension (blood pressure ≥140/90mmHg or antihypertensive medication) among Australian adults (25 years and older) in the Australian Diabetes Obesity and Lifestyle Study of 2000 (AusDiab survey) was 31% for men and 27% for women [4]. There was also little change between 1980 and 2000 in the usage of antihypertensive medication and many hypertensive persons under treatment still had elevated blood pressure levels [4]. In the US, overall prevalence of hypertension was similar to that reported in AusDiab, but certain ethnic groups appear to experience excessive prevalence of hypertension [5]. Reliable, large-scale, population-based data on blood pressure for Australian Aboriginal and Torres Strait Islander populations are limited. Better definition of this important risk factor may lead to targeted and integrated primary health care strategies to combat the high burden of CHD.
The present study aims to describe the blood pressure levels and to explore the clinical risk factors for hypertension among Australian Aboriginal and Torres Strait Islander peoples.
Methods
Participants
Between 1993 and 1997, collaborative research programs saw 10 communities in Cape York, Torres Strait and Central Australia screened for diabetes and other cardiovascular risk factors. Many of these settlements were originally established by colonial authorities and include numerous language and tribal groups, whereas others are traditional homelands, and there is a range of histories of urbanization (from minimal to 130 years). While we recognize the wide diversity of ethnicities and nations represented in these surveys, and their different histories, we have analyzed these data collectively for reasons of statistical power, accuracy and generalizability. We have neither assumed nor sought ‘racial’ or genetic explanations for the health disparities reported here. Response proportion ranged from 40 to 86% of adult residents present at the time of survey. Communities included were those that chose to participate in health surveys and are therefore not a random sample of indigenous people in Australia generally or in the Northern Territory and Queensland. Anecdotal evidence suggests that for individuals within communities, participation was determined by social factors rather than by health status. The survey sample was representative of the national indigenous population with respect to age and sex distribution [6]. Ethnicity was determined by self-report. After excluding non-indigenous people, 1088 Aboriginal people and 606 Torres Strait Islanders aged 15 years and over were included in the present analysis. Further details of screening procedures have been reported elsewhere [7, 8].
The study was approved by Deakin University Ethics Committee, the Alice Springs Institutional Ethics Committee, the Ethics Committee of the Peninsula and Torres Strait Regional Health Authority and Cairns Base Hospital Institutional Ethics Committee and conducted in collaboration with indigenous community organizations.
Biochemical analyses
Plasma glucose and urinary albumin and creatinine were measured using standard laboratory techniques as previously reported [8]. Diabetes was defined as fasting plasma glucose >7.1 mmol/l or 2–h post-glucose load >11.1 mmol/l or antidiabetic medication [9]. According to the albumin-creatinine ratio (ACR), renal function was categorized into normal (ACR>3.4 mg/mmol); microalbuminuria (ACR 3.4–33.9 mg/mmol) and macroalbuminuria (ACR >34mg/mmol) [10].
Anthropometric measurements and blood pressure
Body weight was recorded to the nearest 0.1 kg and height to the nearest 0.1 cm. Sitting blood pressure was measured with the subjects seated at least 5 min prior to measurement using a Dinamap automated blood pressure monitor (Critikon, Tampa, Florida, USA). The mean of three consecutive readings was taken. Pulse pressure (PP) was calculated as systolic blood pressure (SBP) minus diastolic blood pressure (DBP). Hypertension was defined as SBP >140mmHg or DBP >90mmHg or current anti-hypertensive medication. For some analyses, blood pressure levels were classified according to the standard used by the European Society of Hypertension (ESH) as optimal (SBP >120 and DBP >80), normal (SBP 120–129 and DBP 80–84), high normal (SBP 130–139 or DBP 85–89), grade 1 hypertension (SBP 140–159 or DBP 90–99), grade 2 hypertension (SBP 160–179 or DBP 100–109) and grade 3 hypertension (SBP >180 or DBP >110) [11]. Self-reported antihypertensive medication usage was also recorded.
Statistical analysis
Data analysis was undertaken using the Statistical Package for Social Sciences (SPSS) version 11.5 (SPSS Inc, Chicago, Illinois, USA). Differences in mean levels of SBP, DBP and PP across categories of body mass index (BMI), renal function and diabetes were tested by analysis of variance using the general linear modeling function. Interaction of clinical categories with age, sex and ethnicity were tested but omitted if found to be nonsignificant. For comparison, we used data from participants in the age range 25–54 years [for which cardiovascular disease (CVD) mortality differentials are greatest] and from participants in this age range in the Northern Territory and Queensland arms of the AusDiab survey (which also used a Dinamp device for blood pressure measurement) [4]. Prevalence data were age-standardized using the 1996 Australian indigenous population as the reference population [6]. SBP, DBP and PP for participants in this study were also compared with Aboriginal people (n = 221) from central and northern Australia, who were screened between 1959 and 1963 and who had limited European contact [12]. The distribution of ESH blood pressure categories for men and women was compared using the X 2 test. Logistic regression analysis was conducted using hypertension as the dependent variable to identify independent predictor variables. Statistical significance was defined at the level of P >0.05 (two-tailed).
Results
Metabolic characteristics, blood pressure levels and hypertension prevalence
The sample of Aboriginal people was 1088; age range was 15–94 years (36 ± 16 years, mean ± SD). For Torres Strait Islanders, the sample size was 606, age range 15–87 years (37 ± 16 years, mean ± SD). There was no significant difference in mean SBP between Aboriginal people and Torres Strait Islanders (129 and 131 mmHg, respectively, P = 0.094). DBP for Aboriginal people was significantly greater than for Torres Strait Islanders (73 and 71 mmHg, respectively, P = 0.008) while the opposite was the case for PP (56 and 59mmHg, P >0.001). SBP, DBP and the prevalence of hypertension were significantly higher for men than for women (Table 1). Average BMI was significantly higher in women than in men. The crude prevalence of hypertension in the survey sample was 34% for men and 24% for women. For men in the age range 25–54 years, the age-standardized prevalence of systolic hypertension (SBP >140 mmHg) was 31% (compared with an age-standardized prevalence of 11% for the Northern Territory and Queensland arms of AusDiab, P >0.001), diastolic hypertension (DBP >90mmHg) was 14% (4% for AusDiab, P >0.001) and total hypertension was 43% (13% for AusDiab, P >0.001). For women in the age range 25–54 years, the age-standardized prevalence of systolic hypertension was 17% (compared with an age-standardized prevalence of 3% for the Northern Territory and Queensland arms of AusDiab, P >0.001), diastolic hypertension was 6% (4% for AusDiab, P = 0.256) and total hypertension was 20% (6% for AusDiab, P >0.001). For both indigenous men and women aged 25–54 years, the age-standardized prevalence of hypertension was 27%, compared with 9% in non-indigenous Australians (the Northern Territory and Queensland arms of AusDiab Survey, P >0.001).
There were significant linear associations of SBP, DBP and PP with increasing age for both the Aboriginal and Torres Strait Islander populations (Fig. 1). Whereas SBP continued to increase with increasing age, mean DBP leveled off at around 50 years and decreased thereafter. Consequently, PP started to increase sharply at around 50 years, particularly for men. An examination of historical data for Aboriginal people with little or no history of urbanization (Fig. 1) suggested that, while SBP increased consistently with age, the fall in DBP in older age groups may have been less marked or even absent. This was also the case for the National Heart Foundation Risk Factor Prevalence Survey [13] and in AusDiab (data not shown).
There were also significantly different frequency distribution of blood pressure levels between men and women (X 2 = 156, P >0.001; Fig. 2). The prevalence of hypertension including grade 1 to 3 hypertension defined by the ESH cut-off point was 33% for men and 21% for women (P >0.001), and the prevalence of grade 3 hypertension was around 2% for both men and women.
Of those with hypertension, one-quarter of men and women reported taking antihypertensive medication. Of those on medication, 32% had blood pressure below 140/90, and for diabetic people, 49% had blood pressure below 140/90. In the AusDiab survey of 2000, 41% of participants who were taking antihypertensive medication had blood pressure below 140/90mmHg [4].
Determinants of hypertension
The levels of SBP and DBP were significantly associated with increasing BMI and urinary ACR (Table 2). Diabetic participants had significantly higher blood pressure levels than non-diabetic participants (Table 2). In logistic regression analysis using hypertension as the dependent variable (Table 3), independent predictors were age (70% increase in odds per 10-year increment), male sex (fourfold), diabetes, microalbuminuria (all approximately twofold increase in odds of hypertension), macroalbuminuria (fourfold) and BMI (7% increase per kg/m2). There was a significant interaction of diabetes with sex, such that diabetes was associated with a greater odds ratio of having hypertension for women than for men. There were no other statistically significant interactions of sex or ethnicity with clinical variables.
Clinical characteristics of Aboriginal and Torres Strait Islander survey populations aged 15 years and over
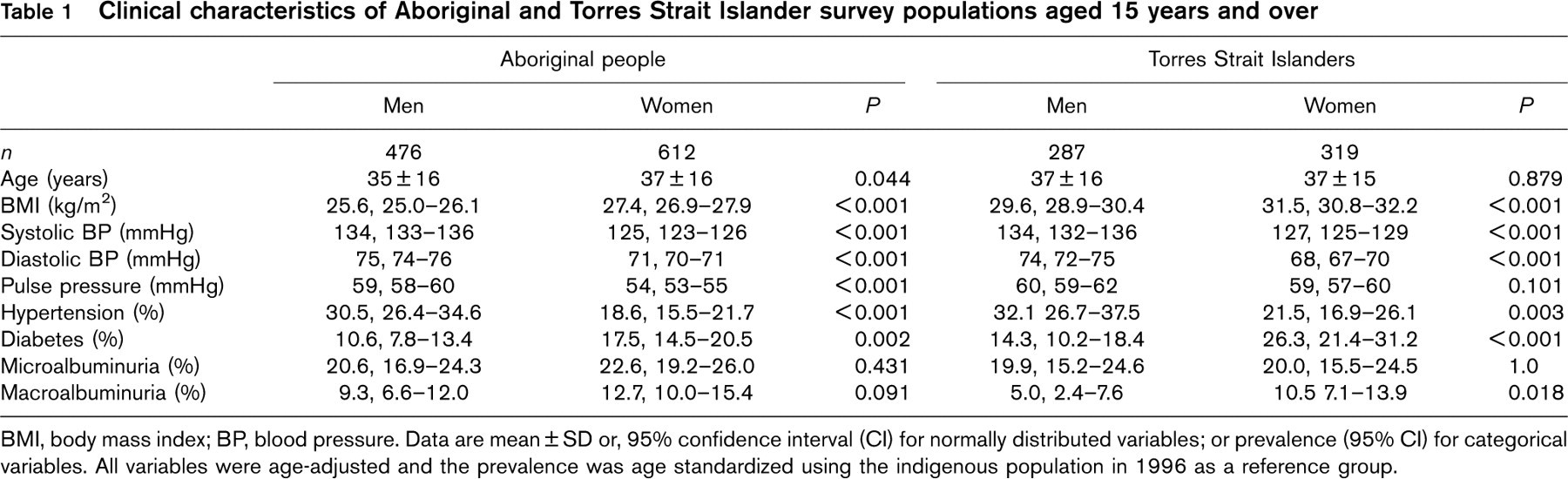
BMI, body mass index; BP, blood pressure. Data are mean ± SD or, 95% confidence interval (CI) for normally distributed variables; or prevalence (95% CI) for categorical variables. All variables were age-adjusted and the prevalence was age standardized using the indigenous population in 1996 as a reference group.
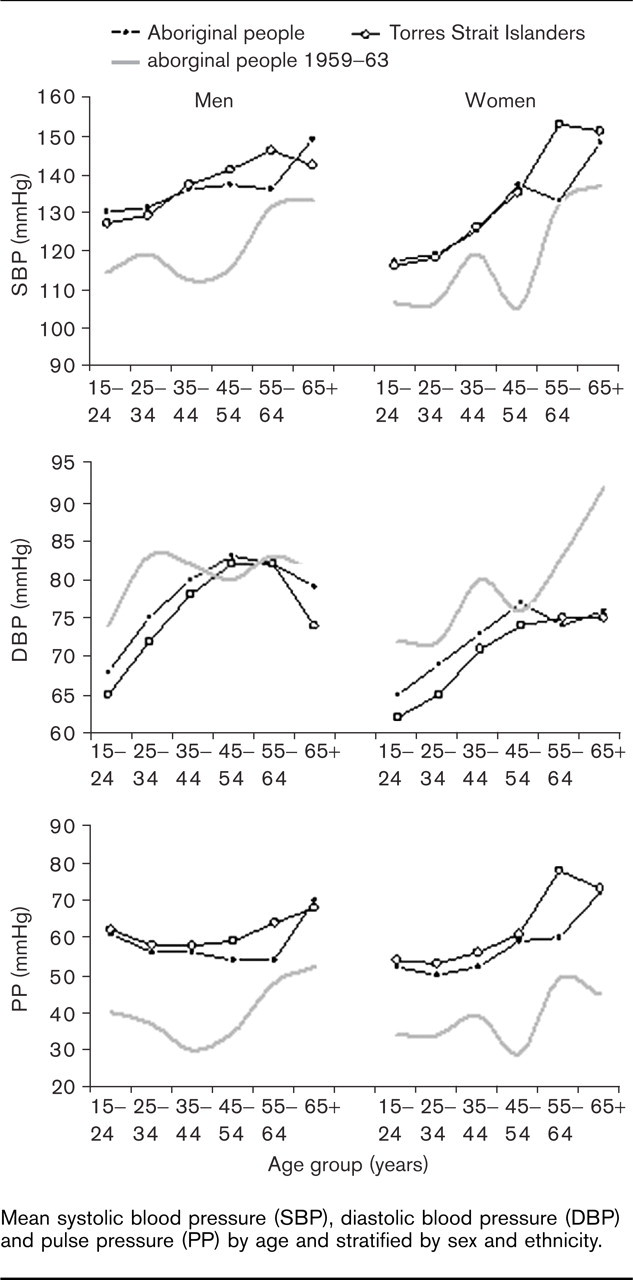
Mean systolic blood pressure (SBP), diastolic blood pressure (DBP) and pulse pressure (PP) by age and stratified by sex and ethnicity.
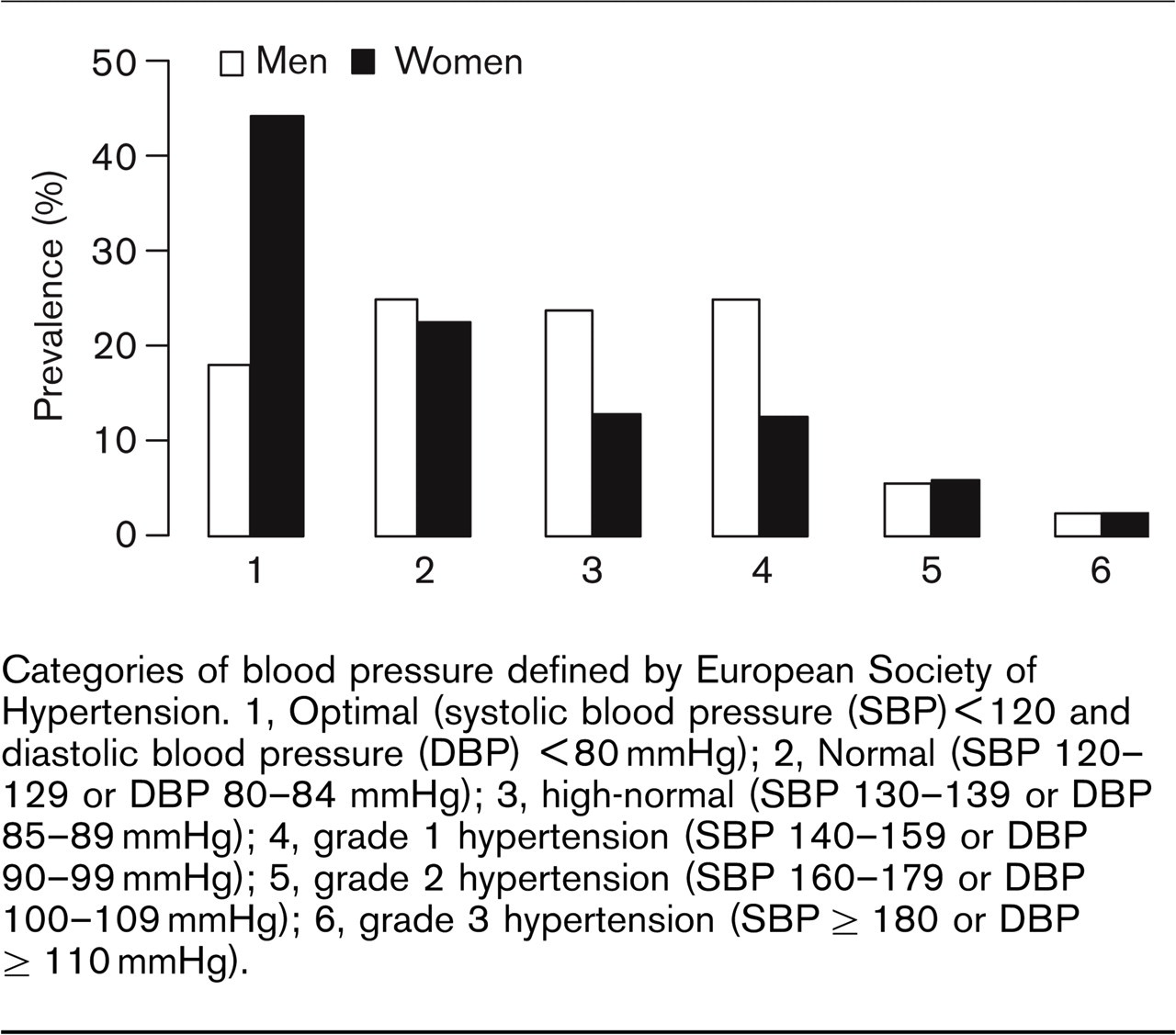
Categories of blood pressure defined by European Society of Hypertension. 1, Optimal (systolic blood pressure (SBP) >120 and diastolic blood pressure (DBP) >80mmHg); 2, Normal (SBP 120–129 or DBP 80–84 mmHg); 3, high-normal (SBP 130–139 or DBP 85–89 mmHg); 4, grade 1 hypertension (SBP 140–159 or DBP 90–99mmHg); 5, grade 2 hypertension (SBP 160–179 or DBP 100–109mmHg); 6, grade 3 hypertension (SBP >180 or DBP >110mmHg).
Discussion
This study indicates that elevated blood pressure is highly prevalent and therefore probably an important mediator of the high risk of cardiovascular mortality for Aboriginal and Torres Strait Islander people in Australia. The mean SBP was higher for men than for women, and it increased with age especially for women. DBP also increased with age up to 50 years, and decreased thereafter suggestive of large arterial stiffening (see below). The prevalence of hypertension was very high in the age range 25–54 years compared with Northern Territory and Queensland participants in AusDiab, although we observed no significant difference in prevalence of diastolic hypertension for indigenous and non-indigenous women in this age range.
The little available data suggest that blood pressure of Aboriginal people prior to the rapid urbanization that has occurred in the last few decades was lower [12, 13]. Compared with the indigenous people in the present study, the mean SBP in the Aboriginal people living with limited European contact between 1959 and 1963 [12] was apparently lower, particularly in the younger age groups, and DBP appeared similar and PP substantially lower than observed in the more contemporary data although methodological differences (use of Dinamap versus mercury sphygmomanometer) probably contribute to the apparently low DBP in the present survey (Fig. 1). Previous studies also indicated that blood pressure increased to a higher level among Aboriginal people living in semi-urban areas and was higher than that of non-Aboriginal Australians [14, 15]. Regarding generalizability of these results, the survey sample was highly representative of the adult populations of the participating communities, and of the national Aboriginal and Torres Strait Islander populations identified in the census with respect to age and sex [6]. While we should be cautious in generalizing our conclusions beyond central and northern Australia, we note the diversity of communities represented and the results observed are therefore likely to be typical of other communities in those regions. Other reports have found that prevalence of hypertension (BP >140/90 mmHg) in Aboriginal people was 27–29% for a Top End (Northern Territory) community and urban Aboriginal people in Perth respectively [15, 16], after age-standardization to the 1996 indigenous population [6]. These results were similar to our findings. Data for Aboriginal populations in the Kimberley in the 1980s found a somewhat higher prevalence of diastolic hypertension (DBP >95mmHg) (13% compared with our figure of 3%) after age-standardization [17] for reasons which are not clear.
Blood pressure by clinical categories
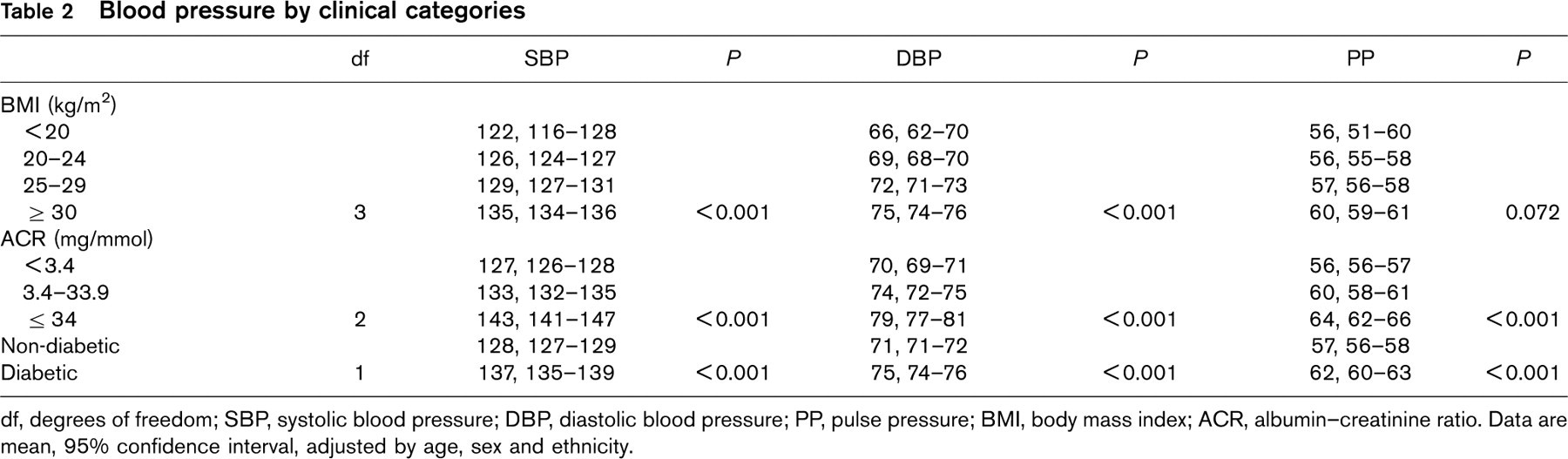
df, degrees of freedom; SBP, systolic blood pressure; DBP, diastolic blood pressure; PP, pulse pressure; BMI, body mass index; ACR, albumin-creatinine ratio. Data are mean, 95% confidence interval, adjusted by age, sex and ethnicity.
Logistic regression analysis of hypertension
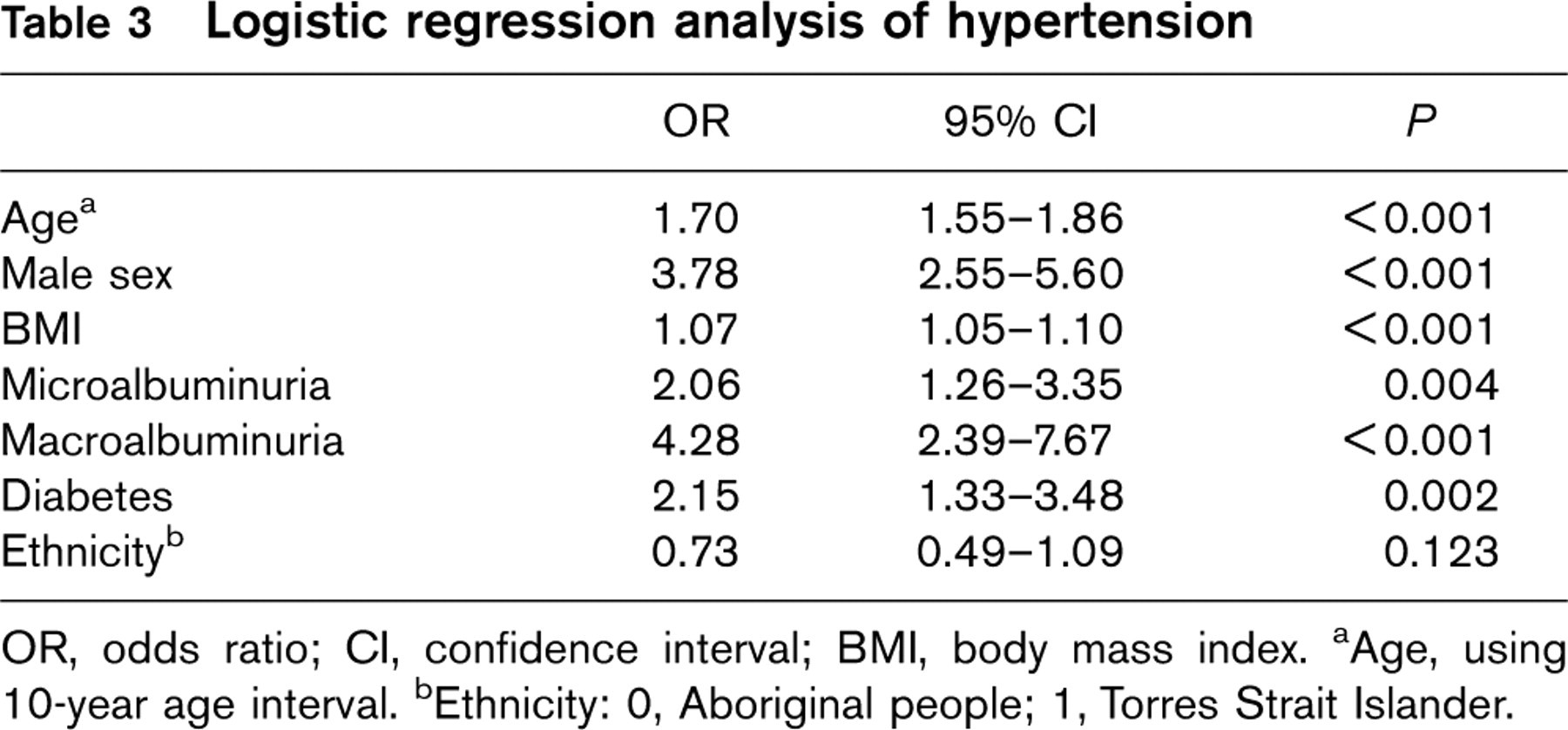
OR, odds ratio; CI, confidence interval; BMI, body mass index. aAge, using 10-year age interval. bEthnicity: 0, Aboriginal people; 1, Torres Strait Islander.
In the present cross-sectional study, independent predictors of hypertension were older age, male sex, diabetes, BMI and renal function while a previous study identified BMI and alcohol consumption (especially among younger people) as contributors to elevated SBP and DBP. In general, our findings regarding determinants of blood pressure were consistent with studies in other populations [2, 4].
Previous work has indicated that SBP, DBP and PP all predict CHD risk [18]. It is well established that SBP increases with age, while DBP plateaus [19] and may even fall with age [20], leading to increased PP and this pattern was also observed here. Elevated PP may be a surrogate measure of large arterial stiffness, particularly in the aorta [21], and in older populations is more predictive of CVD risk than are DBP or SBP [20]. Whether this increased risk relates to hypertension itself or specifically to arterial stiffening is slightly controversial but an increasing number of studies suggest that arterial stiffening is an independent predictor of CHD mortality [22]. For Aboriginal and Torres Strait Islander participants in this study, mean DBP decreased after age 45–54 years: in the Risk Factor Prevalence Survey this phenomenon occurred later for men and not at all for women [19]. Thus, the data are consistent with the concept that central arterial stiffening may be occurring at a relatively younger age in indigenous populations, and the apparently normal DBP levels are not necessarily benign. Whether this is associated prospectively with risk is not known but would be reasonably expected based on studies in other populations.
Previous studies indicated that lowering BP in patients with diabetes and hypertension is associated with decreases in cardiovascular events and renal failure [23]. Only 25% of hypertensive indigenous people reported taking antihypertensive medication in the present study, although under-reporting of medication usages is possible. For those on medication, only one-third had adequate blood pressure control (blood pressure >140/90 mmHg). Of the diabetic participants, 49% had blood pressure below 140/90mmHg, hence improving blood pressure control in diabetes should be a goal of therapy. Hoy et al. [23] reported that treatment of all high-risk people with angiotensin-converting enzyme inhibitors markedly reduced mortality and renal failure in an Aboriginal community. Sustaining such intensive clinical interventions, however, remains a challenge. We note that the data presented are now up to 10 years old. Current management of hypertension in regions from which the present survey sample was recruited is substantially better, with most diabetic patients with hypertension being prescribed appropriate medication and 62–70% achieving ‘good’ blood pressure control [24]. Anecdotal evidence suggests improvements occurred partly as a result of the collaborative nature of the screening programs described here raising awareness of the value of early detection. More current data are required to show whether these subsequent clinical and other interventions are having a beneficial effect across the population of these communities (albeit in face of the broader social and political determinants of CVD risk). Although the type of intensive surveys from which the present data were derived are probably less feasible today, progress in primary healthcare-based screening, recall, and data collection systems should allow such information to be more available. Despite the availability of electronic systems designed for this purpose, however, the chronic under-resourcing of Aboriginal medical services and the necessity for their staff to give priority to acute medical care often prevents optimal use of such systems and data for population monitoring and prevention activities.
In conclusion, the blood pressure of indigenous people was apparently higher than for non-indigenous Australian people. Blood pressure increased with age and was suggestive of arterial stiffening at a relative young age in indigenous people. Older age, male sex, higher BMI, diabetes and ACR were independently associated with hypertension. The detection, control and treatment of high blood pressure and its associated risk factors and community-level risk conditions should be assigned a high priority in Australian indigenous communities in order to reduce the excessive rates of cardiovascular disease. Effective primary healthcare is required for primary prevention, early detection and management of high blood pressure to bridge the gap between indigenous and non-indigenous Australians.
Footnotes
Acknowledgements
The authors thank Phillip Mills, the many people who assisted with fieldwork, and the councils, health services and residents of the participating communities. We thank the AusDiab steering committee for providing access to the AusDiab data.