
Abstract
Background
The purpose of this study was to describe the associations between different levels of long-term physical activity in leisure time and subsequent causes of deaths.
Design
The Copenhagen City Heart Study is a prospective cardiovascular population study of 19 329 men and women aged 20–93 in 1976. Physical activity in leisure time was estimated at the examinations in 1976–78 and 1981–83. This analysis consists of 2136 healthy men and 2758 women aged 20–79 years, with unchanged physical activity at the two examinations, and with all covariates included in the multivariate analyses: smoking, total-cholesterol, high-density lipoprotein-cholesterol, systolic blood pressure, diabetes mellitus, alcohol consumption, body mass index, education, income, and forced expiratory volume in 10.78 (% predicted).
Results
Adjusted relative risks (95% confidence interval) for coronary heart disease were, for moderate physical activity 0.71 (0.51, 0.99) and for high 0.56 (0.38, 0.82). For cancer, moderate activity 0.77 (0.61, 0.97) and high activity 0.73 (0.56, 0.95) and for all-cause mortality, moderate 0.78 (0.68, 0.89) and high 0.75 (0.64, 0.87) for both sexes combined. Using Kaplan—Meier plots we calculated gained years of expected lifetime from age 50. Men with high physical activity survived 6.8 years longer, and men with moderate physical activity 4.9 years longer than sedentary men. For women the figures were 6.4 and 5.5 years, respectively.
Conclusion
Long-term moderate or high physical activity was in both sexes associated with significantly lower mortality from coronary heart disease, cancer and all-causes. The same tendency was found for stroke and respiratory diseases, but the associations did not reach statistical significance. Eur J Cardiovasc Prev Rehabil 13:173–179 © 2006 The European Society of Cardiology
Introduction
In 1953, the first report describing a significant inverse relation between occupational physical activity and coronary heart disease was released by Morris et al. [1]. Since then several investigators have confirmed this finding [2–7], while others did not found such a relationship [8, 9]. Other studies have examined the relation between leisure-time physical activity and coronary heart disease (CHD) [5, 10–16]. In general, the evidence points to a benefit of regular, moderate physical exercise.
The association between physical activity and stroke was described 35 years ago in a report from the Harvard Alumni Health Study [17]: alumni who had been athletes in college experienced less than half the risk of fatal stroke compared with non-athletes. After adjustments for confounders, physical activity continued to be inversely related to the incidence of stroke [18]. Similar associations have been observed in some other populations [16, 19], but not all [13, 20]. A meta-analysis has concluded that moderate and high levels of physical activity are associated with reduced risk of total, ischemic, and hemorrhagic strokes [21].
The association between physical activity and cancer is controversial. Meta-analyses of population-based studies have shown an inverse dose—response association between physical activity and colon cancer [22, 23], and indicates that higher levels of physical activity in leisure time protect against lung cancer [24]. In a combined population study of 28 000 men and women in Copenhagen, there was none or only a weak, inverse association between physical activity in leisure time and incidence of cancer, except for cancer of the ovary [25].
There are to our knowledge no studies that specifically focus on the association between mortality from respiratory disease and leisure-time physical activity, but studies linking respiratory morbidity with physical activity found a higher level of lung function and lower incidence of respiratory infections in subjects who were physically active [26–28].
In all studies cited above the level of physical activity in leisure time has been measured only at a single examination, and thus the association between physical activity and mortality could be weakened if the participants decrease their physical activity during the observation period. We suggest that it is of importance to include measurements of more than one examination, when analysing the association between leisure-time physical activity and mortality.
In the present observational study we investigated the association between the level of leisure-time physical activity at two examinations 5 years apart, in 1976–1978 and 1981–1983, and subsequent mortality from coronary heart disease, stroke, respiratory diseases, cancer and all-causes.
Materials and methods
Participants
The Copenhagen City Heart Study is a prospective cardiovascular population study comprising a random sample of 9145 men and 10 184 women aged 20–93 years who were drawn from the Copenhagen Population Register as of 1 January 1976 [29]. The first examination was carried out in 1976–1978 (participation rate 74%) and the second in 1981–1983 (participation rate 70%), 11 100 persons 20–79 years of age participated in the first two examinations. The present analysis comprises 2136 men and 2758 women aged 20–79 years at the first examination, who attended both examinations, and did not change leisure-time physical activity level from the first to the second examination. None had experienced a history of coronary heart disease, stroke, cancer, or respiratory diseases at the second examination 1981–1983; that is, the participants had not been admitted to hospital and thus registered in The National Patient Register or The Danish Cancer Registry before the beginning of follow-up in 1981–1983. Information on all covariates needed for the analyses was obtained from all participants.
Survey method
Established procedures and examinations for cardiovascular epidemiologic surveys were used [30]. A self-administered questionnaire requesting information about physical activity, smoking, alcohol consumption, and socio-economic status was completed and checked by the staff. Blood pressure (measured by the London School of Hygiene sphygmomanometer), plasma cholesterol and glucose concentrations, body mass index, and forced respiratory volume in the first second of expiration (FEV1) were measured as previously described [29]. Identical study methods were applied in the first and second examination.
Physical activity during leisure time was graded in four levels based on a questionnaire constructed by Saltin and Grimby [31], with minor modifications. Levels of activity were defined as follows: (1) almost entirely sedentary (e.g. reading, watching television or movies, engaging in light physical activity such as walking or biking for less than 2 h per week); (2) light physical activity for 2–4 h per week; (3) light physical activity for more than 4 h per week or more vigorous activity for 2–4 h per week (e.g. brisk walking, fast biking, heavy gardening, sports that cause perspiration or exhaustion); and (4) highly vigorous physical activity for more than 4 h per week or regular heavy exercise or competitive sports several times per week. In this analysis 1 was considered low physical activity, 2 was considered moderate physical activity and categories 3 and 4 were combined and considered as high physical activity in leisure time. We assumed that low, moderate, and high physical activity corresponded to <4, 4–6 and >6 metabolic equivalents, respectively. Only persons with unchanged physical activity in leisure time at the two examinations 5 years apart were included in the analysis.
Endpoints
Participants were followed from the second examination in 1981–1983 until 31 December 2000, or death, using the unique personal identification number in the National Central Person Register and The Register of Causes of Death. During this observation period, Denmark shifted from the eighth version of International Classification of Diseases (ICD) to the 10th version, which came into use in January 1994. We analysed separate endpoints comprising deaths from CHD, ICD-8 diagnosis codes 410–414 until 1 January 1994, ICD-10 I21–I25 from 1994 to 2000; deaths from stroke, ICD-8 430–438 and ICD-10 I60–I69 and G45 respectively; deaths from cancer, ICD-8 140–209 and ICD-10 C00–D09 and deaths from respiratory diseases, ICD-8 460–519 and ICD-10 J00–J99. For each participant only the main cause of death was used in the analysis.
Statistical methods
To assess the independent effect of physical activity on mortality, Cox's proportional hazards regression analysis was used with age as underlying timescale and delayed entry accordingly, thereby adjusting for age [32]. We tested for interaction between physical activity and sex. When we analysed men and women together we performed a sex-stratified Cox analysis, thus assuming the same effect of covariates in men and women but allowing for different baseline hazards. Relative risks were calculated as proportional hazards ratios. Additional covariates measured at the second examination were included as categorical dummy variables: smoking status (no, former, current), plasma total cholesterol (< 5, 5–6.9, ≥ 7 mmol/l), high-density lipoprotein (HDL)-cholesterol (< 1, 1–1.2, ≥ 1.3 mmol/l), systolic blood pressure (< 140, 140–159, ≥ 160 mmHg, antihypertensive medication), diabetes mellitus (none, non-insulin-dependent diabetes mellitus/non-fasting plasma glucose ≥ 11.1 mmol/l, insulin-dependent diabetes mellitus), alcohol consumption (< 1, 1–13, 14–69, ≥ 70 beverages per week), body mass index (< 20, 20–24.9, 25–29.9, ≥ 30 kg/m2), education (< 8, 8–10, ≥ 11 years of school), and income (low, middle, high; approximately equivalent to a pre-tax income of <1000, <1000–<2000, > <2000 per month) and FEV1 expressed in percent of predicted value (% predicted) into three groups (< 60% predicted; 60–79.9% predicted; ≥ 80% predicted). To estimate the difference in remaining lifetime between subjects in different physical activity groups we used Kaplan—Meier plots, with age as timescale and for which subjects were not included until they reached age 50. Tests for trend were done by linear, logistic or Cox regression (df = 1). All analyses were performed by the statistical software packages SAS (SAS System for Windows, release 8.02; SAS Institute Inc., Cary, North Carolina, USA) and Stata (Stata Statistical Software: Release 6.0; Stata Corporation, College Station, Texas, USA).
Results
Baseline characteristics of the 4894 persons, 2136 men and 2758 women, at the second examination in 1981–1983 (i.e. at the start of follow-up) are presented in Table 1. The data show a clear tendency towards a higher risk factor burden for both men and women in the low physical activity group, especially regarding, age, smoking, HDL-cholesterol, antihypertensive drugs, systolic blood pressure, education, household income and FEV1% predicted.
During follow-up 1787 persons died: 927 men and 860 women. Table 2 presents the total numbers of deaths from CHD, stroke, cancer, respiratory diseases, and all causes in relation to leisure-time physical activity in men and women, respectively.
Table 3 presents the relative risks of cause-specific and all-cause mortality in relation to leisure-time physical activity level. Both univariate and multivariate analyses are shown. A low activity level at both examinations served as the reference category for relative risk estimation. Initially we analysed the mortality for men and women separately, but as we found similar results in the two sexes, we only present the results for both sexes combined. In the univariate analysis, adjusting for age and sex, there was an inverse significant association between leisure-time physical activity and risk of death from CHD, cancer, respiratory diseases and from all causes. Although the relative risk of death from stroke was below 1 for both moderate and high compared with low physical activity, this association did not reach the level of statistical significance. In the multi-variate model, we included the following covariates: smoking, total cholesterol, HDL-cholesterol, systolic blood pressure, diabetes mellitus, alcohol consumption, body mass index, education, income and FEV1% predicted.
Men and women engaging in long-term moderate or high leisure-time physical activity experienced a significantly lower risk of death from CHD, relative risk (95% confidence intervals) in multivariate analyses was 0.71 (0.51–0.99) for moderate activity and 0.56 (0.38–0.82) for high activity. The physically active also experienced a significantly lower risk of cancer: moderate activity 0.77 (0.61–0.97) and high activity 0.73 (0.56–0.95). The same was true for all-cause mortality: moderate physical activity 0.78 (0.68–0.89) and high 0.75 (0.64–0.87); both sexes were combined. For deaths from respiratory diseases there was no significant risk reduction, although the relative risk (RR) for both moderate and high physical activity was below 1. In particular, the introduction of FEV1% predicted in the regression model had a pronounced effect on the RR of death from respiratory disease. For stroke, the RR also was below 1 for both moderate and high physical activity, but the association was not significant.
Using Kaplan—Meier plots we also calculated the gained years of expected lifetime, which is the difference in median survival between a 50-year-old person in the low, moderate and high physical activity group. Men with high physical activity in leisure time survived 6.8 years and men with moderate activity 4.9 years longer than men with a low activity level. For women the figures were 6.4 and 5.5 years, respectively.
Baseline characteristics for leisure-time physical activity levels
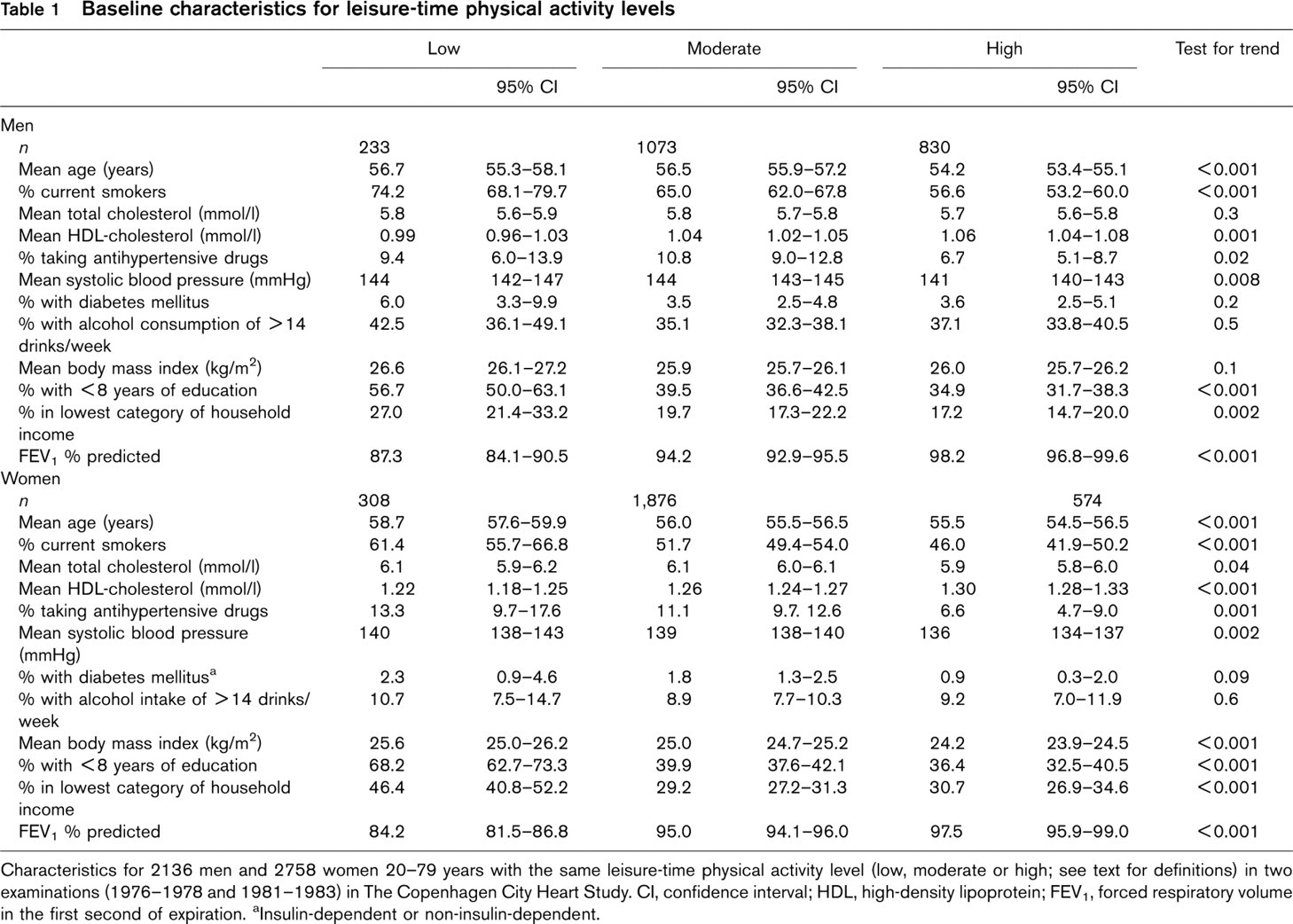
Characteristics for 2136 men and 2758 women 20–79 years with the same leisure-time physical activity level (low, moderate or high; see text for definitions) in two examinations (1976–1978 and 1981–1983) in The Copenhagen City Heart Study. CI, confidence interval; HDL, high-density lipoprotein; FEV1, forced respiratory volume in the first second of expiration. aInsulin-dependent or non-insulin-dependent.
Cause-specific and all-cause mortality for leisure-time physical activity level
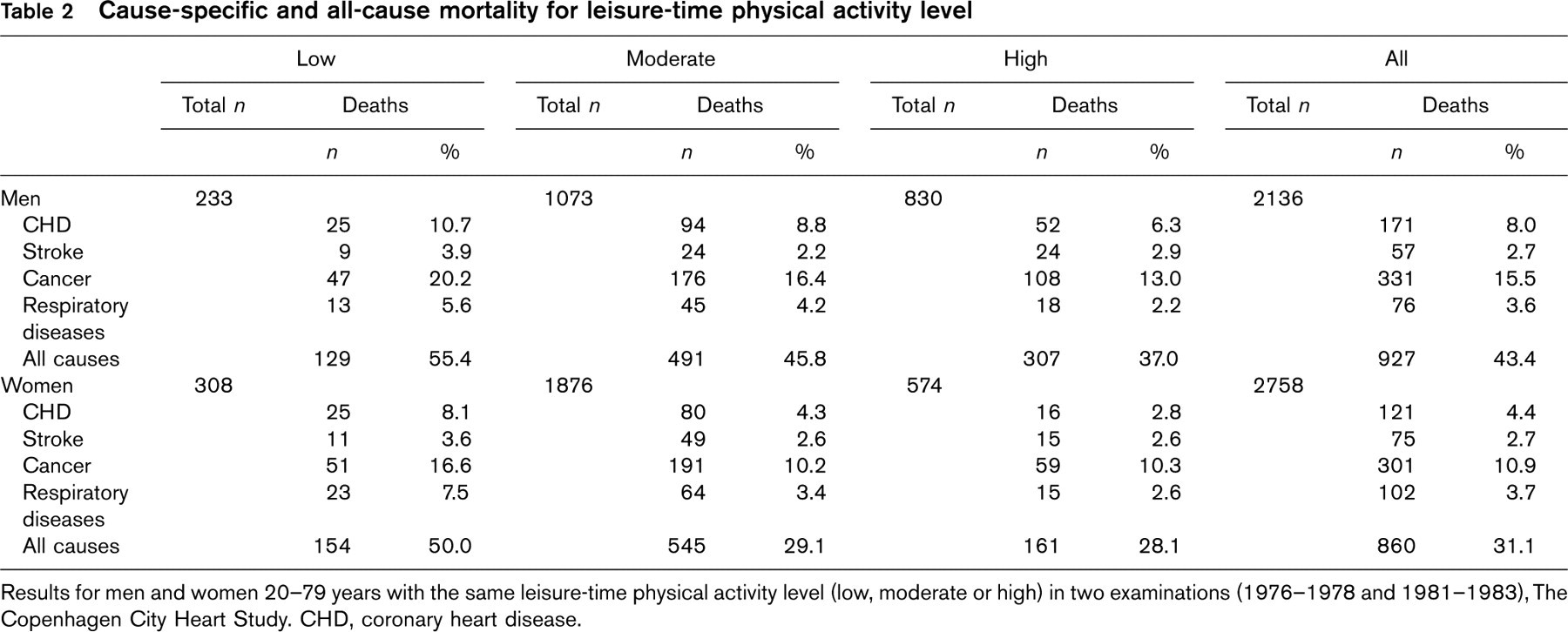
Results for men and women 20–79 years with the same leisure-time physical activity level (low, moderate or high) in two examinations (1976–1978 and 1981–1983), The Copenhagen City Heart Study. CHD, coronary heart disease.
Discussion
This observational study of 4894 healthy men and women of which 1787 died during follow-up has shown an inverse and significant dose—response association between leisure-time physical activity and mortality from CHD, cancer and from all causes in both sexes. These findings are in agreement with previous studies [5, 10–16]. For CHD, there was a dose—response relation: the higher the physical activity, the lower the risk of death. This was also the case for cancer and all-cause mortality. There was no significant association between physical activity and death from stroke in our population. One study reported that low physical activity is associated with the lowest risk of stroke [13], others have found none or an inverse association [13, 16, 20, 33].
Relative risk (RR) of cause-specific and all-cause mortality in men and women together for leisure-time physical activity level
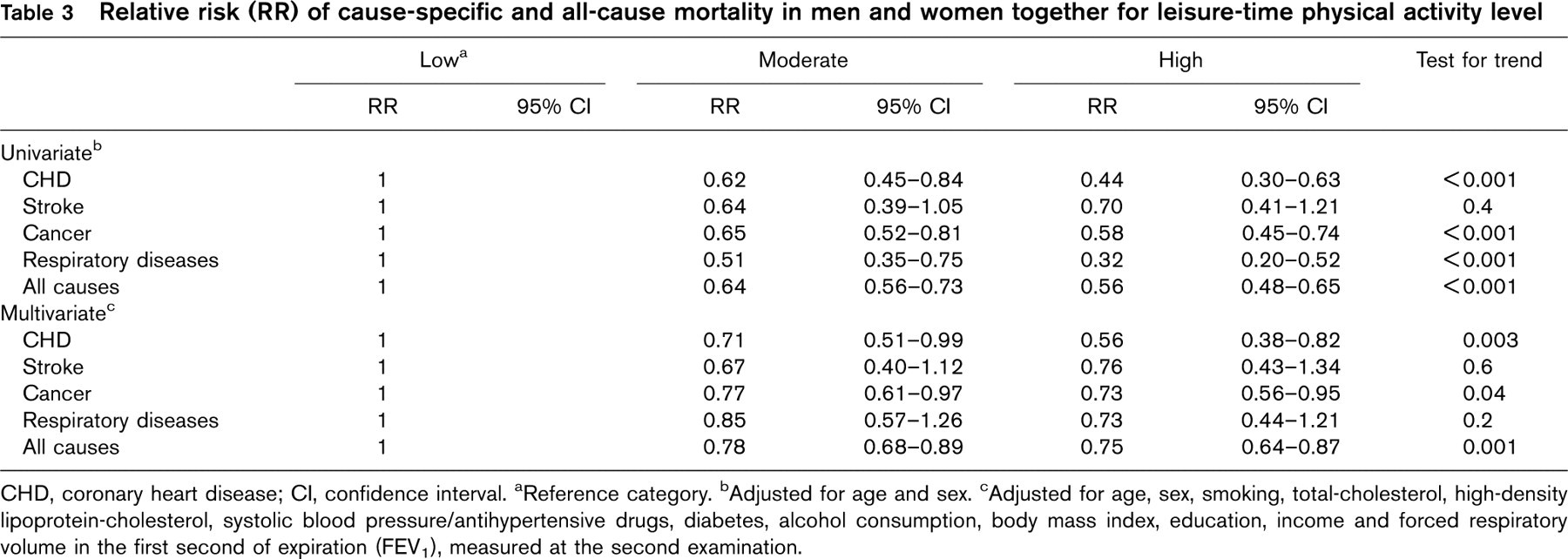
CHD, coronary heart disease; CI, confidence interval. aReference category. bAdjusted for age and sex. cAdjusted for age, sex, smoking, total-cholesterol, high-density lipoprotein-cholesterol, systolic blood pressure/antihypertensive drugs, diabetes, alcohol consumption, body mass index, education, income and forced respiratory volume in the first second of expiration (FEV1), measured at the second examination.
Both the univariate and the multivariate analyses have shown a protective role of leisure-time physical activity on mortality from cancer. We have not analysed specific types of cancer in this paper, but we did so in another report based on three large cohorts in Copenhagen. We found a highly significant inverse relation between vigorous physical activity in postmenopausal women and cancer of the ovary. Furthermore, we found an inverse relation between physical activity and cancer of the colon for men, but not for women. We found no protection for breast cancer, but non-melanoma skin cancer in men was significantly associated to leisure-time physical activity [25].
The univariate analysis showed a strong inverse relationship between higher levels of physical activity and risk of respiratory death. In the multiple regression analysis without FEV1 as a covariate, this association remained significant, but it was insignificant after inclusion of FEV1% predicted as an additional variable in the model. This is likely, because reduced FEV1 is, in addition to being a strong predictor of mortality [34], also a limiting factor for physical activity. As anticipated, in the present population we observed that participants with low FEV1 reported less physical activity than those with higher FEV1. The lack of a significant association between physical activity and respiratory mortality does not necessarily mean that physical activity is without effect on respiratory diseases. When comparing the association between physical activity and total mortality with the association between physical activity and respiratory disease mortality, the RRs are of similar magnitude, but the statistical significance in case of total mortality is the result of a higher number of endpoints. In addition, several clinical intervention studies of physical training on patients with lung diseases, in particular chronic obstructive pulmonary diseases (COPD), have shown beneficial effects on various health measures including quality of life and hospital admissions [35]. Also an observational study of patients with established COPD showed that high levels of physical activity were associated with lower incidence of hospital admissions [36]. There are, however, to our knowledge no studies showing a beneficial effect of physical activity on mortality in patients with lung diseases.
Assessment of leisure-time physical activity is difficult. The questionnaire used discriminates sedentary participants from their more active counterparts with respect to maximal oxygen uptake [37]. Furthermore, the questionnaire has revealed significant associations between physical activity level and mortality [38]. To diminish the risk of misclassification in the present analyses, we assessed the leisure-time physical activity on two examinations 5 years apart. All participants belonged to either low, moderate or high leisure-time physical activity at both examinations. All were healthy at the start of follow-up in 1981–1983, so none belonged to the low level of physical activity because of a history of coronary heart disease, stroke, cancer or respiratory diseases. Furthermore none of the participants had been admitted to hospital between 1976, 1978, 1981 and 1983, before the follow-up.
We have found that several men and women in our study changed level of leisure-time physical activity between the first and second examination 5 years apart: of those with high physical activity 42% changed to moderate or low, and of those with moderate activity 13% changed to low and 29% to high, whereas of those with low activity 63% increased to moderate or high [38]. In another study analysing jogging at two examinations 5 years apart and the relative risk of death, we found that persistent joggers had a significantly lower mortality than non-joggers and those who jogged at only one of the two examinations [39]. Thus we suggest that it is of importance to include measurements of more than one examination, when analysing the association between leisure-time physical activity and mortality.
Plausible mechanisms behind the association between mortality from CHD and leisure-time physical activity include increased insulin sensitivity, improved lipid profile, lower blood pressure, reduced platelet aggregation, increased fibrinolytic activity, improved cardiac function, increased oxygen uptake, lower resting heart rate, reduction of C-reactive protein and prevention of obesity [40–42].
Because our study was observational and not a randomized trial, we can demonstrate associations but not causalities. We stress, however, that our cohort was a large random sample that included both men and women from the general population of Copenhagen, and the attendance rate of those invited was high. Furthermore, the risk estimates were adjusted for smoking, total cholesterol, HDL-cholesterol, systolic blood pressure, diabetes mellitus, alcohol consumption, body mass index, education, income and FEV1 (% predicted).
In conclusion, these data from a large observational population study indicate, that risk of death is significantly lower in physically active persons, than in their sedentary counterparts. Thus, moderate physical activity in leisure time should be encouraged to decrease the risk of premature death. For CHD high physical activity seems even more beneficial than moderate.