
Abstract
Background
Presently, complementary and alternative medicine, including both therapies and herbal/oral supplements, is used globally. Few studies have examined the use of specific therapies, separate from herbal/oral supplements, in cardiac rehabilitation. This paper presents a systematic evaluation of current research evidence related to use of specific complementary and alternative medicine therapies in secondary prevention of cardiovascular disease, with a view to making recommendations for cardiac rehabilitation.
Design and methods
A literature search was conducted using complementary and alternative medicine websites, Medline, Allied and Complementary Medicine, CINAHL, Cochrane databases, EMBASE, SportDiscus, Clinical Evidence, and Evidence-Based Practice to locate research-based scientific evidence related to the use of complementary and alternative medicine in cardiac rehabilitation. Search keywords included heart, cardiac, cardiovascular, coronary, myocardial and rehabilitation, combined with particular therapies. Herbal/oral supplements were not included in this evaluation.
Results
Some complementary and alternative medicine therapies may be useful to patients by themselves or coupled with traditional cardiac rehabilitation. Tai chi, as a complement to existing exercise interventions, can be utilized for low and intermediate risk patients. transcendental meditation may be used as a stress reduction technique. There was insufficient evidence found for the use of acupuncture or chelation therapy in cardiac rehabilitation or secondary prevention.
Conclusions
Some complementary and alternative medicine therapies hold promise for patients in cardiac rehabilitation. Further research is essential, however, in all areas of complementary and alternative medicine to confirm its usefulness as an adjunct to cardiac rehabilitation.
Keywords
Introduction
The study of complementary and alternative medicine (CAM) and its relationship to more accepted forms of medical practice is the subject of increased focus in both research and practice, even though there continues to be a lack of consensus about the definition of CAM. There are no reliable and valid measures of CAM use (or likelihood to use), and researchers struggle with appropriate methodologies for testing the effectiveness of CAM, particularly in patient populations with complex illnesses involving multiple treatment modalities, such as those with cardiovascular disease.
Given the lack of agreement about a precise definition of CAM, the definition employed in this paper needs to be clearly described. For our purposes, CAM is defined as a broad spectrum of therapies and natural products perceived as different from those that would normally be prescribed by Western medical practitioners. CAM is a non-traditional, holistic approach used to complement allopathic care. Allopathic care is defined as a method of treating disease with remedies that produce effects antagonistic to those caused by the disease itself. Typically, allopathic treatment focuses on symptom or sickness-driven approaches to care.
The National Center for Complementary and Alternative Medicine (NCCAM), a center within the National Institutes of Health, acknowledges a group of diverse medical and healthcare systems, practices and products, which are not part of Western medicine and are used as complementary/alternative approaches to health. Alternative medical systems have unique theories and practices, which evolved prior to the Western healthcare system. Homeopathy, naturopathy, traditional Chinese medicine and ayurveda are examples of alternative medical systems.
Tataryn and Verhoef [1] proposed a framework that classifies both conventional and CAM healthcare practices according to basic assumptions regarding the nature of health and disease. According to the framework, there are four basic paradigms: body, body–mind, body–energy and body–spirit. The body paradigm acknowledges biological mechanisms as the primary agents of health and disease. The body–mind paradigm extends the body paradigm to include factors such as stress and social support as influencing health and disease. Therapies in the body–energy paradigm are based on the flow and balance of life energies. Finally, the body–spirit assumes that one or more transcendental aspects or personalities existing outside the limitations of the material universe can influence health and disease, for example faith healing.
The words complementary and alternative are used to distinguish the current relationship that may exist between two different paradigms of thought regarding approaches to healthcare. Simplified, conventional Western medical practice is grounded in a biological or body model, concentrating on diagnosis and treatment of disease. On the other hand, CAM is founded on the belief that biological phenomena are explained through the existence of a vital life force. Health issues are created when the flow of vital energy is blocked resulting in disruptions on any level whether it is physical, mental, emotional or spiritual. Harmony between body, mind and spirit is essential for health. A complementary approach uses a non-traditional holistic approach to complement Western medical care; whereas alternative care is the sole use of non-allopathic treatments for a healthcare condition. Interestingly, this term is slowly being replaced by the emerging term ‘integrative medicine', which includes a combination of practices based on biological determinants of health, as well as those founded in alternative beliefs about what determines health and disease.
In this evaluation of the literature, we have purposefully separated the herbal/oral supplements component of CAM from CAM therapeutic practices. Use of herbal/oral supplements, while typically considered part of a broad definition of CAM, are increasingly utilized by consumers as remedies for treating health conditions and thus, using them in this fashion approximates a more traditional, allopathic approach to health. While there is an increasing body of literature related to herbal/oral supplements, there has been less focus on specific CAM practices and their utility in particular patient populations. In order to hone the focus of this review we have chosen to limit it to CAM practices. Given the definition of CAM that we have adopted, therapies such as massage, relaxation and other conventional stress management techniques were not included, primarily because they are considered within the realm of mainstream Western medicine (e.g. massage therapy is prescribed by physicians and often covered by health insurance plans).
Literature review
In the past decade there has been a rise in the use of CAM, as defined in the broadest sense, especially in countries where it has not previously been part of the formal health care system. Ernst [2] published a systematic review of studies examining the prevalence of use of all forms of CAM in various countries. Though actual prevalence of use was difficult to determine, he concluded that the popularity of CAM was increasing, and that a common demographic profile of users was emerging. Since then, several studies have confirmed the global and increasing use of CAM, especially in the adult population.
Eisenberg [3] reported that the prevalence of all-CAM use (i.e. herbal/oral supplements and therapies/practices) was approximately 42% in the United States in 1997. Harris and Rees [4], in a systematic review on the prevalence of all-CAM use in the general population, confirmed the prevalence figures reported by Eisenberg. Recently, Hanssen et al. [5] described the prevalence of all-CAM use in Norway, Denmark and Stockholm County and reported prevalence rates ranging from 34% in Norway, to 45% in Denmark and 49% in Stockholm. Al-Windi [6] explored CAM use, and its determinants, in a multi-ethnic Swedish primary healthcare practice population. Findings revealed that 17% of respondents (n = 1433) had consulted a CAM provider in the previous year and many had consulted several types of CAM providers. Data related to the prevalence of CAM use among patients in cardiac rehabilitation have not been described, though three issues might lead us to speculate that a significant number of cardiac rehabilitation patients are using CAM. First, the widespread popularity of CAM among healthcare consumers may be at least partially extended to cardiac rehabilitation patients; second, it is well documented that consumers view most CAM treatments as very low risk and potentially of benefit; and third, users of CAM may be reluctant to fully inform their healthcare providers about CAM use.
Evidence is slowly beginning to emerge related to the effectiveness of CAM in particular patient populations, but the appropriate research design for studies of effectiveness is a randomized controlled trial and, to date, few such studies have been reported. A particularly important patient population to assess in terms of the potential role for CAM is those with cardiovascular disease. In spite of this, the current state of the scientific literature related to CAM therapeutic practices in cardiac rehabilitation precludes a meta-analysis. The vast majority of the published research in this area is observational. Where controlled trials exist, they have been done in related cardiovascular patient populations (e.g. heart failure) but not specifically in the context of cardiac rehabilitation programs.
Therefore, the purposes of this systematic evaluation were to search for research evidence related to use of CAM therapies in cardiac rehabilitation, further, if evidence related specifically to cardiac rehabilitation was unavailable, to extrapolate from evidence related to CAM therapies in general cardiovascular patient populations, and finally to evaluate the level of current evidence.
Methods
This review focused on CAM therapies that are not currently incorporated into traditional cardiac rehabilitation programs and identifying best evidence for cardiac rehabilitation practitioners. We conducted a search of traditional databases and CAM websites, including Medline, Allied and Complementary Medicine, CINAHL, Cochrane databases (Database of Abstracts of Reviews of Effects, Central Register of Controlled Trials, Database of Systematic Reviews), EMBASE, SportDiscus, Clinical Evidence, and Evidence-Based Practice to locate research-based scientific evidence related to the use of CAM therapeutic practices in cardiac rehabilitation. The key search words were heart, cardiac, cardiovascular, coronary, myocardial and rehabilitation, which were combined with particular CAM therapies. Other search words were systematic review, meta-analysis, randomized controlled trial and review. Several CAM-related websites were also used for additional information: The National Center for Complementary and Alternative Medicine (www.nccam.nih.gov); the Alternative Medicine Foundation (www.amfoundation.org); the American Board of Clinical Medical Toxicology-Chelation (www.abct.info); and Registered Nurses’ Association of Ontario (www.rnao.org). A large amount of CAM literature is published in foreign languages and has not been included here.
Rating scale for grading evidence-based recommendations
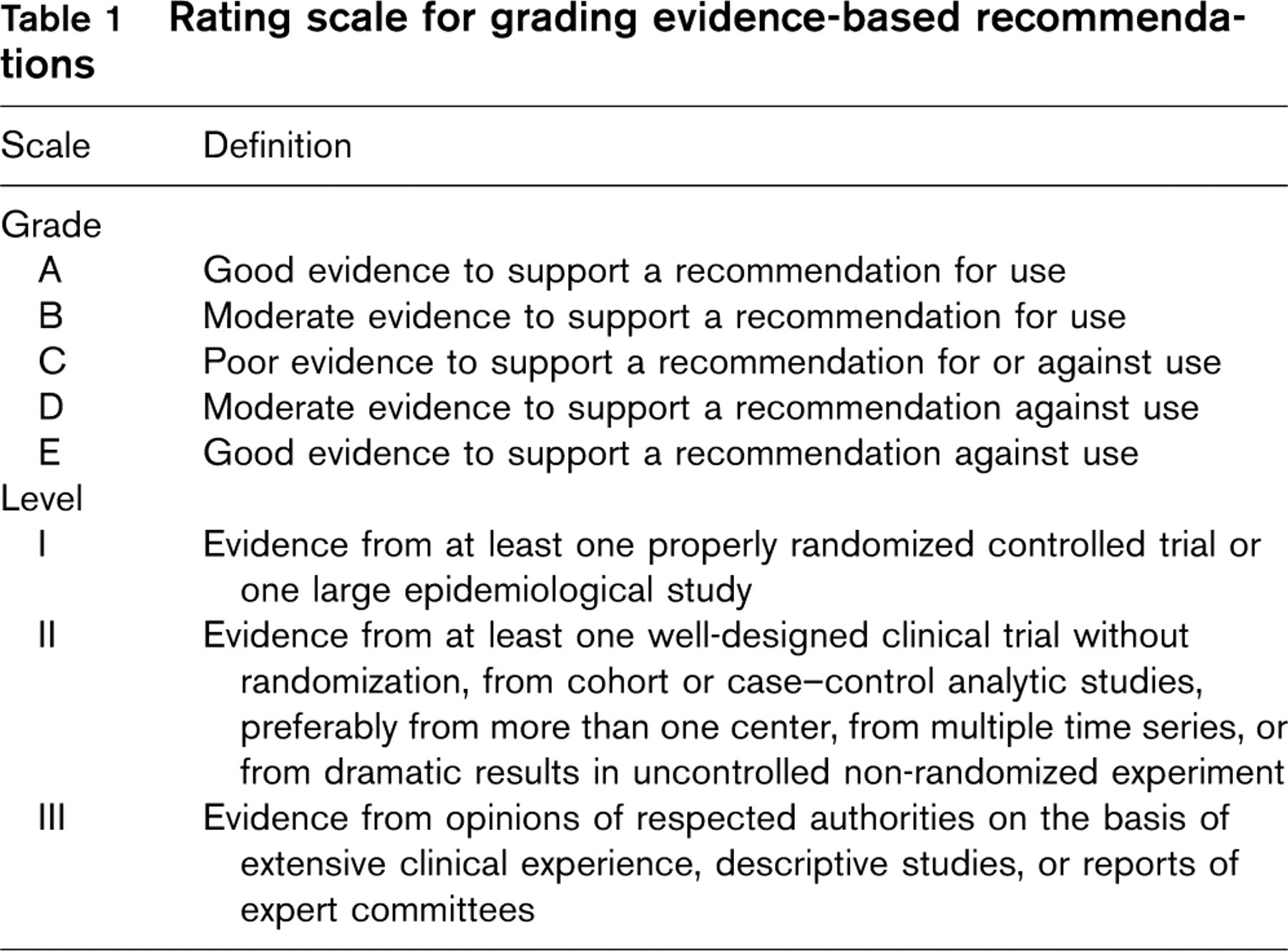
Only those studies reporting the most rigorous methodology and having potential value in cardiac rehabilitation were selected for review. Observational, descriptive, cross-sectional or case studies were not included. Individual articles that were included in review papers were not re-assessed as separate studies; only the review paper is cited here. In order to capture most recent evidence, the time parameters on this search were from September 1999 to July 2004. The very few controlled trials that were conducted prior to 1999 are included in review papers published between 1999 and 2004.
Studies were included based on the following criteria: the therapy was examined in a cardiac rehabilitation population; if direct cardiac rehabilitation evidence was not available, the therapy was examined vis-à-vis an established coronary artery disease risk factor (e.g. hypertension); and the study was conducted according to clearly described methods. There are additional CAM therapies to those presented in this paper. Most were excluded, however, on the basis of the criteria mentioned above; primarily weaknesses in design, sample size or other methodological issues. The evidence reviewed here has been rated according to the criteria outlined in Table 1.
Results
Tai chi
Tai chi, a form of qigong (pronounced chee-gung) is an ancient Chinese practice that includes different techniques, such as medication, postures, exercises and breathing, designed to restore energy and promote health. Tai chi is commonly practiced in North American society and is best known for its benefits with older adults [7–9]. In the Chinese practice of medicine, qi is viewed as life energy present in the world and in the body. Imbalances in the physical, mental and emotional states of the individual will disturb the qi in different parts of the body Tai chi uses various forms of exercise, called movements, which function to guide breathing and circulation as a means of directing vital energy through the body. It is the slow continuous rhythm of each posture that is believed to improve circulation, breathing, and strengthen internal organs. The energy cost of movements associated with tai chi has been reported to range from 1.5 to 2.6 metabolic equivalents in healthy adults [10]. Tai chi has been successfully used to treat hypertension, stress, depression, mental strain, chronic indigestion, insomnia and arthritis [9].
No studies were located that examined tai chi within the specific context of cardiac rehabilitation programs or compared tai chi to either exercise-based or comprehensive cardiac rehabilitation in a controlled manner. Lan et al. [11] evaluated the training effect of a 1-year tai chi program in 20 men who had undergone coronary artery by-pass graft (CABG) surgery and had completed a phase II cardiac rehabilitation program. Nine men practiced tai chi in a supervised setting an average of 3.8 (SD 1.5) times per week for 1 year. The comparison group of 11 men were given a home-based exercise prescription at similar intensity (48–57% heart rate range). Mean frequency of exercise in the control group was 1.7 (SD 1.1) times per week. Graded exercise tests were performed before and after 1 year of training. After 1 year, peak V o 2 increased by 10.3% (P < 0.01) whereas the control group showed a non-significant decrease. Limitations related to methods, sample size and exercise frequency make it difficult to comment upon the effect of tai chi compared with other typically recommended exercise prescriptions in cardiac rehabilitation. The within-group improvement in the tai chi group, however, suggests possible benefits of this form of exercise in patients after CABG surgery.
Channer et al. [12] studied the effects of tai chi, aerobic exercise or a non-exercise support group on blood pressure in 126 patients (all male) following an acute myocardial infarction. Patients who were capable of exercising and not diagnosed with severe arthritis, overt heart failure or limiting angina were randomly assigned to one of the three groups. Patients attended twice weekly for 3 weeks, then weekly for a further 5 weeks. Over the 11 sessions of exercise there was a negative trend in diastolic blood pressure in the tai chi group only (Rs = 0.79; P < 0.01). Significant downward trends in systolic blood pressure occurred in both exercise groups (Rs values 0.64 and 0.63, both P < 0.05). The clinically important finding from this study is the apparent equivalent effect of tai chi to aerobic exercise on blood pressure in post-myocardial infarction patients, suggesting that tai chi may be either an alternative or an adjunct to aerobic exercise within cardiac rehabilitation programs, depending on patient preference.
Recently, Yeh et al. [13] conducted a randomized controlled trial to examine the effects of a 12-week tai chi program on quality of life and exercise capacity in a small sample (n = 30) of patients with chronic stable heart failure. Patients were randomly assigned to receive either 12 weeks of tai chi training or usual care (which included general advice about medications, diet and exercise but did not include a formal, supervised exercise protocol). Tai chi classes were held twice a week for 12 weeks. Quality of life was assessed using the Minnesota Living with Heart Failure Questionnaire [14] and exercise capacity was assessed using both the 6-min walk test and a symptom-limited bicycle exercise test. After 12 weeks of training, there was a statistically significant between-group difference (P = 0.001) in quality of life scores and distance walked in favor of the tai chi group. There were no significant differences in peak oxygen uptake and no adverse outcomes. Compared with usual care (which did not include cardiac rehabilitation), the findings of this study suggest that tai chi may be a beneficial adjunct to cardiac rehabilitation for patients with chronic stable heart failure.
Acupuncture
Acupuncture, like tai chi, is part of a holistic system of traditional Chinese medicine (TCM), which views health as the flow of energy. TCM states that there are acupuncture points on the human body connected to meridians, which conduct energy or qi throughout the body and correspond to specific organs. The acupuncture points are where the meridians come closest to the skin surface. In order to understand acupuncture fully, however, the concept of yin and yang must also be considered. The concept of yin and yang is based on natural law, one of the foundational theories of TCM. According to the foundational theories of TCM, energy fields, known as yin and yang, are antagonistic but balancing interdependent forces in natural phenomena. Qi flows freely through the meridians when these forces are balanced. A balanced yin and yang and flow of qi maintain the body in a healthy state. Acupuncture is believed to restore balance to yin and yang and to keep the normal flow of energy unblocked [15].
Acupuncture is one of the TCM practices that has captured the attention of Western medical practitioners despite their inability to explain how it works. Studies have shown, however, that acupuncture can cause biological responses, such as the conduction of electromagnetic signals, activation of the opioid systems, changes in brain chemistry and blood flow regulation [16].
The effect of acupuncture on angina pectoris and other related cardiac disorders has not been studied rigorously with controlled trials, and those who have attempted to use these designs have had difficulties with methodological issues. Researchers have found conflicting results as to the effectiveness of this therapy in relieving symptoms and improving functional capacity of patients with angina pectoris [17–20]. The true value of this technique is yet to be determined. In 1997, The National Institutes of Health Consensus Panel [16] released the following statement describing the potential benefits of acupuncture and highlighting the methodological issues.
While there have been many studies of its potential usefulness, many of these studies provide equivocal results because of design, sample size, and other factors. The issue is further complicated by inherent difficulties in the use of appropriate controls, such as placebos and sham acupuncture groups. However, promising results have emerged, for example, showing efficacy of acupuncture in adult postoperative and chemotherapy nausea and vomiting and in postoperative dental pain. There are other situations such as addiction, stroke rehabilitation, headache, menstrual cramps, tennis elbow, fibromyalgia, myofascial pain, osteoarthritis, low back pain, carpal tunnel syndrome, and asthma, in which acupuncture may be useful as an adjunct treatment or an acceptable alternative or be included in a comprehensive management program. Further research is likely to uncover additional areas where acupuncture interventions will be useful. (p. 1)
Although generalization of this statement to the cardiac patient is impossible, the promising results in many other areas of healthcare point to the clear need for research in cardiac rehabilitation before any conclusion can be drawn.
Transcendental meditation
Transcendental meditation was founded by the Maharishi Mahesh Yogi in 1957, and has been taught to millions of people throughout the world. In 1980, Maharishi introduced Maharishi Ayur-Veda, a comprehensive revival of the world's most ancient system of healthcare. Maharishi's Vedic Approach to Health is a holistic, prevention-oriented natural system of healthcare that includes transcendental meditation and Maharishi Ayur-Veda [21]. Transcendental meditation is a simple technique, which is practiced for 15–20 min twice daily. It is initially learned from qualified teachers in a seven-step course. Transcendental meditation allows the mind to settle while alertness is maintained. The result is generally calmer and clearer thinking.
The technique should not be considered synonymous with stress management as it is currently understood and utilized in cardiac rehabilitation. A ‘relaxation response’ can be attained by means of any number of relaxation and meditation techniques. Research suggests, however, that each technique has differing effects on body and mind [22]. Each approach should be considered on its merits and therefore transcendental meditation should be considered a distinct modality, separate from other stress management techniques that are often used (and have been studied) in cardiac rehabilitation.
A review of the literature on transcendental meditation was recently published by the Royal Australian College of General Practitioners [21] that outlined the diverse physiological, psychological and behavioral findings of transcendental meditation. Since this review incorporates the individual studies related to transcendental meditation in cardiac patients, only the findings of the review are reported here. Some of the physiological findings, which would be of interest in cardiac rehabilitation, included decreased blood pressure and cholesterol, lower baseline levels of respiration, heart rate and plasma lactate, a reversal of the effects of stress on neuroendocrine functioning and decreased sympathetic activation. Psychological and behavioral responses identified in the review [21], which may be important for recovery and the sustained well-being of cardiac patients included decreased anxiety, post-traumatic stress disorder, and depression; improved self-concept; and decreased use of tobacco, alcohol and illicit drugs. Based on these responses, it was concluded that transcendental meditation showed promise for both prevention and treatment of patients with coronary artery disease. Two other independent reviews of randomized, controlled trials and meta-analyses have supported this finding and further concluded that transcendental meditation is an efficacious and cost-effective, specialized stress reduction strategy that could also reduce cardiovascular disease risk factors [23,24]. Further research is required to identify the mechanisms involved and verify preliminary findings concerning a reduction of atherosclerosis [25]
Chelation
Chelation therapy has received considerable attention as a treatment for heavy metal poisoning and vascular diseases. It involves the use of repeated intravenous administration of ethylenediamine tetra-acetic acid (EDTA), usually in combination with vitamins, trace elements and iron supplements. It binds to metallic ions in the body and removes them through urinary excretion, and in the process it redistributes many metals within the body. Some supporters of the therapy believe that it may alter plaque morphology or improve endothelial function. There is no evidence, however, to support this claim. In four randomized, controlled trials and two systematic reviews, researchers reported insufficient evidence to support the use of chelation with coronary artery and peripheral vascular disease [26–31]. In the Program to Assess Treatment Strategies to Achieve Cardiac Health (PATCH) trial, more than 80 patients with documented, angiographically significant coronary artery disease, but minimal angina, were randomized to standard full-length chelation therapy versus placebo. After 1 year, there were no significant differences in treadmill walking time to angina or 1 mm of ST depression and no differences in endothelial function as measured by forearm blood flow vasodilatation. [26,27].
The Trial to Assess Chelation Therapy (TACT) may finally answer questions regarding the true clinical efficacy of chelation therapy. This is a study sponsored by the National Heart Lung and Blood Institute that will randomize, in a double-blind fashion, more than 2500 patients with a documented history of myocardial infarction to either standard chelation therapy or placebo. The primary endpoint of this trial is a composite clinical endpoint that includes all cause mortality, myocardial infarction, stroke, coronary revascularization, and hospitalization for angina. Patients will be followed for up to 4 years after chelation therapy. Patient recruitment is still underway and results are not expected until after 2008.
Discussion
Cardiac rehabilitation programs are designed to assist patients with various cardiovascular diagnoses, improve their symptom status and increase their functional capacity. Most importantly, cardiac rehabilitation programs have been shown to reduce mortality in persons with documented coronary artery disease and to improve the control of cardiovascular risk factors such as cholesterol levels and systemic hypertension [32]. Creative and innovative approaches to maintain health in vulnerable cardiac states are necessary in this specialty. Some CAM practices hold promise for providing unique forms of therapies that have physiological and psychological benefits without necessarily requiring vigorous physical activity, a desired outcome with patients in vulnerable cardiac states. The limited availability of high-quality scientific evidence, however, makes a statement of efficacy impossible for many of the therapies at this time, but also reinforces the importance of further research.
On the basis of this review the following conclusions are offered (see Table 1 for definitions of grades and levels): There is preliminary evidence to suggest that tai chi and modified forms of it could be an adjunct to existing exercise interventions in cardiac rehabilitation programs for low and intermediate risk patients (grade B, level II). There is insufficient information for the use of acupuncture in cardiac rehabilitation until further research is conducted (grade C, level 1). There is evidence for cardiac rehabilitation professionals to consider transcendental meditation as a unique stress reduction technique for selected patients. For severely compromised patients, more research is required (grade B, level 1). There is no evidence to support the use of chelation therapy for the treatment of vascular disease. Furthermore, the therapy may cause severe adverse effects (grade E, level 1).
This review reveals important trends and consistencies in the data and clarifies the totality of the evidence to date. Until studies with stronger research designs are conducted, this review tells us that there are emerging patterns in the potential usefulness of certain CAM practices within traditional cardiac rehabilitation programs.