
Abstract
Background
Design
Method
Results
Conclusion
Introduction
Coronary heart disease (CHD) is ubiquitous in large areas of the world, beginning insidiously, progressing with age, and ultimately, affects one in two men and one in three women in Western populations [1]. The clinical presentation of CHD varies substantially, however, from chronic conditions such as angina pectoris or heart failure to acute coronary syndromes or sudden death. Although atherosclerosis of the coronary arteries is the common denominator in all these conditions, the pathophysiologic processes are different. The natural history of angina pectoris and of other clinical manifestations of the arteriosclerotic plaque has been extensively described [2–8]. The predominant distinguishing feature separating acute coronary syndromes from chronic angina is plaque rupture with subsequent formation of thrombosis [7, 9–12]. The pathophysiology of plaque rupture has been extensively examined and cigarette smoking, hemodynamic factors, inflammatory cell activity, and disturbed fibrinolysis have been linked to disruption and thrombosis [9–12]. Patients with chronic stable angina have been demonstrated to have more stenotic lesions than patients with acute myocardial infarction (AMI) [2–4, 12, 13], suggesting that these two manifestations of coronary atherosclerosis develop in different ways.
Coronary artery bypass grafting (CABG) is a procedure which is usually undertaken because of extensive coronary heart disease, whereas AMI may occur in patients with moderate or even minimal disease [14]. Thus, CABG without prior AMI may serve as a marker for generalized obstructive lesions whereas a first AMI is a marker of a condition ensuing from plaque rupture. Few studies have assessed whether the risk factors for chronic stable angina are similar to those predicting AMI. One study [15] did not find any major differences between the two, with the exception of proinsulin levels and blood pressure, which predicted AMI but not stable angina. In this analysis we used CABG without prior AMI as a model for chronic angina and compared them with patients with AMI in order to assess possible differences in risk factor pattern.
Participants and methods
Study population
Data were derived from 7434 participating men free from prior AMI or stroke from the intervention group in the multifactor Primary Prevention Study that began in Göteborg, Sweden in 1970 [16]. All men in the city who were born between 1915 and 1925 (n = 30 000), except those born in 1923, were randomized into three groups of 10 000 men each. The men in one of the groups (intervention group; n = 9998; participants 7495 (75%)) were offered a screening examination to identify and treat risk factors. A second examination was done in 1974 to 1977, and a third in a 20% sub-sample in 1980. The intervention was essentially a high-risk strategy directed towards men with pronounced hypercholesterolemia, severe hypertension, or heavy smoking habits, according to predefined criteria with treatment for hypertension, hyperlipidemia or smoking offered at specialist clinics [16]. Outcome and risk factor pattern after 12 years were found to be similar in the intervention and control groups [16] and hence we consider the intervention group to be reasonably representative of the background population in the city. All participants gave their informed consent to participate in the study. The study was approved by the Ethics Committee for Medical Research at Göteborg University.
Information on smoking habits, physical activity during leisure time, treatment for hypertension, diabetes, psychological stress, myocardial infarction and stroke, and family history of AMI were collected via a postal questionnaire to all men in the investigated group. Men who returned the questionnaire were invited to a clinical examination. Men who did not return the questionnaire were sent one reminder but after this no further action was taken. The screening examinations were performed in the afternoon. Blood pressure was measured after 5 min rest with the subject seated. Body mass index (BMI) was calculated as weight per square metre. BMI was classified into six categories < 20, 20–22.5, 22.5–25.0, 25.0–27.5, 27.5–30.0 and > 30.0 kg/height2. Smoking habits were coded as never smoked, former smoker of more than 1 month's duration, smoking 1-14 g of tobacco per day, smoking 15-24 g and smoking 25 g or more per day. One cigarette was considered to contain 1 g of tobacco, a cigarillo 2 g and a cigar 5 g of tobacco. Serum cholesterol concentrations were determined in blood samples taken after fasting for at least 2 h according to standard laboratory procedures [17]. Physical activity during leisure time was categorized into four levels with 1 representing sedentary activity, 2 moderate activity such as walking or light gardening during at least 4 h per week, and 3 regular, strenuous, or 4 very strenuous activities. Because there were few men in category 4, the two highest categories were combined. Psychological stress was assessed by way of one single question in the postal questionnaire and rated from 1 to 6, with 5 and 6 defined as permanent stress during the last year, or the last 5 years, before the examination, respectively [18].
Follow-up procedures
All participants in the multifactor Primary Prevention study were followed from the date of their baseline examination until 31 December 1998, by running the data file of the men in the study against the Swedish national register on cause of death and the Swedish Hospital Discharge Register. This process was approved by the review board of the Göteborg University Ethics Committee. The Hospital Discharge register has been in operation since 1970 and has operated on a nationwide basis only since 1987. All discharges from Sahlgrenska Hospital, however, which was the single major hospital in the city until 1977, and also the only hospital in the region with heart surgery, have been entered in the national register since 1970 but all years (except 1976 due to a legislative change for that single year), and all discharges from Östra Hospital, the other major hospital of the city, that opened in 1978, were entered from the start [19]. In addition, until March 1983, all fatal and non-fatal myocardial infarctions fulfilling predefined criteria occurring in the study population were recorded in the Göteborg AMI Register [20].
For the purpose of these analyses, cases of AMI and of men undergoing CABG without prior AMI were identified. AMI was defined as a discharge, or death with International Classification of Diseases (ICD) 410 (ICD 8 until 1986, ICD 9 until 1996) or I21 (ICD 10) as a principal diagnosis. Fatal cases were defined as AMI if the underlying cause of death was 410-414 (ICD 8 and 9) or I21-I25 (ICD10). To identify cases of aorto-coronary bypass operations classification codes 3066, 3067 and 3091 were used prior to 1997 and FNA and FNC during 1997 and 1998. Codes for coronary angioplasty were not registered for the purpose of the present study. Forty-six men undergoing CABG in connection with an operation for aortic stenosis were excluded, leaving 146 men who had undergone CABG, 1664 men with AMI and 5578 men without evidence of CHD during follow-up; altogether 7388 men, for analysis. Of the men with AMI, 198 subsequently underwent CABG; they were categorized among the AMI group.
Statistical methods
SAS software statistical package (version 8e; SAS Institute, Cary, North Carolina, USA) were used for all analyses. Means were calculated with standard methods. To evaluate risk over time Cox proportional hazard ratios, with 95% confidence interval were calculated. The risk over time was adjusted for all variables significantly associated with AMI in univariate analysis. Age, serum cholesterol, body mass index, and systolic blood pressure were entered as continuous variables, whereas smoking was entered with five levels, physical activity with three, and stress as permanent versus all other, and family history, treatment for hypertension and diabetes as yes/no variables. To estimate the differences in association between the risk factors for AMI and CABG a multiple logistic regression analysis for the two diagnoses, AMI and CABG, was used in a generalized logit model. According to this we modeled the logits of three category's response variables (no risk, AMI and CABG) against the risk factors. In this model, age-adjusted odds ratios are obtained for the two separate outcomes, and then compared to see whether they are significantly different.
Results
Men who underwent CABG without previous AMI had the highest mean total serum cholesterol 7.04 (SD 1.21) mmol/l, followed by men with AMI or who died from CHD, 6.72 (SD 1.23), whereas men with no CHD had a mean baseline level of 6.36 (SD 1.12) (Table 1). BMI differed only marginally between the groups. Men with coronary disease had higher mean systolic and diastolic blood pressure than men who remained free of CHD but there were no differences between the AMI and the CABG groups.
Baseline characteristics by diagnosis during follow-up

CHD, coronary heart disease; MI, myocardial infarction; CABG, coronary artery bypass grafting; BMI, body mass index.
Even within the comparatively narrow age span of the men in the study, the risk of AMI increased sharply with age (Table 2). In contrast, older men were less likely to undergo CABG. Family history of CHD, serum cholesterol, hypertension and diabetes predicted both AMI and CABG, whereas high BMI, low physical activity and psychological stress were significantly associated only with AMI. Even light to moderate smoking (1-14 g/day) was associated with increased risk of AMI, hazard ratio 1.70 (1.50–1.94); whereas only very heavy smokers were more likely to undergo CABG, hazard ratio for 25 g/day or more 2.19 (1.02–4.66). Serum cholesterol was a stronger predictor of CABG than of AMI. Compared to men with serum cholesterol of 5.0 or lower, men with serum cholesterol 5.1–6.4, 6.5–7.4 and over 7.4 mmol/l had adjusted hazard ratios of 1.22 (1.00–1.49), 1.66 (1.352.03) and 2.04 (1.65–2.51) for AMI. Corresponding hazard ratios for CABG were 1.57 (0.66–3.70), 3.44 (1.47–8.03) and 5.21 (2.20–12.31) after adjustment for age and other factors.
An increase in serum cholesterol of 1 mmol/l was associated with an odds ratio of 1.56 for CABG but only 1.30 for AMI (Table 3). These odds ratios were statistically different (P = 0.004). Likewise, there were significant differences in the effect of age (P < 0.001) smoking (P < 0.0001) and of a family history of AMI, with the latter being more strongly related to CABG than to AMI (P = 0.013). There were no differences in the odds ratios for systolic or diastolic blood pressure, or diabetes. BMI, stress and physical activity were significant predictors for AMI, but not for CABG.
Discussion
We found that, whereas most coronary risk factors by and large predicted both AMI and CABG, serum cholesterol was a stronger predictor of CABG than of AMI. Smoking was a weaker risk factor for CABG than for AMI, with no discernible increase in risk except in very heavy smokers. In addition, family history of AMI was a stronger predictor of CABG than of AMI.
Hazard ratios and observation year associated with cardiovascular risk factors for acute myocardial infarction and for coronary artery bypass grafting without prior acute myocardial infarction during follow-up
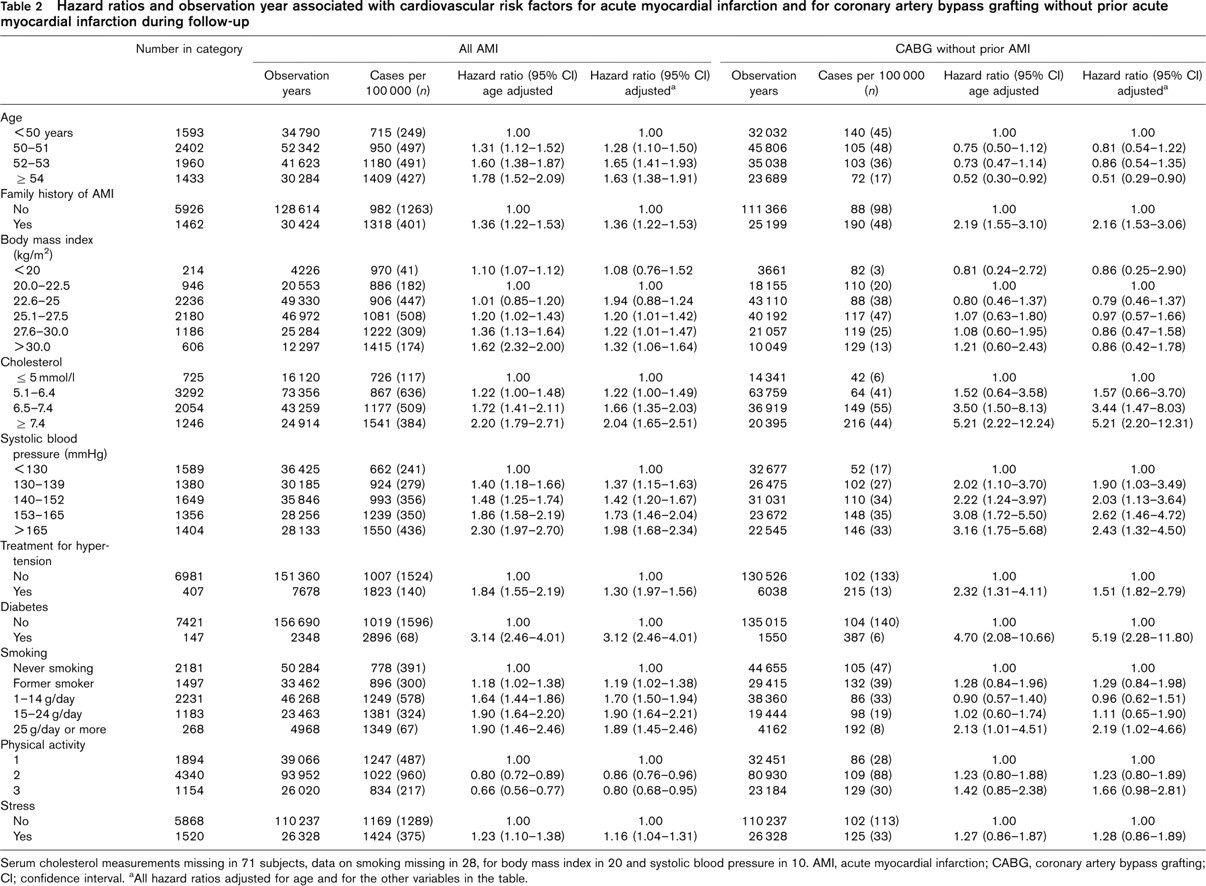
Serum cholesterol measurements missing in 71 subjects, data on smoking missing in 28, for body mass index in 20 and systolic blood pressure in 10. AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; CI; confidence interval. aAll hazard ratios adjusted for age and for the other variables in the table.
Analysis of odds ratios and the differences between the subjects with acute myocardial infarction and subjects who underwent coronary artery bypass grafting without a previous acute myocardial infarction
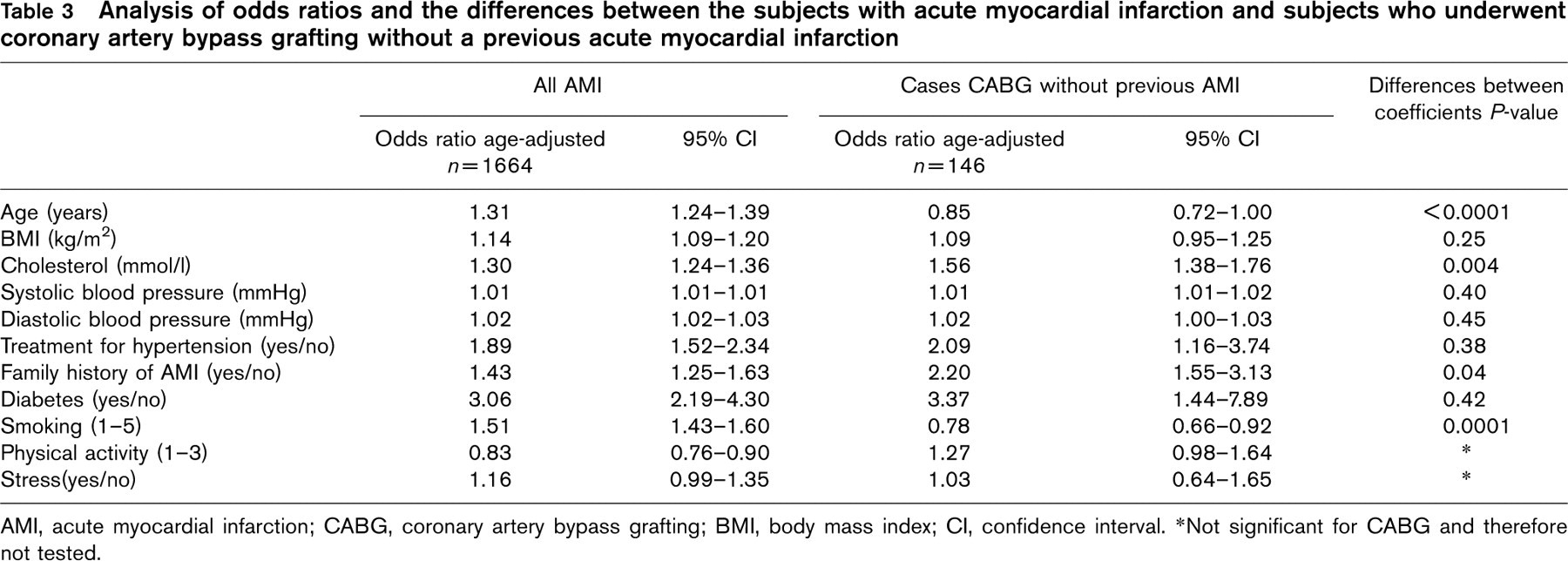
AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; BMI, body mass index; CI, confidence interval. ∗Not significant for CABG and therefore not tested.
These findings could be relevant both to differences in pathophysiology, and to potential changes in the clinical expression of the disease over time. We know that lifetime risk of coronary heart disease and elevated serum cholesterol are strongly linked [20] and that low-density lipoprotein accumulates over time in the artery wall [21]. Patients with chronic stable angina have been demonstrated to have more stenotic lesions than patients with AMI [2–4, 13]. Possibly, our finding of a stronger correlation between CABG and elevated levels of serum cholesterol than between AMI and cholesterol could be due to more extensive coronary lesions in the former, secondary to more widespread lipid deposits, but not necessarily a more pronounced tendency to plaque rupture. Conversely, the stronger relation between AMI and smoking may be due to a stronger link between smoking and coagulation factors, because the precipitating event in AMI is usually a plaque rupture, with ensuing thrombosis.
The finding that family history of AMI was more strongly linked to CABG than to AMI is unexpected but could be mediated through familial influences on serum cholesterol level [22, 23]. The fact that the CABG patients were more physically active than the AMI patients is probably because physical activity will have provoked more symptoms. Hypertension and diabetes were equally strongly associated with both AMI and CABG.
Even within the comparatively narrow age span of the men in the study, the risk of AMI increased sharply with age (Table 2). In contrast, older men were less likely to undergo CABG. It is probably partly an effect of thoracic surgeons being less disposed to let older patients undergo CABG, with the assumption of more postoperative complications and multiple diseases in the elderly [24, 25]. During the almost 30-year follow-up of the study, coronary surgery expanded rapidly, but this will mainly have benefited the younger men of the study. By the mid-1990s, the older men of the study were approaching 80 years.
This study has several limitations. First, only men of a comparatively limited age span were studied which means that the findings may not be generalizable to younger men, to women and to the present era when indications for surgery will have changed and percutaneous interventions have emerged as a major procedure in coronary disease. Second, we did not have angiographic data in any patient group so the assumption that the men undergoing CABG had more extensive disease is not firmly supported. Possibly, they were only more symptomatic, and there was probably a major overlap between the groups with respect to the extensiveness of their lesions. This, however, would probably have decreased the chances of detecting differences in the effect of the risk factors. Third, patients with mild angina who did not undergo CABG were not studied. CABG as an outcome may also be related to other factors than atherosclerosis such as availability of resources, local practices and severity of symptoms. In a prior analysis of this study population 128 men developed symptoms of angina with no prior AMI over the first 4 years of follow-up [26]. In multivariate analysis neither serum cholesterol nor smoking predicted angina but these findings may not be strictly relevant to the present analysis, where the men were much older. Lastly, many CHD drug treatments have a substantial effect on the measured outcomes that may differ systematically between groups.
The strengths of the study are the comparatively large number of endpoints and that we were able to follow the patients through official hospital registers. The hospital discharge diagnosis of AMI forms the basis of the Swedish AMI register which has been validated and examination of medical records for a national sample of ischemic heart disease patients suggested a high sensitivity (94%) and a high positive predictive value (86%) for ICD-9 code 410 in hospital discharge data with regard to definite AMI [19].
Coronary bypass surgery is only performed in five centers in Sweden, all of which were linked to the national Hospital Discharge register for practically all years of follow-up. Thus, only very few cases, if any, will have been missed. All CABG operation codes for the men in the study were accompanied by diagnoses of ischemic heart disease [27].
In conclusion, this paper indicates that serum cholesterol appears to be a stronger predictor for future CABG than for AMI, whereas smoking is not associated with future CABG, except in very heavy smokers, indicating that different risk factors are not related in the same way to different expressions of the disease. Both smoking rates and mean levels of cholesterol have declined in the Swedish population but other populations display other patterns [28]. Notably, a decreasing prevalence of angina pectoris in the Swedish population has been described [29]. When risk factor patterns change the clinical expression of the disease may also change.