
Abstract
Background
Risk reduction of myocardial infarction has been shown for leisure time physical activity. The results of studies on occupational physical activity and risk of myocardial infarction are incongruous and studies on commuting activity are scarce. The aim of this study was to investigate how commuting activity, occupational physical activity and leisure time physical activity were associated with risk of future first myocardial infarction.
Design
We used a prospective incident case-referent study design nested in Västerbotten Intervention Program and the Northern Sweden MONICA study.
Methods
Commuting habits, occupational physical activity, leisure time physical activity and cardiovascular risk factors were assessed at baseline screening and compared in 583 cases (20% women) with a first myocardial infarction and 2098 matched referents.
Results
Regular car commuting was associated with increased risk of myocardial infarction versus commuting by bus, cycling or walking [odds ratio (OR) 1.74; 95% confidence interval (CI), 1.20–2.52] after multivariate adjustment. High versus low leisure time physical activity was associated with reduced risk of myocardial infarction (OR 0.69; 95% CI, 0.50–0.95) after adjustment for occupational physical activity and commuting activity, but the association was not statistically significant after further multivariate adjustment. After multivariate adjustment we observed a reduced risk for myocardial infarction in men with moderate (OR 0.70; 95% CI, 0.50–0.98) or high (OR 0.67; 95% CI, 0.42–1.08) versus low occupational physical activity.
Conclusions
We found a clear association between car commuting and a first myocardial infarction and a corresponding inverse association with leisure time physical activity, while the impact of occupational physical activity on the risk of myocardial infarction was weaker.
Introduction
Ever since protection against coronary heart disease (CHD) was shown in active bus conductors compared with sedentary drivers in the 1950s [1], multiple subsequent epidemiological studies have demonstrated an inverse relationship between physical activity and risk of CHD [2, 3]. A new paradigm ‘lifestyle physical activity’ was introduced in the late 1990s. Evidence for substantial health benefits from physical activity even at moderate intensity had been assembled and led to a new public health recommendation by which every individual should accumulate at least 30 min of moderate intensity physical activity each day [4].
The difficulties in motivating individuals with sedentary lifestyles remain. Despite the health benefits, large proportions of the population are simply not interested in leisure time physical activity. The inverse relationship between physical activity and risk of CHD has been shown predominantly in studies with focus on leisure time physical activity, whereas the effect of occupational physical activity tends to vary between studies. Only a few previous studies [5–9] have investigated the association between commuting activity and risk of cardiovascular disease (CVD). Convincing evidence is needed to show that physical activity, when incorporated in everyday life and achieved in an affordable and not too time-consuming manner, will reduce cardiovascular risk.
The aim of this study was to investigate how commuting activity and occupational and leisure time physical activity were associated with risk of future first myocardial infarction (MI).
Methods
Study population
We used a prospective incident case-referent study design nested in Västerbottens Intervention Program (VIP) and the WHO MONICA study in northern Sweden. In the framework of MONICA, population-based surveys were performed in 1986, 1990, 1994 and 1999 [10]. In VIP, which started in 1985, all men and women 30, 40, 50 and 60 years of age were invited to participate in a health survey at their local primary healthcare center (since 1996 at 40, 50 and 60 years of age). The participants in the present study were asked to complete a questionnaire concerning cardiovascular risk factors, work conditions and lifestyle. Examinations with regard to cardiovascular risk factors such as blood pressure and lipid status were performed on all participants. VIP represented 86.1% of the cohort.
All cases of MI from the MONICA area have since 1985 been included in the Northern Sweden MONICA registries. Six hundred and fifty-one cases fulfilled criteria for a first MI defined by the Northern Sweden MONICA registry [11] and had participated in the MONICA or VIP surveys prior to the MI. From the population-based surveys in VIP and MONICA, 2238 referents (one or more per case) were randomly selected and matched for sex, age (± 2 years), date of health survey (± 1 year) and geographical region. Cases and referents were excluded if previous MI, stroke or malignant disease could not be excluded according to questionnaire or case records. Greatly reduced exercise habits during the year prior to baseline was an exclusion criterion to avoid bias from the possibility that individuals who had reduced their physical activity due to subclinical disease may enter the study. Furthermore, individuals who stated use of nitrates or other heart medicine during 14 days prior to screening were excluded because they might have suffered from CHD at baseline. Five hundred and eighty-three cases and 2098 referents remained after exclusions. The study was approved by the Research Ethics Committee of Umeå University and data handling procedures were approved by the National Computer Data Inspection Board. All participants gave informed consent.
Variables and diagnosis
Hypertension was defined as systolic blood pressure of 160 mm Hg or above or diastolic blood pressure of 95 mmHg or above or because the patient reported use of antihypertensive drug treatment during a period of 14 days before the health survey. Smokers were divided into daily smokers and non-smokers. Ex-smokers were defined as non-smokers. Statements on diabetes were obtained from the questionnaire. Body mass index (BMI) was calculated after measurements of body weight and height, as weight (kilograms) divided by height (meters) squared.
Statements on physical activity were obtained from the questionnaire. The questionnaire design differed on physical activity between the two surveys and the answers were compiled into three categories to create well defined groups of low and high physical activity. Individuals stating sedentary work or almost never physically demanding work were categorized as low occupational physical activity. Individuals stating highly physically demanding work or often physically demanding work were categorized as high occupational physical activity. Remaining individuals represented a middle group categorized as moderate occupational physical activity. Individuals stating no exercise for the last 3 months or who were never physically active during leisure time for the last year were categorized as low leisure time physical activity. Individuals stating exercise at least two to three times a week or at least 3 h a week were categorized as high leisure time physical activity. Remaining individuals represented a middle group categorized as moderate leisure time physical activity.
From subjects attending the VIP survey we obtained data on individual commuting habits. Separate answers were given for the four seasons. Questions concerning commuting habits were not present in the MONICA questionnaire and these subjects were not included in analysis of commuting activity. Level of educational attainment was defined as elementary school, vocational school, upper secondary school or university degree.
A diagnosis of MI was confirmed if the event met MONICA criteria [12]. For fatal MIs we also accepted diagnosis based on necropsies and on deaths confirmed by records as being caused by CHD (ICD-9 codes 410–414, 429.2, ICD-10 codes I20–I25). For fatal MIs, possible MIs were also accepted. Silent MIs found on routine examination were not included because they could not be assigned an accurate date of occurrence.
Blood sampling and laboratory procedures
Venous blood serum samples for lipid measurements were obtained after 4 h or more of fasting. Total cholesterol was measured by enzymatic methods with Reflotron bench-top analyzers (Boehringer Mannheim GmbH, Mannheim, Germany) at each health survey center at the time of the health survey. The mean interassay coefficient of variation for this analysis was 2.6%.
Statistical analyses
Proportions and mean values of cardiovascular risk factors and measures of physical activity were calculated for cases and referents separately for both sexes. In order to compare characteristics between cases and referents and men and women, respectively, we used the Mann-Whitney two independent samples test for continuous variables and the χ2 test for categorical variables. In comparisons of characteristics of physical activity categories we used the Kruskal-Wallis Several Independent test for continuous variables and the χ2 test for categorical variables. A P-value under 0.05 was considered statistically significant. To account for the matching variables and potential confounding factors simultaneously, conditional logistic regression analysis was used to estimate relative risks by calculating odds ratios (ORs) and 95% confidence intervals (CIs) in univariate and multivariate models. The χ2 linear-by-linear association test for trend was used for trend analyses. Statistical analyses were performed using SPSS software package for PC version 11.5 (SPSS, Chicago, Illinois, USA).
Missing values
The proportions missing values per variable were as follows: smoking 5.0%, diabetes 3.9%, BMI 3.4%, hypertension 3.7%, cholesterol 4.4%, level of educational attainment 14.1%, leisure time physical activity 14.4%. For commuting activity the proportion missing values was 9.1% and for occupational physical activity 9.4%. In addition, 194 individuals had a disability or old-age pension and for 779 individuals questions concerning commuting habits were not present in the questionnaire. In the conditional multivariate logistic regression tests, missing values were replaced by the mean value for the referent group in the continuous variables and in the categorical variables categorized in a separate group. This allowed all subjects to be included in the conditional multivariate logistic regression analyses.
Results
MI for the 583 cases occurred on average 4 years and 5 months after the initial participation in the health survey. Established risk factors, commuting activity and physical activity variables for 109 women and 474 men who developed a first MI and for the matched referents are presented in Table 1. A university degree was less common in cases, whereas smoking, diabetes, hypertension and car commuting were more common in cases. Furthermore, cases had higher mean cholesterol concentrations, systolic and diastolic blood pressures and BMI.
Mean baseline characteristics for 583 cases and 2098 referents subjects at health survey
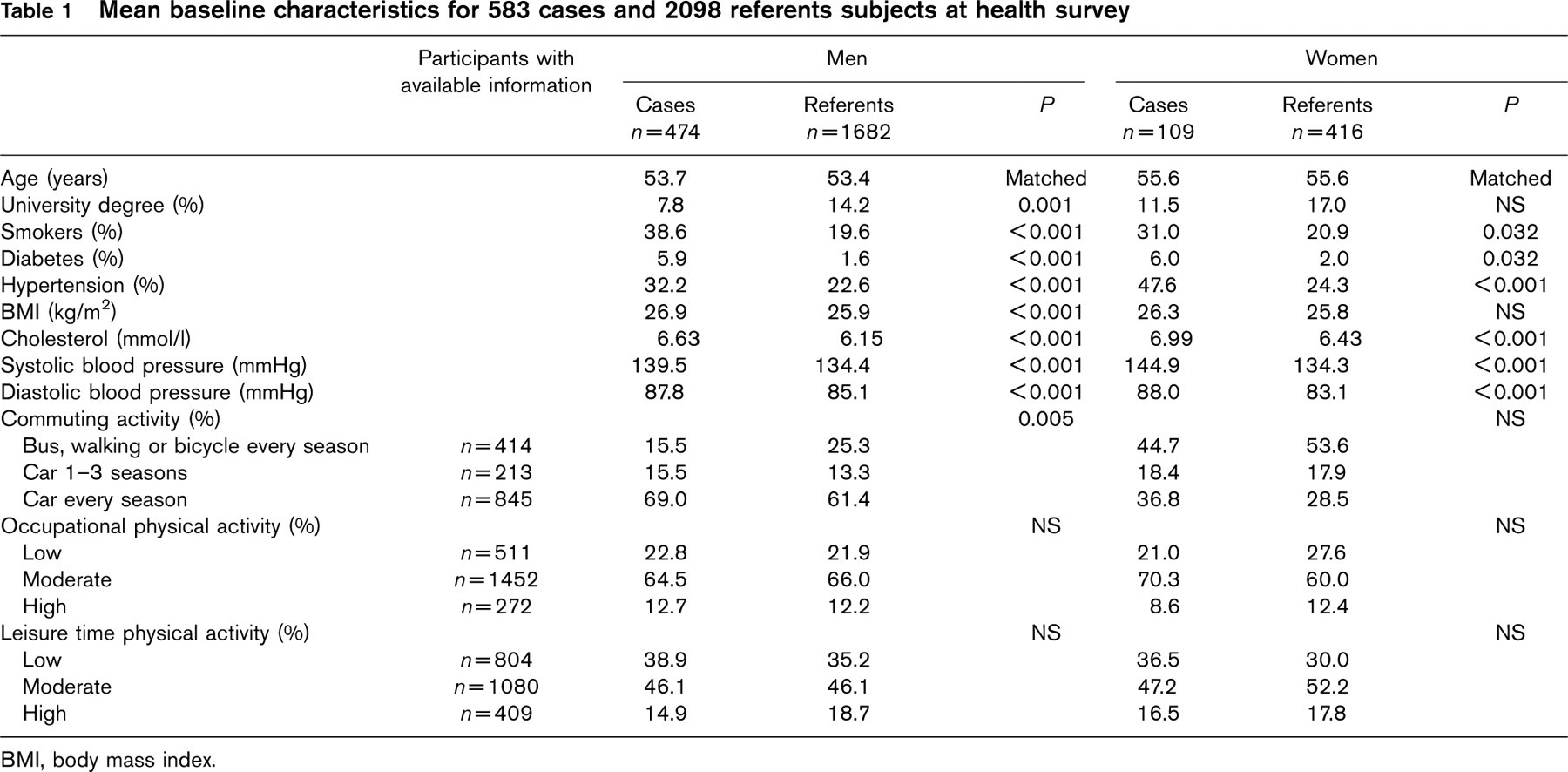
BMI, body mass index.
Comparison between men and women, including comparing only referents showed that women had significantly lower BMI and diastolic blood pressure and higher mean cholesterol concentrations than men. Moreover, car commuting was more common for men while low occupational physical activity was more common among women.
In Table 2, risk factors with both sexes combined are presented in relation to subgroups of commuting activity, occupational and leisure time physical activity. Comparison between the subgroups showed that smoking was more common among individuals with low leisure time physical activity. Furthermore, car commuters had higher BMI and were, like individuals with high occupational physical activity, associated with higher mean cholesterol concentration. A university degree was less common among car commuters and individuals with high occupational physical activity and low leisure time physical activity.
In conditional univariate logistic regression analysis with MI as outcome variable, there were significant associations with smoking, diabetes, hypertension, BMI, cholesterol, systolic and diastolic blood pressure, university degree compared to elementary school (Table 3). Significant associations were also seen for car commuting and high compared to low leisure time physical activity for men and both sexes combined. Occupational physical activity was not associated with risk of MI.
Table 4 presents risk of MI with conditional multivariate logistic regression. Similar trends in risk were seen in men and women for commuting activity, but the association between car commuting and MI was not significant for women. Men who used a car for transportation to work one to three seasons per year or every season were associated with an increased risk of MI after multivariate adjustment (OR 2.04; 95% CI, 1.18–3.53 and OR 1.68; 95% CI, 1.10–2.56, respectively) compared to men who went to work by bus, walked or cycled every season. For occupational physical activity, the trends in risk differed between men and women, showing a significantly lower risk of MI for moderate compared to low occupational physical activity for men in multivariate model 2 (OR 0.70; 95% CI, 0.50–0.98), which included educational attainment level. In multivariate model 1 with adjustment for other forms of physical activity, high compared to low leisure time physical activity was associated with lower risk of MI for men (OR 0.68; 95% CI, 0.47–0.97), but this association was lost after adjustment for remaining confounders in multivariate model 2. A nonsignificant trend for lower risk for moderate and high compared to low leisure time physical activity was seen in women in both multivariate models.
Discussion
The strengths of this study include the prospective design, the strict criteria for clinical variables and diagnosis, and the high participation rate in the health surveys. Furthermore, our referents were matched for geographical area to minimize the effect of different local lifestyle patterns. The geographical matching may also reduce the effect of genetic stratification, since the total population of northern Sweden is quite heterogeneous, while the larger river valleys in the region are home to distinct genetic sub-isolates [13]. Our study is limited by the fact that data on physical activity were self-reported with no separate estimation on intensity or duration and the questionnaires were not validated against other methods. Furthermore, statements on physical activity were only given on one occasion and questions on commuting activity were not included in all questionnaires.
One major finding was an association between car commuting and risk of MI. This association was not confounded by levels of traditional cardiovascular risk factors, attained educational level or occupational and leisure time physical activity. Probably due to the differences in sample size between sexes, the association was only significant in men. A second major finding was the protective effect of high physical activity during leisure time. We also found an association between occupational physical activity and risk of MI. This association was only shown in men and only after extensive adjustments, but in contrast to commuting activity the trends in risk at different levels of occupational activity differed between men and women.
Mean baseline characteristics in relation to subgroups of commuting activity, occupational and leisure time physical activity
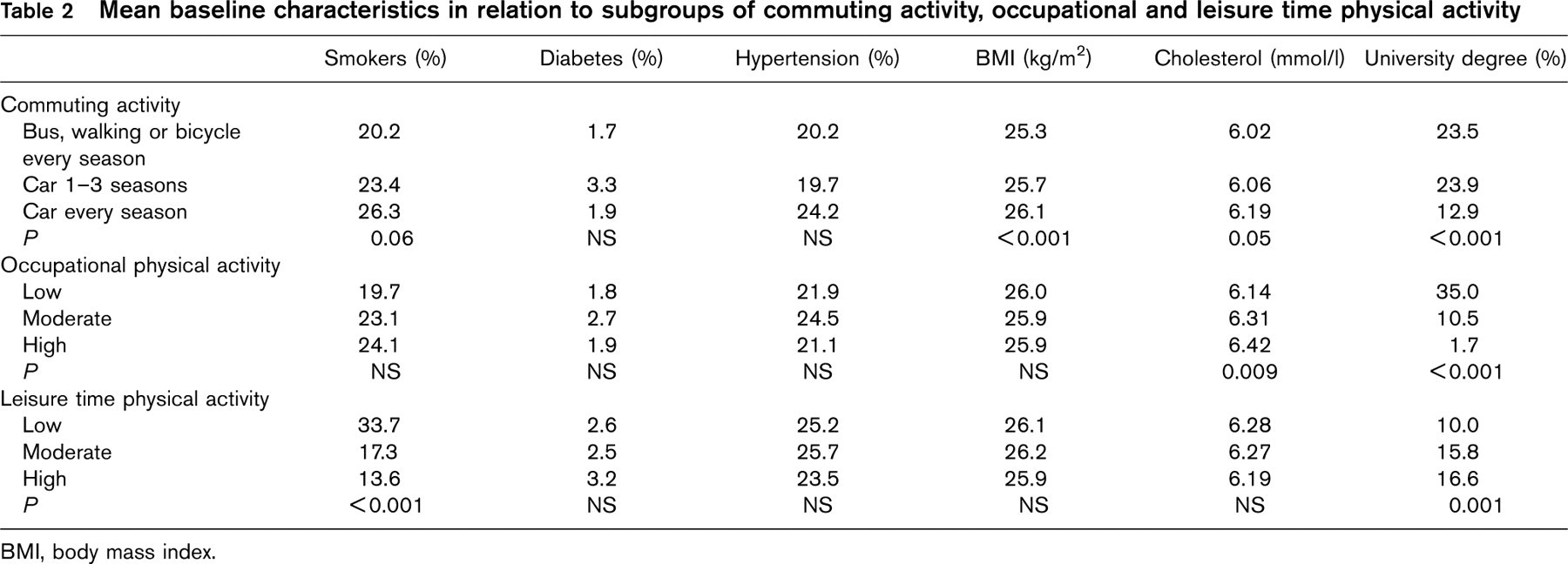
BMI, body mass index.
Risk of myocardial infarction with conditional univariate logistic regression and χ2 linear-by-linear association test for trend
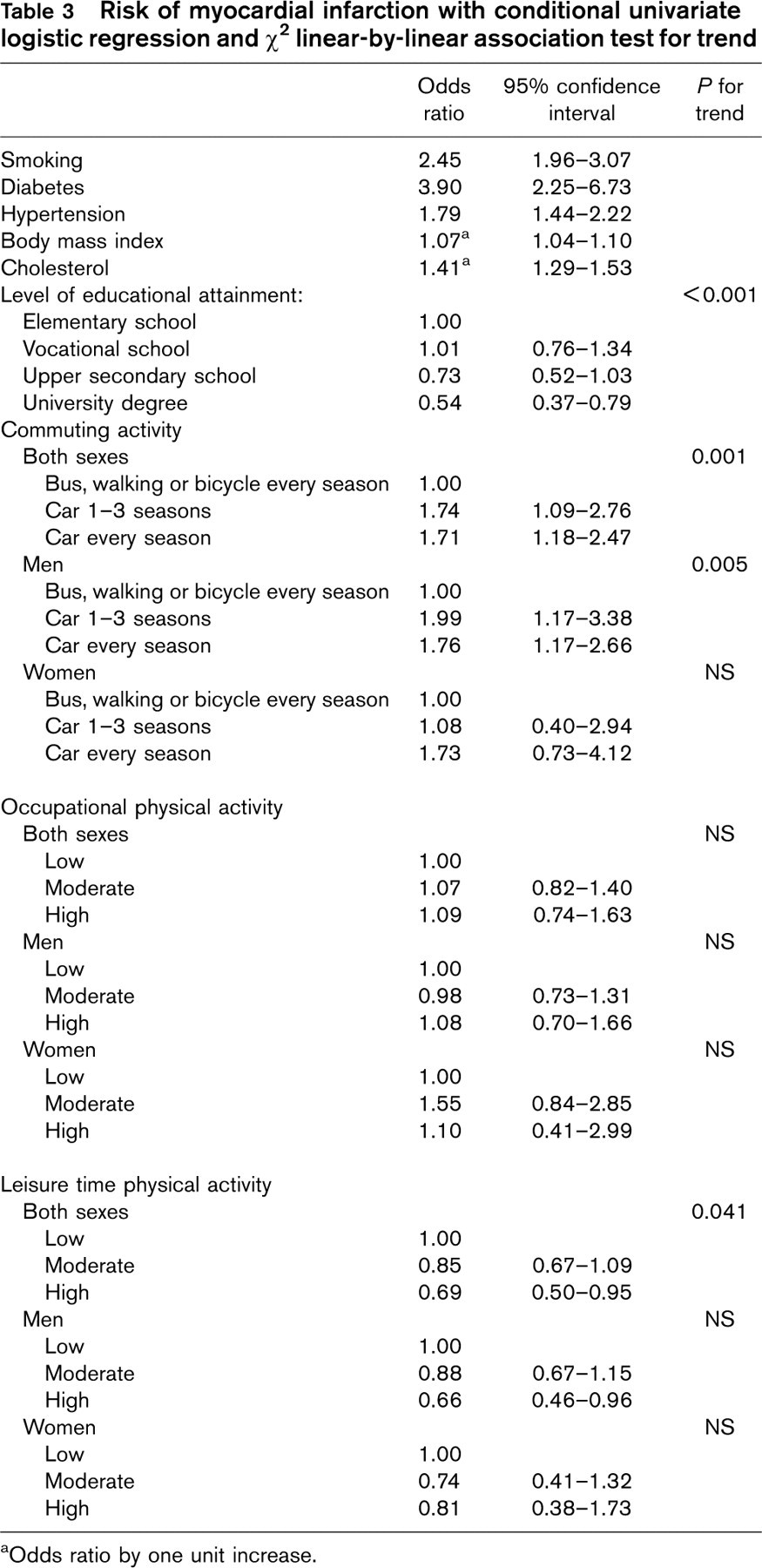
aOdds ratio by one unit increase.
When comparing the levels of cardiovascular risk factors in the present study to the INTERHEART study [14] in Western Europe, smoking and diabetes were less common among referents in our study, while hypertension was somewhat more common. Lipid levels could not be compared since the INTERHEART study used ApoB/ApoAI ratio as an index of abnormal lipids. Previous international comparisons, however, have shown relatively high lipid levels in northern Sweden. In the INTERHEART study, regular physical activity (moderate or strenuous exercise for 4h or more a week) were significantly related to MI with an OR of 0.86 (99% CI, 0.76–0.97) after multivariate adjustment. The majority of previous studies on physical activity and CVD have not separated the physical activity variable in commuting activity, occupational and leisure time physical activity. This fact can partly explain a somewhat weaker association between leisure time physical activity and risk of MI in our study compared to previous studies [2, 3, 14].
A study by Barengo [5] and co-workers in a Finnish population, demonstrated that moderate and high levels of leisure time physical activity and occupational physical activity were associated with reduced risk of CVD mortality in both sexes. Women spending 15 min or more walking or cycling to and from work daily had reduced CVD mortality, but the association was no longer significant after adjustment for leisure time physical activity and occupational physical activity. Other Finnish studies have shown associations between active commuting (walking or cycling) and reduced risk of ischemic stroke [15], type 2 diabetes [16], cardiovascular death among subjects with type 2 diabetes [7], and antihypertensive drug treatment [6]. The association between commuting activity and all-cause mortality has been investigated in a Danish study [17], which found that bicycling to work decreased risk of mortality by approximately 40% after multivariate adjustment including leisure time, but not occupational physical activity. In our study we chose to investigate car commuting as a determinant for MI, with commuting by bus, walking or bicycle as reference. This was mainly because we did not have statistical power to compare commuting by car with commuting by bus, walking or bicycle in separate analysis. We also considered car commuting to be associated with the least energy expenditure, since many bus commuters have to walk in order to arrive at their bus stop.
Previous studies of the association between occupational physical activity and cardiovascular disease have shown inconsistent results [5, 7, 18–23]. In the present study, moderate compared to low occupational physical activity was associated with a lower risk of MI for men, but not women in multivariate analysis. The findings are more likely to reflect sex differences in professions and work tasks than differences in health benefits from occupational physical activity between men and women. The association is overall weak and in the univariate model no protection at all was associated with occupational physical activity. An explanation for this may be that physical activity at work tends to involve a lower proportion of cardiorespiratory stress and a higher proportion of static workload on peripheral muscles compared with leisure time physical activities like jogging and swimming or active commuting like cycling or walking. Since the inverse relationship between physical activity and risk of CHD has mainly been shown for aerobic exercise [2, 24], the effect of occupational physical activity is consequently lower. In a previous study, anaerobic activities such as heavy lifting at work were related to even increased risk of MI, whereas aerobic physical activities such as exercise or walking at work seemed to reduce the risk [25]. A focus on different occupational activity components will be an important element in future studies on occupational physical activity and CHD.
Risk of myocardial infarction with conditional multivariate logistic regression
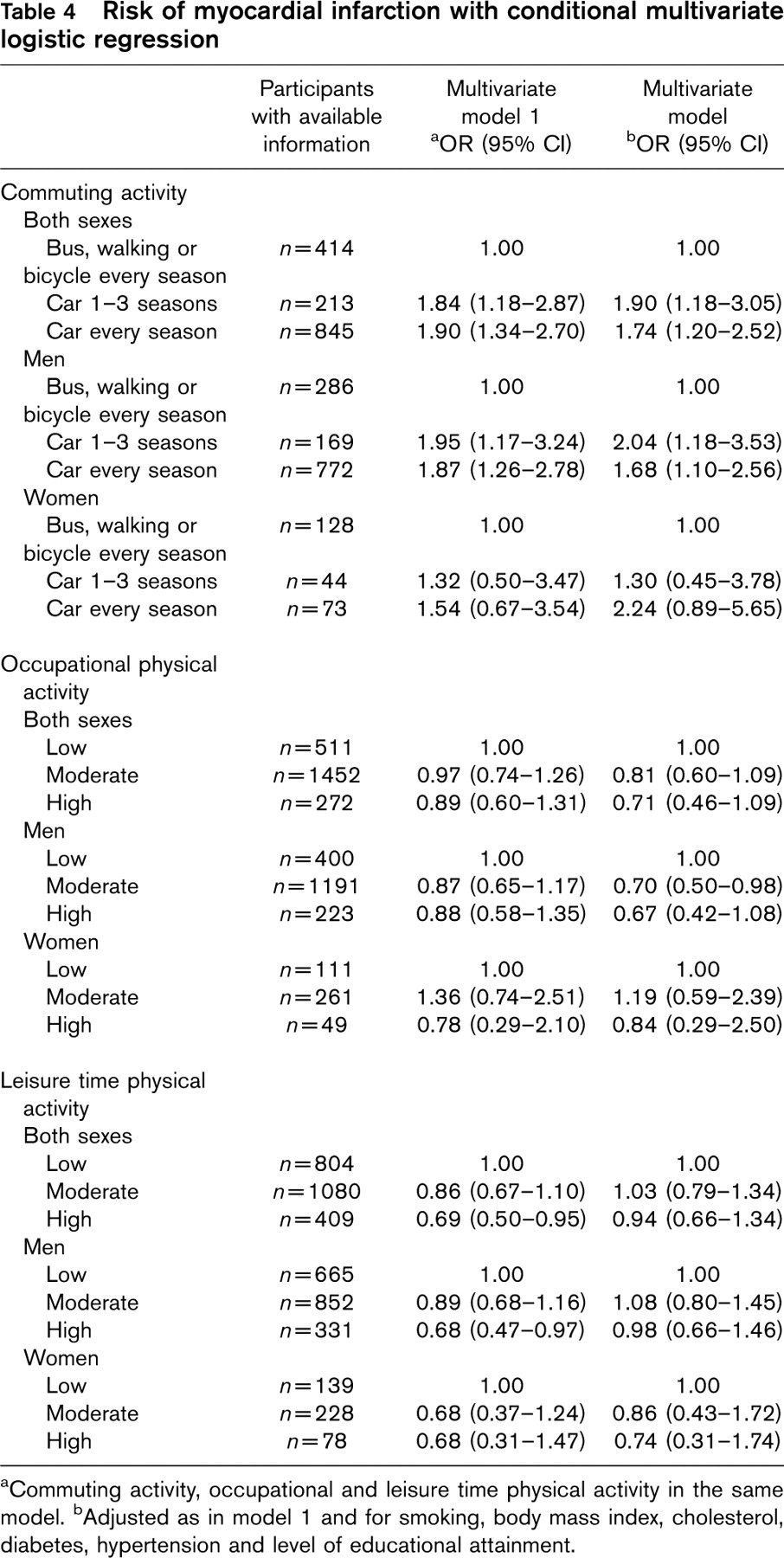
aCommuting activity, occupational and leisure time physical activity in the same model.
bAdjusted as in model 1 and for smoking, body mass index, cholesterol, diabetes, hypertension and level of educational attainment.
Regular physical activity modifies cardiovascular risk factors and reduces the risk of cardiac death for patients with CHD and is therefore widely used in cardiac rehabilitation programs [26]. Meta-analyses have shown growing evidence for an independent role of increased physical activity in the primary prevention of CHD in the last decades [2, 27]. In order to develop behavioral counseling, consistent knowledge is needed about the separate effects of different forms of physical activity on risk of CHD. Our findings of a potent effect in risk reduction for commuting activity supports individualized programs for physical activity in primary prevention, where promoting leisure time physical activity and active commuting can be a way to prevent future CHD.
In conclusion, our major results show an association between car commuting and a first MI and a corresponding inverse association with leisure time physical activity. The impact of occupational physical activity on the risk of MI was weaker than that of commuting activity and leisure time physical activity.
Footnotes
Acknowledgements
We thank Åsa Ågren, Hubert Sjödin, Karin Burman and Thomas Suh for excellent research assistance.