
Abstract
Background
Atherothrombosis is a systemic disease affecting coronary, cerebral, and lower limb arteries, and requiring secondary prevention measures.
Design
Data from three observational studies carried out in 1999-2000 (ECLAT1, APRES, PRISMA) were pooled to describe the prevalence of cardiovascular risk factors and the patterns of drug use in atherothrombotic patients.
Methods
General practitioners and cardiologists engaged in a private practice and evenly distributed in France recruited consecutive patients who had a history of at least one atherothrombotic event: myocardial infarction (MI), ischaemic stroke, and/or peripheral arterial disease (PAD).
Results
The sample was composed of 14 544 patients (men: 75.0%, age 75 or older: 31.0%). At least one of the four major risk factors (smoking, hypertension, hypercholesterolemia, diabetes) was present in 94.3% of the sample. Prevalence of drug use was: 78.8% (antiplatelet agents), 48.5% (statins), 36.7% (beta-blockers), and 33.4% [angiotensin-converting enzyme (ACE) inhibitors]. After adjustment for confounders, statins were taken in a significantly larger extent in patients with a history of isolated MI than in those with a previous ischaemic stroke or PAD, or in patients who suffered from both MI and ischaemic stroke. Isolated MI (as compared with ischaemic stroke and PAD) was significantly and independently associated with a higher probability to take antiplatelet agents, beta-blockers or ACE inhibitors.
Conclusions
At least one conventional risk factor was observed in almost all atherothrombotic patients. Use of preventive drugs was lower in patients with a history of ischaemic stroke or PAD, and should increase, accordingly to the results of recent randomized controlled trials.
Keywords
Introduction
The recent publication of the Third Joint Task Force of European and other Societies on cardiovascular disease prevention in clinical practice [1] has raised new features in the management of cardiovascular prevention as compared with previous guidelines [2]. This new statement emphasizes that the initiation of specific preventive action can be guided by the estimation of the risk of suffering from any cardiovascular event, not only coronary heart disease, but also ischaemic stroke and peripheral arterial disease. Patients with established coronary heart disease, cerebrovascular atherothrombotic disease, or peripheral arterial disease are considered as being at the highest risk of a further vascular event and require intensive lifestyle interventions and appropriate drug therapies. The burden of cardiovascular disease is dramatic in European countries and cardiovascular prevention is a health care priority. The EUROASPIRE [3,4] and PREVENIR surveys [5] have previously described the prevalence of modifiable cardiovascular risk factors and the use of cardiovascular drugs in patients with coronary heart disease, but they did not consider other arterial localizations. Data on the management of patients with myocardial infarction are numerous, but less is known about cerebral and peripheral arterial disease, especially when considering out-of-hospital management.
The observational data shown in the present paper focus on the long-term management of patients with a history of myocardial infarction, ischaemic stroke or peripheral arterial disease, three pathological conditions that share a similar underlying aetiology – atherothrombosis. We described the prevalence of cardiovascular risk factors and the use of cardiovascular drugs in a huge sample of 14 544 patients who presented with at least one prior atherothrombotic event, and who were recruited in the private practices of French general practitioners and cardiologists. We also studied potential differences in risk factors and drug use according to the localization and the extent of the atherothrombotic disease.
Methods
Recruitment of the patients and data collection
The sample analysed in the present work was obtained by pooling patients included in three French observational studies (ECLAT1, APRES and PRISMA) who had a previous history of atherothrombotic disease: myocardial infarction (MI), ischaemic stroke (IS), and/or peripheral arterial disease (PAD). The ECLAT1 [6] and PRISMA [7] studies were two registries designed to estimate the prevalence of subjects with a previous history of atherothrombotic disease among patients of French physicians in a private practice (general practitioners and cardiologists). The APRES study was not designed to be a registry. Its purpose was to assess the incidence of major cardiovascular events in atherothrombotic patients [8]. In each of these three studies, a random sample of general practitioners and cardiologists was constituted by drawing on lists of French physicians in a private practice. Taking the three studies together, 5553 general practitioners and 3189 cardiologists were selected and constituted a sample evenly distributed in France. The ECLAT1 study was carried out on 7 December 2000. All the patients who consulted one of the participating physicians on that day were registered (67 993 patients). Among these 67 993 patients, only 4042 had a previous history of atherothrombotic disease. All these 4042 subjects were included in our pooling analysis. Similarly, 100 429 patients were recruited in the PRISMA study (all the patients who consulted one of the participating physicians during the inclusion period in March–July 1999) [7]. Among these 100 429 patients, 30 430 had a previous history of atherothrombotic disease. Data on cardiovascular risk factors and drug therapy were collected only for the first (up to three) consecutive atherothrombotic patients of each physician, thus providing a sample of 2780 atherothrombotic patients that we studied in the pooling analysis. In the APRES study, a sample of 8967 patients with a previous history of atherothrombotic disease was recruited [the first (up to three) consecutive patients who consulted one of the participating physicians during the inclusion period in April–December 2000]. Only 7783 subjects had complete clinical follow-up data available for the primary criteria and were kept for the analyses. In the pooling study, we analysed the 7722 patients who had complete data on prior atherothrombotic events.
In the three studies, the assessment of myocardial infarction, ischaemic stroke and peripheral arterial disease was based on the diagnosis of the physician in charge of the patient. This method was appropriate since we aimed at studying patients who were known to suffer from an atherothrombotic disease. In each study, the diagnosis had to be documented in the patient's medical file: MI diagnosis was based on hospitalization record and/ or new Q wave on electrocardiogram, IS diagnosis was based on hospitalization record and/or cerebral computed tomography scan and/or magnetic resonance imaging, and PAD diagnosis was based on typical intermittent claudication and ankle-arm systolic index below 0.90, and/or ultrasound duplex or arteriography of the lower limbs. In none of the three studies, unstable angina, hemorrhagic stroke or transient ischaemic attack were considered as inclusion criteria. Patients with a history of embolic stroke were included in the ECLAT1 and PRISMA studies, whereas this vascular event was not a criteria for inclusion in the APRES study.
Similarly, in the three studies, the assessment of hypertension, hypercholesterolaemia, and diabetes mellitus was based on the diagnosis of each patient's physician. Physicians were asked to base their diagnosis on the thresholds commonly used in France to assess hypertension (blood pressure higher than or equal to 140/ 90 mmHg) and diabetes (fasting glycaemia higher than or equal to 7.00 mmol/l) and on the threshold used to start lipid lowering-therapy in secondary prevention (plasma low-density lipoprotein cholesterol higher than or equal to 3.35 mmol/l). Subjects taking antihypertensive, hypercholesterolaemic or hypoglycaemic drugs were systematically considered as suffering from hypertension, hypercholesterolaemia or diabetes, respectively. Smoking status was assessed by each patient's physician. In the ECLAT1 and PRISMA studies, patients were classified as current smokers, past smokers or non-smokers. In the APRES study, smoking status was defined according to two classes only: current and past smoking versus nonsmoking. This latter definition was used in the analysis of the pooling data.
Inclusion criteria and collected data in the ECLAT1, APRES, and PRISMA studies
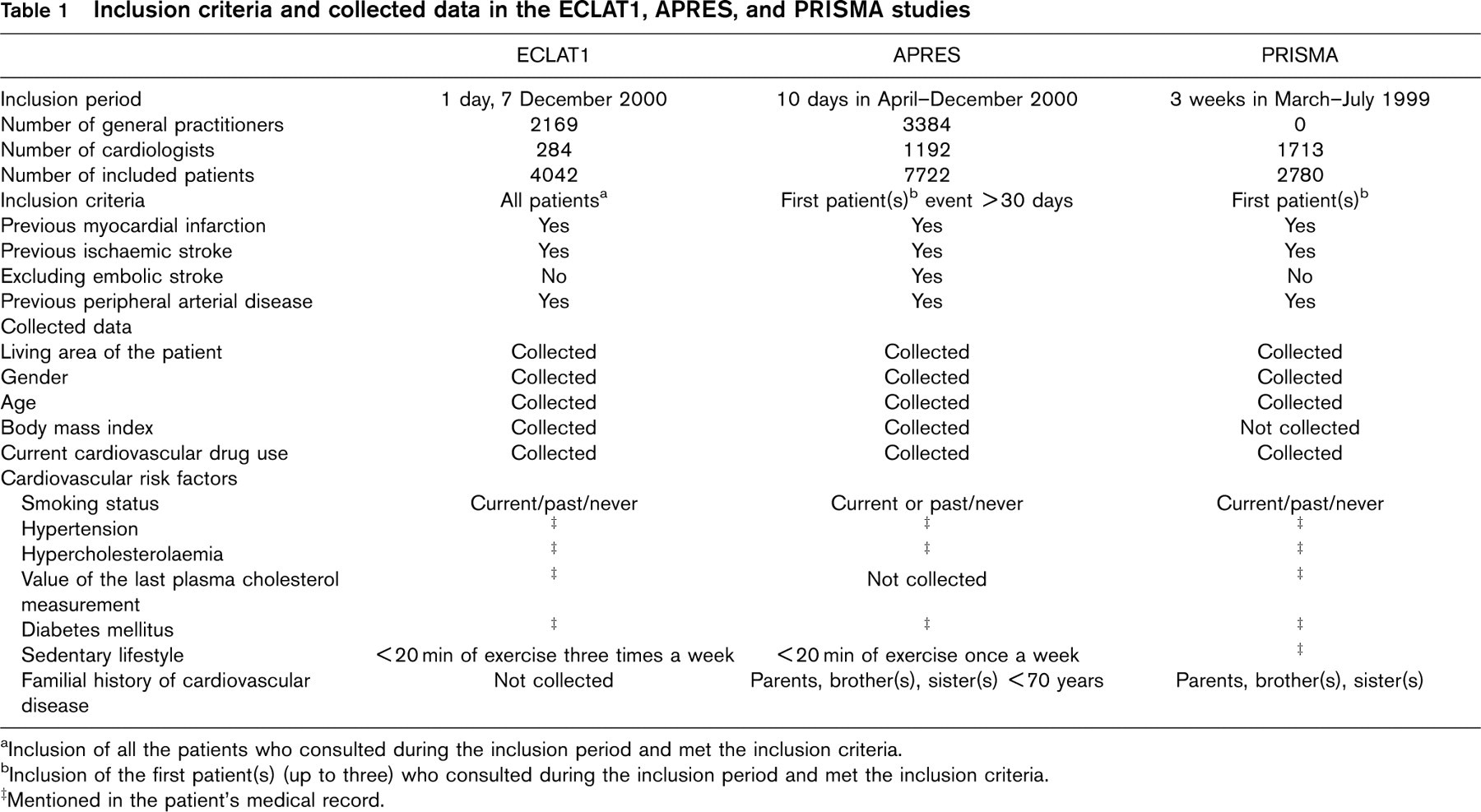
aInclusion of all the patients who consulted during the inclusion period and met the inclusion criteria.
bInclusion of the first patient(s) (up to three) who consulted during the inclusion period and met the inclusion criteria.
‡Mentioned in the patient's medical record.
Before data processing, variables were controlled by a scientific committee in order to look for conflicting data. These conflicting data were checked by enquiring at the physicians. Table 1 summarizes the number of participating physicians and selected patients, the inclusion criteria, and the collected data in the three studies.
Statistical analysis
The collected data were anonymously stored on computers and analysed on SAS statistical software (SAS Institute Inc., Cary, North Carolina, USA). Tests were considered as significant when the P-value was below 0.05. The χ2 test was used to compare the prevalence of cardiovascular risk factors and drug use according to the localization of the atherothrombotic disease (isolated MI, IS or PAD). Patients with multiple localizations were excluded from these analyses. When multiple omparisons were performed, a Bonferroni correction was applied to protect against inflation of the type I error rate. Similar comparisons were made according to the extent of the atherothrombotic disease (one, two or three arterial loci with atherothrombotic lesions) and a P-value for trend was calculated.
Multivariate logistic regression analyses were performed to assess whether the localization of the atherothrombotic disease (MI, IS or PAD, associated or not) was a significant determinant of the use of the major cardiovascular drug classes in secondary prevention [antiplatelet agents, statins, beta-blockers and angiotensin-converting enzyme (ACE) inhibitors]. The models were systematically adjusted for the living area of the patient, its gender and age, the study in which the patient was included (ECLAT1, APRES or PRISMA), and the specialization of the physician who did the inclusion (general practitioner or cardiologist). The determinants of the use of antiplatelet agents were analysed only in patients not taking anticoagulants, and the determinants of statin use, only in patients with a history of hypercholesterolaemia. As prescription rates could differ according to the presence of hypertension, the models assessing the determinants of the use of beta-blockers and ACE inhibitors were separately performed in hypertensive and non-hypertensive subjects. In addition to the covariates listed above, these models were also adjusted for heart failure and history of hypercholesterolaemia and diabetes.
Results
The sample was composed of 14544 patients: 14.1% lived in Ile de France (Paris area), 22.5% in north-western France, 14.4% in the north-east, 15.9% in the south-east, 19.6% in the south-west, and 13.5% in middle France. The number of patients with MI as the only prior atherothrombotic event was 5341 (36.7%). It was 3129 (21.5%) for IS, 3998 (27.5%) for PAD, 366 (2.5%) for the association MI plus IS, 1075 (7.4%) for MI plus PAD, 450 (3.1%) for IS plus PAD, and 185 (1.3%) for MI plus IS plus PAD. The main characteristics of the patients are summarized in Table 2, as well as the prevalence of cardiovascular drug use. Three-quarters of the sample were men, 31.0% of the patients were 75 years or older, 14.7% were obese (body mass index equal to or higher than 30 kg/m2), and the prevalence of smoking (current or past), hypertension, hypercholesterolaemia, and diabetes was 56.4, 60.1, 61.9 and 19.6%, respectively. At least one of these four major cardiovascular risk factors was observed in 94.3% of the patients, and more than two-thirds of the sample presented with two or more cardiovascular risk factors.
Characteristics of the patients and cardiovascular drug use in the sample
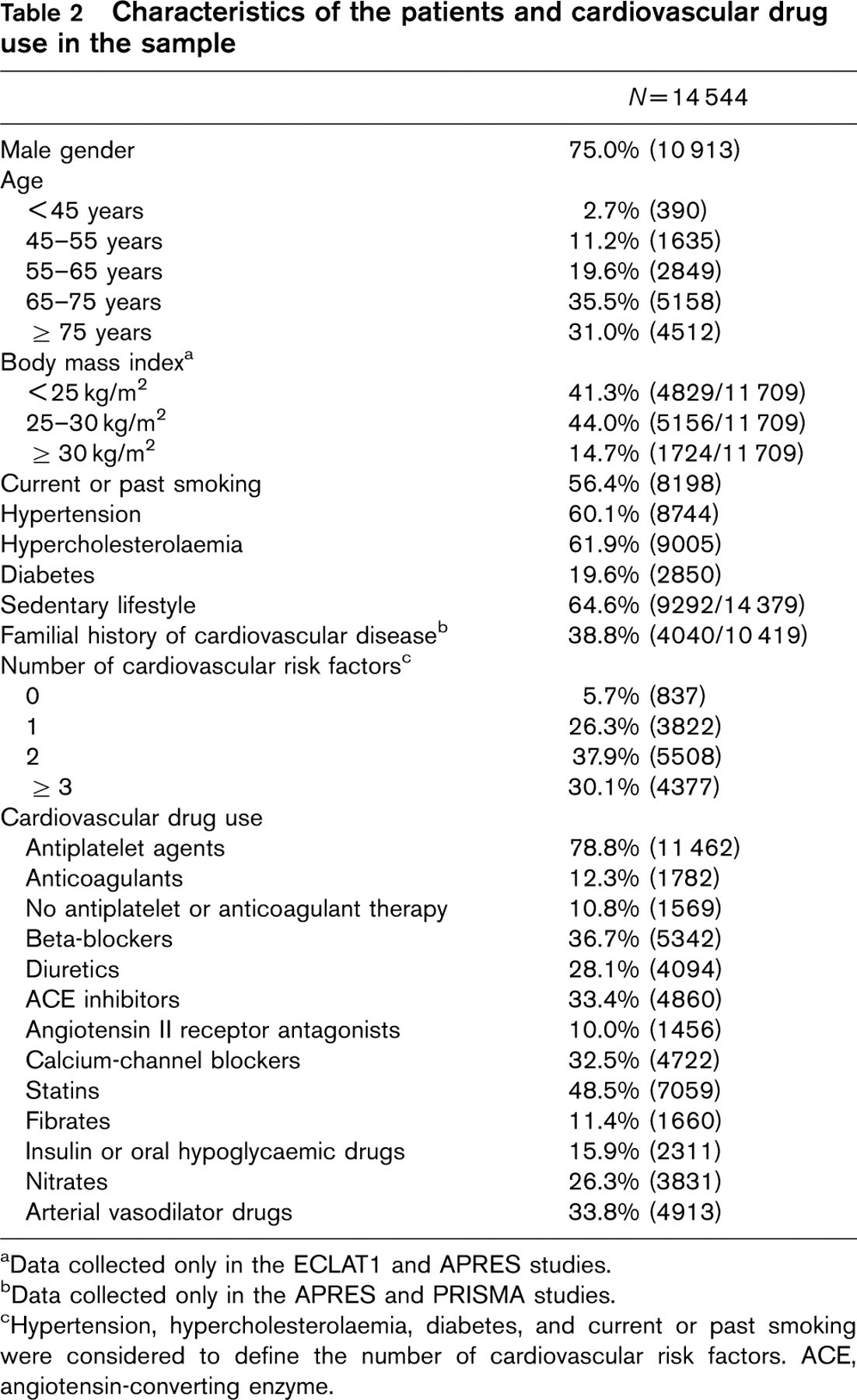
aData collected only in the ECLAT1 and APRES studies.
bData collected only in the APRES and PRISMA studies.
cHypertension, hypercholesterolaemia, diabetes, and current or past smoking were considered to define the number of cardiovascular risk factors. ACE, angiotensin-converting enzyme.
The prevalence of cardiovascular risk factors according to the extent and the localization of atherothrombotic disease is shown in Tables 3 and 4. There was a significant trend for an increase in the proportion of men and elderly subjects with the extent of the atherothrombotic disease (Table 3). The prevalence of smoking, hypertension, hypercholesterolaemia, diabetes, sedentary lifestyle, and familial history of cardiovascular disease also tended to significantly increase with the extent of the disease. The proportions of women, subjects aged 75 years or older, hypertension, and sedentary lifestyle were higher in patients who experienced an ischaemic stroke than in patients who suffered from a myocardial infarction or a peripheral arterial disease (Table 4). Myocardial infarction was associated with higher body mass indexes and higher prevalences of hypercholesterolaemia and familial history of cardiovascular disease, whereas smoking and diabetes were preferentially associated with peripheral arterial disease. The cluster of at least two cardiovascular risk factors was more frequent in patients with peripheral arterial disease than in patients with a prior myocardial infarction or ischaemic stroke. Data regarding the control of cardiovascular risk factors were collected only for hypercholesterolaemia, and the value of total cholesterol level was available for 37.0% of the hypercholesterolaemic subjects. Among these subjects, there was a higher proportion of controlled hypercholesterolaemic patients (last measurement of plasma total cholesterol below 5 mmol/l) in the group with myocardial infarction as compared with the group with ischaemic stroke (20.7 versus 9.3%, Bonferroni corrected P-value < 0.0001) and the group with peripheral arterial disease (20.7 versus 14.0%, P < 0.001).
Table 5 shows the prevalence of cardiovascular drug use according to the localization of the atherothrombotic disease. In multivariate logistic regression analysis, antiplatelet agents were taken to a greater extent in men than in women, and in patients with a history of myocardial infarction than in patients with a previous ischaemic stroke or peripheral arterial disease (Table 6). In hypercholesterolaemic subjects, male gender, age younger than 75 years, and history of myocardial infarction were independently associated with a higher probability to have statin therapy. Heart failure was a major determinant of the use of beta-blockers (a lower consumption in cases of heart failure) and ACE inhibitors (greater consumption in cases of heart failure) (Table 7). Hypercholesterolaemia was independently associated with a higher probability to take beta-blockers, and diabetes with a higher probability to take ACE inhibitors. A history of myocardial infarction was an independent determinant of a greater use of these two drug classes, in both hypertensive and non-hypertensive subjects. With the exception of ACE inhibitors, significant regional differences were observed in drug use between the Paris area and other parts of France (Tables 6 and 7).
Prevalence of cardiovascular risk factors according to the extent of the atherothrombotic disease

aχ2 test; P, probability for trend (≥ 75 versus < 75 years, for age; ≥ 30 versus < 30 kg/m2, for body mass index; ≥ 2 versus < 2 risk factors, for the number of risk factors); P 1, comparison between 1 and 2 loci; P 2, comparison between 1 and 3 loci; P 3, comparison between 2 and 3 loci; P 1, P 2, and P 3 are Bonferroni adjusted probabilities.
bData collected only in the ECLAT1 and APRES studies.
cData collected only in the APRES and PRISMA studies.
dHypertension, hypercholesterolaemia, diabetes, and current or past smoking were considered to define the number of cardiovascular risk factors. MI, myocardial infarction; IS, ischaemic stroke; PAD, peripheral arterial disease; NS, non-significant.
∗ P< 0.05;
∗∗ P< 0.01;
∗∗∗ P< 0.001.
Discussion
The pooling of the data from the ECLAT1, APRES and PRISMA studies has enabled the analysis of a huge sample of patients with a medical history of atherothrombotic disease. These subjects were recruited among patients consulting general practitioners or cardiologists, evenly distributed in France, and engaged in private practice, which is the most widespread practice among French physicians. A first important result is that 94.3% of the atherothrombotic patients presented with at least one of the four major cardiovascular risk factors: smoking, hypertension, hypercholesterolaemia or diabetes. This result is in accordance with the recently published data from Greenland et al. [9] and Khot et al. [10], assessing in broad populations that 80 to 90% of the subjects who develop a clinically significant coronary heart disease, and more than 95% who experience a fatal coronary event, have at least one the four major cardiovascular risk factors. Similarly, Emberson et al. [11] have shown, in more than 6000 middle-aged British men, that at least 80% of first major coronary heart disease events can be attributed to hypercholesterolaemia, hypertension or smoking. Our results add information to these data, pointing out that almost all the patients with a history of atherothrombotic event, whatever its localization, have at least one of the four conventional risk factors. This finding is in direct contrast with the frequent claim that only 50% of coronary heart disease is attributable to conventional risk factors. As already suggested by some authors [12], the four major cardiovascular risk factors can play a much greater role. Despite the indisputable need for additional research to establish the role of new cardiovascular risk markers, the control of conventional risk factors is essential to reduce the burden of cardiovascular disease in populations.
In the present analysis, the assessment of cardiovascular risk factors was based on the diagnosis of each patient's physician. We cannot exclude that this method of assessment may have brought heterogeneity in the identification of patients with cardiovascular risk factors. However, the prevalence rates of hypertension, hypercholesterolaemia, diabetes, and smoking were relatively close to those previously published in French samples of subjects with a history of coronary heart disease [13,14] or other atherothrombotic events [15].
Prevalence of cardiovascular risk factors according to the localization of the atherothrombotic disease (patients with multiple localizations are excluded)
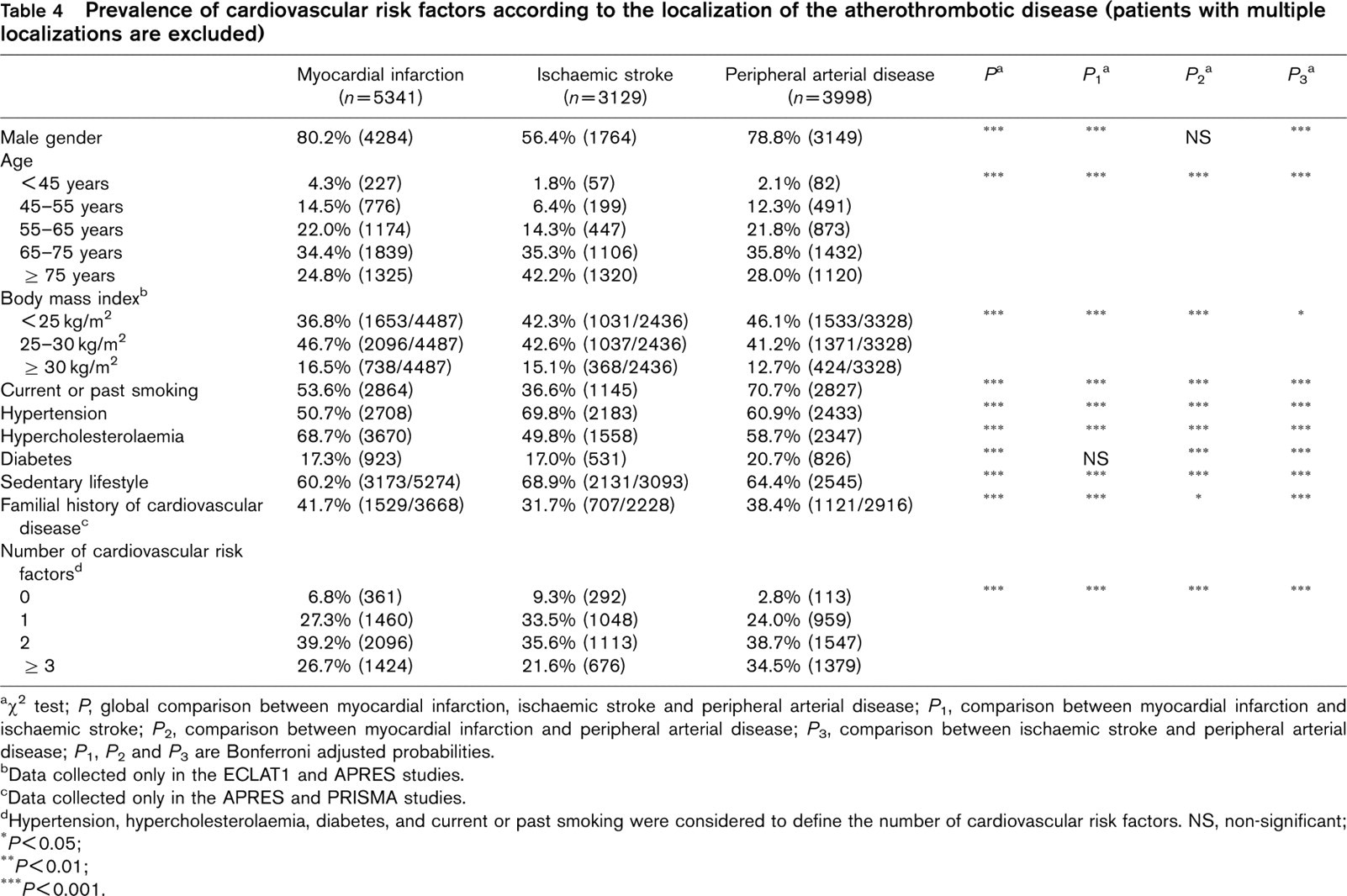
aχ2 test; P, global comparison between myocardial infarction, ischaemic stroke and peripheral arterial disease; P 1, comparison between myocardial infarction and ischaemic stroke; P 2, comparison between myocardial infarction and peripheral arterial disease; P 3, comparison between ischaemic stroke and peripheral arterial disease; P 1, P 2 and P 3 are Bonferroni adjusted probabilities.
bData collected only in the ECLAT1 and APRES studies.
cData collected only in the APRES and PRISMA studies.
dHypertension, hypercholesterolaemia, diabetes, and current or past smoking were considered to define the number of cardiovascular risk factors. NS, non-significant;
∗ P< 0.05;
∗∗ P< 0.01;
∗∗∗ P< 0.001.
Drug use according to the localization of the atherothrombotic disease (patients with multiple localizations are excluded)
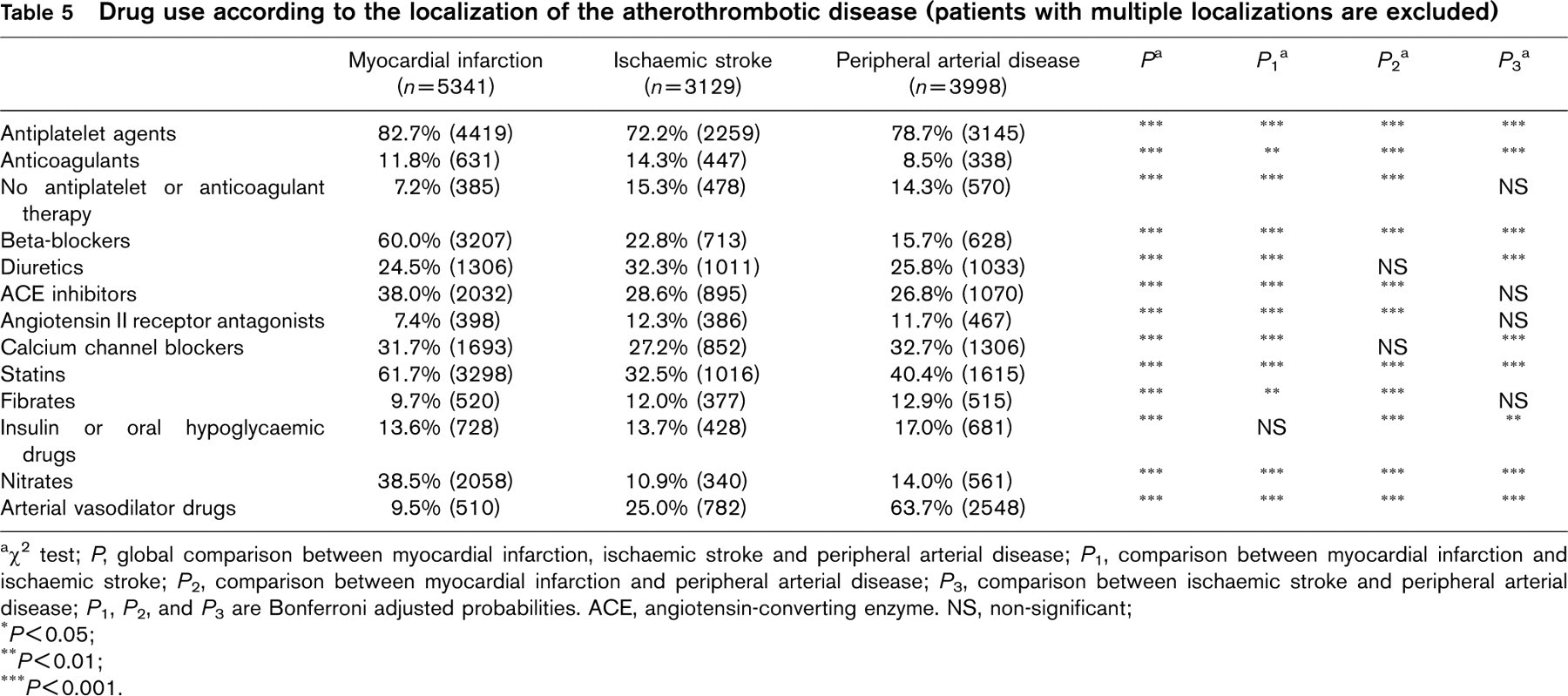
aχ2 test; P, global comparison between myocardial infarction, ischaemic stroke and peripheral arterial disease; P 1, comparison between myocardial infarction and ischaemic stroke; P 2, comparison between myocardial infarction and peripheral arterial disease; P 3, comparison between ischaemic stroke and peripheral arterial disease; P 1, P 2, and P 3 are Bonferroni adjusted probabilities. ACE, angiotensin-converting enzyme. NS, non-significant;
∗ P< 0.05;
∗∗ P< 0.01;
∗∗∗ P< 0.001.
The prevalences significantly differed according to the localization of the atherothrombotic disease: obesity, hypercholesterolaemia, and familial history of cardiovascular disease were preferentially associated with myocardial infarction, whereas smoking and diabetes were more frequent in patients with peripheral arterial disease, and male gender, old age, hypertension and sedentary lifestyle more frequent in patients with ischaemic stroke. Even after adjustment for age, the prevalence of male gender was lower in patients with stroke (data not shown), suggesting that gender may have played a role in the determination of the localization of the atherothrombotic disease in this sample.
Multivariate logistic regression analysis assessing the determinants of the use of antiplatelet agents and statins
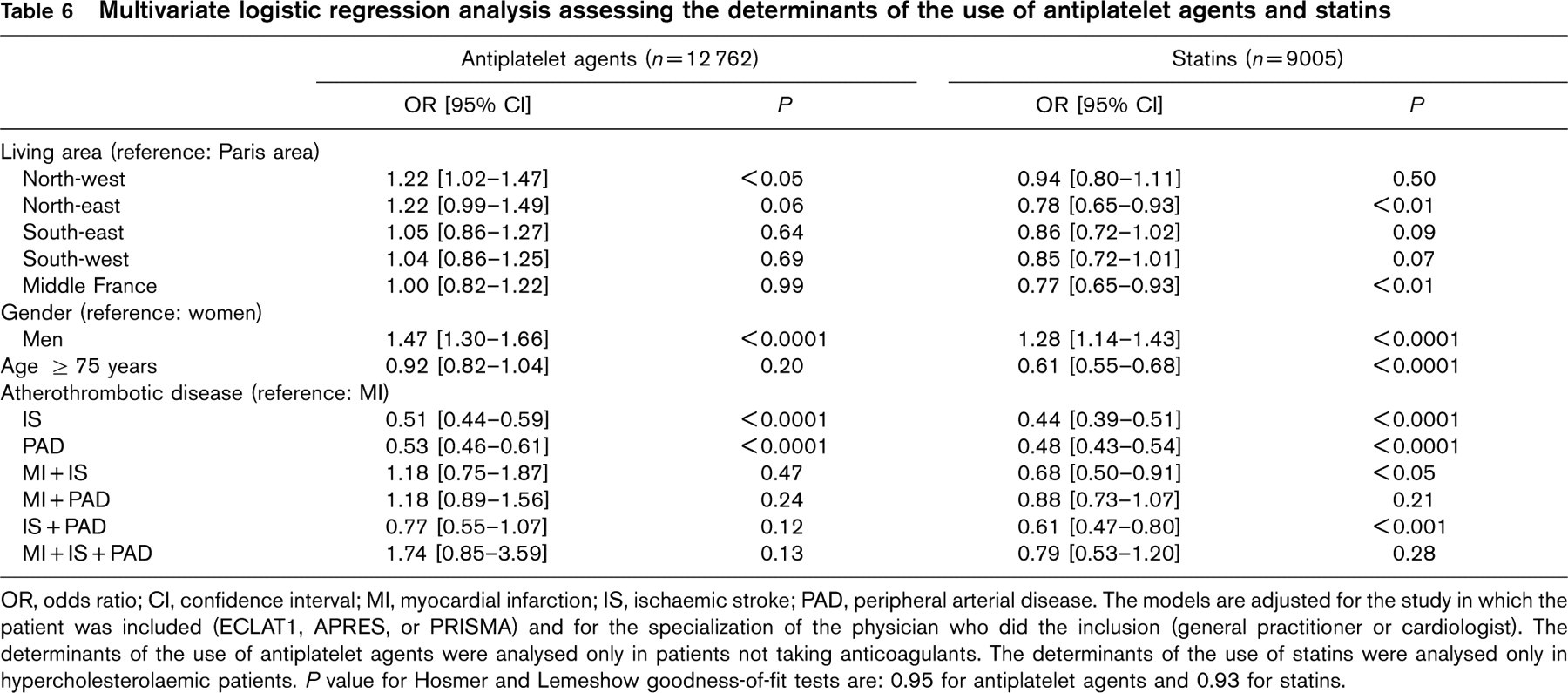
OR, odds ratio; CI, confidence interval; MI, myocardial infarction; IS, ischaemic stroke; PAD, peripheral arterial disease. The models are adjusted for the study in which the patient was included (ECLAT1, APRES, or PRISMA) and for the specialization of the physician who did the inclusion (general practitioner or cardiologist). The determinants of the use of antiplatelet agents were analysed only in patients not taking anticoagulants. The determinants of the use of statins were analysed only in hypercholesterolaemic patients. P value for Hosmer and Lemeshow goodness-of-fit tests are: 0.95 for antiplatelet agents and 0.93 for statins.
Multivariate logistic regression analysis assessing the determinants of the use of beta-blockers and ACE inhibitors
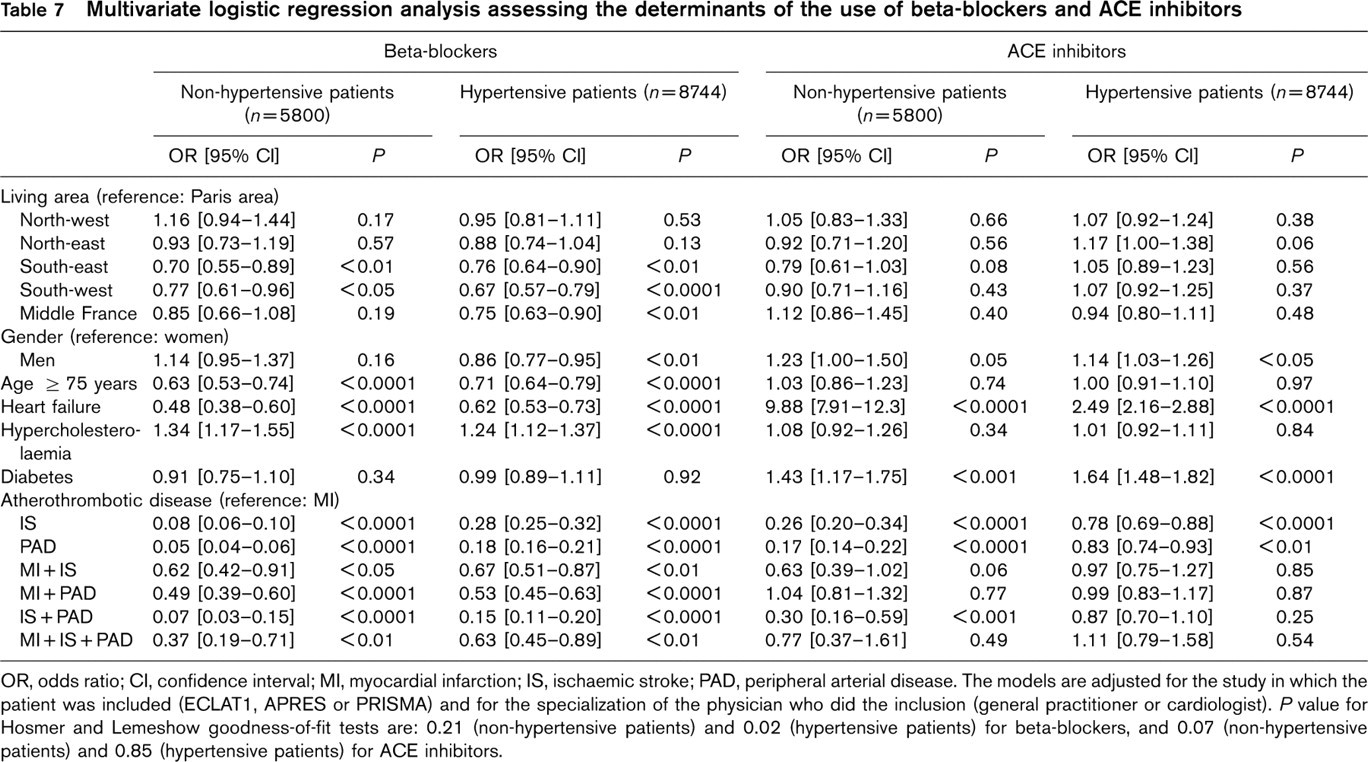
OR, odds ratio; CI, confidence interval; MI, myocardial infarction; IS, ischaemic stroke; PAD, peripheral arterial disease. The models are adjusted for the study in which the patient was included (ECLAT1, APRES or PRISMA) and for the specialization of the physician who did the inclusion (general practitioner or cardiologist). P value for Hosmer and Lemeshow goodness-of-fit tests are: 0.21 (non-hypertensive patients) and 0.02 (hypertensive patients) for beta-blockers, and 0.07 (non-hypertensive patients) and 0.85 (hypertensive patients) for ACE inhibitors.
Although the arterial impact of risk factors appears to be less or more pronounced according to the localization of the arteries in the body, atherothrombosis is a systemic disease and a global approach in the control of risk factors is required. In the present work, data on the control of risk factors were available only for hypercholesterolaemia. The results showed that the control of cholesterol level was more often achieved when hypercholesterolaemic subjects had a history of myocardial infarction. The analysis of drug prescriptions showed that differences in the control of cholesterol levels might be related to differences in statin prescription rates, which could probably be enhanced in certain subgroups of patients: women, elderly, and subjects with a history of stroke or peripheral arterial disease.
As expected, the prescription of antiplatelet agents was high in the sample, and most of the patients without antiplatelet therapy were taking anticoagulants. However, 10.8% of the subjects did not have any antiplatelet or anticoagulant therapy. This proportion was smaller in patients with a history of myocardial infarction (7.2%), whereas it was around 15% in subjects with a prior ischaemic stroke or peripheral arterial disease. In multivariate analysis, we studied the determinants of the use of antiplatelet agents only in subjects not taking anticoagulants, thus analysing factors associated with the absence of therapy acting on hemostasis. Female gender and history of stroke or peripheral arterial disease were independently associated with a lower probability to be treated with a hemostasis-modifying drug. As antiplatelet agents can be beneficial to patients at risk of atherothrombotic events, including subjects with myocardial infarction, stable angina, stroke, transient ischaemic attack, or intermittent claudication [16], this therapy should be prescribed whatever the localization of the disease.
Beta-blockers can prevent the recurrence of events in patients with myocardial infarction [17]. In high-risk subjects [i.e. one or more cardiac risk factor(s) and a dobutamine echocardiography test positive for ischaemia], bisoprolol reduces the risk of cardiac death and myocardial infarction [18]. Moreover, there is now evidence that beta-blockers improve survival and cardiovascular risk in patients with heart failure [19–23. According to all these data, beta-blockers could be beneficial to a wide range of patients. However, in our study, the probability to be treated with a beta-blocker when myocardial infarction was not the sole prior atherothrombotic event, or when heart failure was associated with the atherothrombotic disease, was extremely low. In patients with heart failure, this can be explained by the fact that most of the studies on this topic were not published when we recruited subjects [20–23. The low prescription rate in patients with multiple prior atherothrombotic events may reflect the fact that beta-blockers are often considered as relatively contraindicated in peripheral arterial disease, because of vasoconstrictor properties. However, a meta-analysis of trials on patients with mild-to-moderate peripheral arterial disease found no worsening of walking capacity or symptoms of intermittent claudication with beta-blockers [24]. Furthermore, recent data have shown no significant difference in skin microcirculation before and after withdrawal of beta-blocking therapy in hypertensive patients with peripheral arterial disease (intermittent claudication or ischaemic rest pain) [25]. Therefore, a history of peripheral arterial disease should not prevent the use of beta-blockers in patients for whom these drugs could improve the cardiovascular prognosis.
In the present study, the determinants of the use of ACE inhibitors were first represented by heart failure, both in patients with and without hypertension, with of course, a greater use of ACE inhibitors in case of heart failure. Prescription of ACE inhibitors was also guided by a previous history of myocardial infarction or diabetes, two medical conditions whose prognosis can be improved by this class of drug [26–29. Recent studies have shown that the prescription of ACE inhibitors could be extended to a large proportion of patients at risk of atherothrombotic complications, including subjects with a history of ischaemic stroke and peripheral arterial disease [29,30].
The present data have identified various determinants of drug use. First, regional differences in the use of secondary preventive drugs were pointed out. Despite efforts to homogenize the health care system in France, differences in medical practice still remain. Causes for such differences can be multiple and additional research is required to clearly identify these causes. Second, prescriptions of secondary preventive drugs appeared to be guided mainly by the indications and contra-indications of the drugs, but prescription rates were systematically higher in subjects with a history of isolated myocardial infarction, suggesting a non-optimal use of antiplatelet agents, statins, beta-blockers, and ACE inhibitors in patients with a history of ischaemic stroke, peripheral arterial disease, or multiple atherothrombotic events. However, these findings should be carefully interpreted as our data were collected between 1999 and 2000; that is to say before or immediately after the publication of the randomized controlled trials that have assessed the effectiveness of statins, irrespectively of baseline plasma cholesterol levels, in patients who suffered from stroke or peripheral arterial disease [31,32], or the effectiveness of ACE inhibitors in similar patients [29,30]. Before these trials, little was known about the effectiveness of these drugs in patients who had a cerebrovascular or peripheral arterial disease but did not suffer from coronary artery disease. The EURO-ASPIRE [33], PREVESE [34], USIC and PREVENIR [35] surveys on secondary prevention after myocardial infarction have all shown that the use of preventive drugs in coronary patients has progressively increased during the past few years, along with results of randomized controlled trials and changes in guidelines. Similarly, future prescriptions of secondary preventive drugs should also increase in patients with a history of stroke, peripheral arterial disease or multiple prior atherothrombotic events.
The strength of the present study lies in the size of the sample, and in the analysis of various localizations of the atherothrombotic disease, not only myocardial infarction. Its limitation is that the control of risk factors could not be fully evaluated. Furthermore, since the sample was recruited within patients of general practitioners and cardiologists in private practice, the results cannot be totally extrapolated to all the patients with atherothrombotic disease. Prescription rates of the major secondary preventive drugs appear to be systematically higher in subjects with a history of isolated myocardial infarction than in patients with a previous stroke or peripheral arterial disease, or with multiple prior atherothrombotic events. There is potential for enhancement of drug prescriptions in these latter patients, accordingly to the results of several recent randomized controlled trials. Prescriptions are too frequently based on unproven contraindications instead of being guided by evidence-based medicine that demonstrates the usefulness of secondary preventive drugs, whatever the localization of the atherothrombotic disease.