
Abstract
Background
Heart rate recovery (HRR) is a marker of vagal tone that is a powerful predictor of mortality in patients with coronary artery disease.
Design
This study aims at evaluating the effects of long-term exercise training on HRR after acute myocardial infarction (AMI), in order to clarify whether prolonged exercise training could maintain a long-term improvement of HRR.
Methods
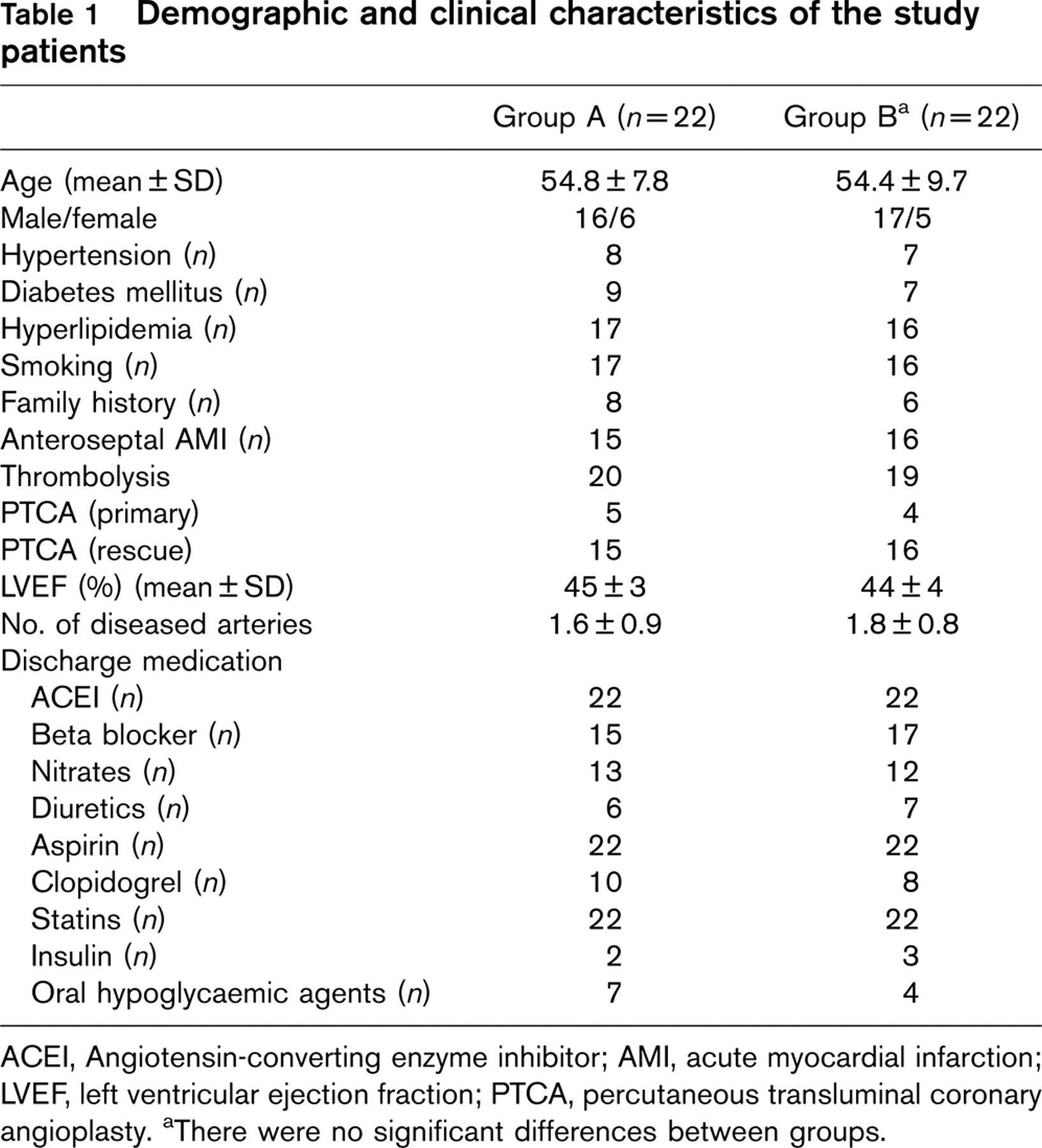
Forty-four patients after AMI were enrolled in a 3-month hospital-based exercise training programme. At the end, patients were subdivided into two groups: group A (n = 22), patients discharged with a specific home-based exercise training programme and instructions for improving leisure-time physical activity; group B (n = 22), patients discharged with generic instructions to maintain physical activity. All patients underwent a cardiopulmonary exercise test before, at the end of 3 months exercise training and at 6 months follow-up.
Results
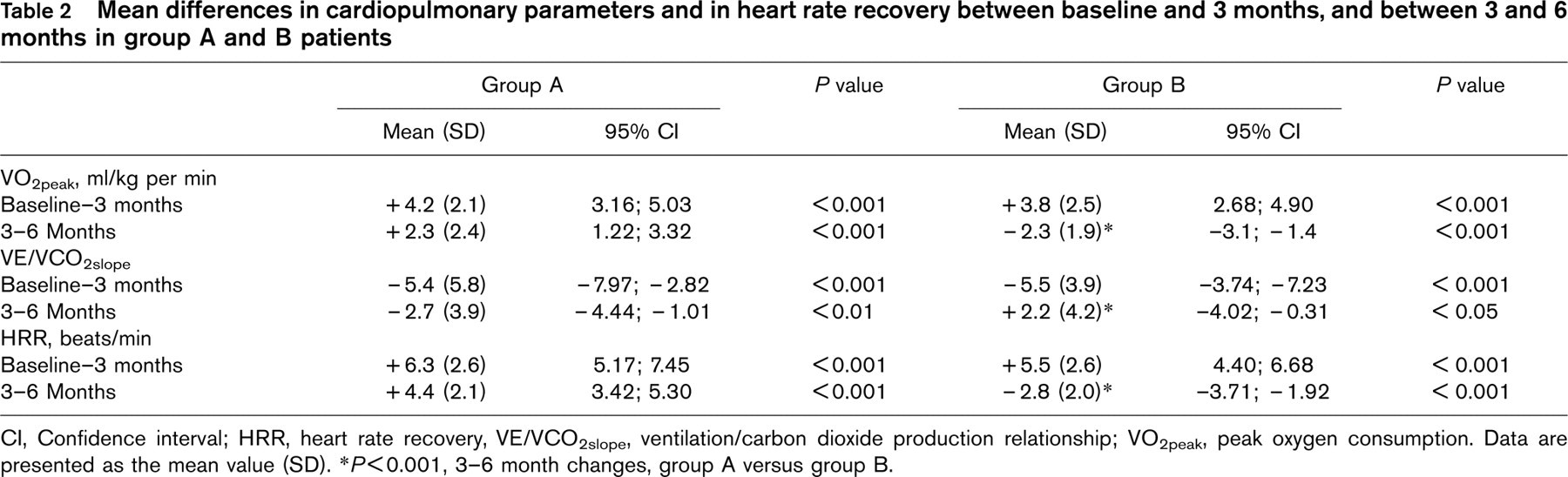
At the end of the hospital-based exercise training programme we observed an increase in peak oxygen consumption [VO2peak; from 13.9 ± 3.6 to 18 ± 2.7 ml/kg per min (A) and from 14.1 ± 3.9 to 17.9 ± 2.1 ml/kg per min (B), P<0.001] and in HRR [from 17.1 ± 1.8 to 23.4 ± 1.4 beats/min (A), and from 18.8 ± 2.1 to 24.3 ± 1.9 beats/min (B), P<0.001]. At 6 months’ follow-up we observed a further improvement in VO2peak (from 18.0 ± 2.7 to 20.3 ± 2.7 ml/kg per min, P<0.001) and in HRR (from 23.4 ± 1.4 to 27.8 ± 2.1 beats/min, P<0.001) in group A, but a significant decrease in VO2peak and in HRR in group B (P<0.001).
Conclusion
Long-term exercise training is useful for maintaining or improving the beneficial results of the standard 3-month exercise training programme on cardiovascular capacity and HRR. This observation may bear beneficial prognostic effects on patients after AMI.
Introduction
The major causes of death are cardiovascular diseases (CVDs) in the developed nations [1]. In the USA alone, cardiovascular diseases accounted for 51% of all deaths [2]. In Sub-Saharan Africa (SSA), CVD is not yet a leading killer but the trend is changing, particularly in urban areas [3, 4]. This is because of economic transition, urbanization, industrialization and globalization, which bring about lifestyle changes that promote heart diseases. These lifestyle changes include: tobacco use, a sedentary lifestyle, unhealthy diet, high blood pressure, obesity, diabetes mellitus and family history [5, 6].
A review of the global trends in CVD over the last century and the emerging evidence of adverse trends in CVD risk factors and mortality from SSA provide compelling evidence for concern [7, 8]. Cardiovascular diseases will undoubtedly increase in frequency in SSA over the coming decades as many countries are now undergoing a rapid transition. For example, in Nigeria (a country with a population of 125 million), approximately 35% of the population is now urbanized [9]. The need for capacity building and exploration for policy, system, and environmental changes that can be incorporated into a population-based approach to CVD prevention in Africa has been stressed [3, 10, 11]. Reports about cardiovascular risk in relation to CVD are limited in this environment. Some secondary data from the developed nations that have been extrapolated for local use either underestimate or overestimate the level of CVDs in Africa.
However, most developing nations lack objective data to quantify the level of CVD. Thus, the aim of this study was to carry out an assessment of cardiovascular risk for members of staff and students of Obafemi Awolowo University, Ile-Ife. A few cases of sudden death resulting from heart attacks among the students and staff served as an impetus for this study. Furthermore, the proliferation of ‘Tokunbo’ cars (imported used cars) and ‘Okada’ (commercial motorbikes) in the campus brought about a change from an active lifestyle to a sedentary lifestyle for the people in this community. In 1999, the democratic government increased the minimum wage of workers across the nation. With this increase, many workers could afford to own used cars through loans. Information from the security records at the institution showed that the number of registered car users within the campus had increased by 71% in the last 3 years. Furthermore, the establishment of the British Tobacco Company in Ibadan (about 60km from the campus) may increase the number of tobacco smokers and passive smokers in this community. The change to a sedentary lifestyle may have significant effects on the cardiovascular system. It is not known what effects these changes might have had on the cardiovascular risk of people in this community.
Methodology
Subjects
The study was carried out within the Obafemi Awolowo University community; 600 volunteers (students and the members of staff) were recruited for the study (300 males and 300 females). The subjects were divided into three groups. Two hundred were members of senior staff cadre; two hundred junior staff cadre and two hundred undergraduate students. Senior staff were either academic staff or non-academic staff that had a salary scale of grade level 7 and above. Junior staff were those non-academic staff whose salary scales were grade level 6 and below. The university is believed to be one of the most beautiful campuses in Africa. It is situated in the ancient city of Ile-Ife, in south-west Nigeria and has a population of over 50 000 people.
Questionnaire
The questionnaire used to obtain information in this study was adapted from the study by Blessey [5]. The questionnaire sought relevant information on age, sex, smoking habit, blood pressure, weight, height, stress, exercise history, diet, personal medical history and cholesterol count. The questionnaire was tested in a pilot study with 33 students prior to the main study. Based on their responses and the level of understanding of the questions in the questionnaire, some ambiguous or unclear questions were restructured or modified. Scores were assigned to each answer based on the scoring design in the original questionnaire. For example, male sex is scored as one, and female sex scored as zero; age ≤ 56 (1) and 55 years or below (0). Family history and personal history are the areas that had the highest scores; for subjects having relatives who had a heart attack or stroke before the age of 60, a score of 12 was given and for subjects who had had a heart attack or heart or vessel surgery, a score of 20 was given.
For each respondent, the scores were summed to obtain an overall risk score. The scores related to cholesterol were removed from final analysis, because the majority of the respondents did not know their cholesterol counts. However, the section on diet was used as a substitute for cholesterol count. The questionnaire was easy to administer because the respondents were drawn from the academic community, with the majority being familiar with the health information asked for in the questionnaire. The average score for high risk was estimated to be 36 and above. Medium risk was between 19 and 35, and low risk, 18 and below.
Procedure
Data was collected during working hours (1000–1500 h). The researchers interacted with each respondent and their physical characteristics (height and weight) measured. After about 10 min of quiet sitting, the blood pressure was measured using an electronic blood pressure monitor (Omron Healthcare Inc., Vernon Hills, Illinois, USA). In the pilot study, good agreement was found between the readings from the automatic device and measurements taken with a conventional sphygmomanometer.
Data analyses
One-way analysis of variance (ANOVA) was used to compare the risk among the students, junior staff and senior staff. Post hoc least significant difference was used to determine the direction of the significance. Student's t-test was used to compare the risk between the male and female subjects.
Results
A summary of the physical characteristics of the subjects is presented in Table 1. The risk scores calculated for each of the three groups are shown in Table 2. Of the students, 87% were found to be of low risk, while 13% were of medium cardiovascular risk.
Of the junior staff, 84% were found to be in the low risk category and 20% at medium risk. No one from these groups was found to be in the high-risk category.
The result of the one-way ANOVA comparing the risk scores among the three groups of subjects showed that there was a statistically significant difference within the three groups (F = 2.452; P <0.004; df = 2599). The least significant difference (LSD) post hoc analysis revealed no difference between the junior and senior staff; or between the students and junior staff. However, the senior staff had a significantly higher cardiovascular risk than the students (P <0.05). The t-test analysis revealed no significant difference in the risk of score between females and males (P > 0.05).
Physical characteristic of the subjects and calculated risk scores
Risk scores calculated for the all the subjects
Cardiovascular risk factor analysis (subsection)
The subsections relating to smoking, diet, exercise and stress were extracted from the data and analyzed separately. The results showed that the subjects’ rate of smoking cigarettes was low and they consumed less food that contained cholesterol. On average, the subjects engaged in moderate physical activities, but the levels of stress were high (Table 3).
Discussion
We found the majority of the subjects in this study were in the low cardiovascular risk category. This was anticipated, since the sample population had better educational awareness and access to improved health care delivery than those in the rural areas. On the other hand we felt that the sedentary lifestyle of these people in an urban area might be a factor that may increase the level of risk. The World Health Organization (WHO) reports that only in the African region is CVD not already the leading cause of death [10]. Several reports confirm the rarity of ischaemic heart disease in Africa [12, 13]. Mensah [3] observed recently that some population groups in SSA have already made the epidemiological transition to non-communicable diseases (NCDs) including CVDs at a much faster rate than ever witnessed in other regions of the world. He warns that, if targeted interventions are not put in place to prevent the development of CVD risk factors in SSA, the public health picture at 2020 and beyond may appear no different to what is seen in the rest of the world today. Factors such as socio-economic status (SES) might be responsible for the low risk recorded in this study. The majority of the subjects fall into the middle socioeconomic status. Rutledge et al. [4] reported that low SES was associated with cardiovascular disease risk factors, including higher body mass index, waist-hip ratios, cigarette smoking, low reported activity levels and a greater probability of hypertension. In this study we found the rate of smoking to be low and the subjects to be moderately physically active.
No statistically significant difference was found between the levels of risk between males and females in this study. Males naturally tend to drink alcohol and smoke cigarettes more than females. The gap between the level of risk for men and that of women developing and dying from CVD has become smaller in recent years. This may be as a result of the increase in the number of women smokers [3, 12, 13]. Peterson et al. [1] reported that CVD is the leading cause of death in women in most industrialized countries accounting for over 40% of deaths in women at all ages in Britain. The number of women suffering with and dying from CVD was found to be similar to that of men [14]. The occurrence of CVD rises rapidly in women after the age of 60, but little is known about the distribution of CVD, risk factors, and their control in older women [15].
In this study, senior staff were found to have a significantly higher risk of developing CVD than the students. The active lifestyle of the students compared with that of the senior staff may account for this difference. Students are more active in sports and are younger in age. Cardiovascular risk has been found to be greater among the elderly [3]. Sedentary lifestyle is a very strong risk factor for cardiovascular disease. The more activity, the greater the level of protection from cardiovascular disease. A change from a sedentary to an active lifestyle can reduce the CVD risk by about 33% [16].
The findings of this study have potential implications. A routine assessment of cardiovascular risk could help to detect persons that are at increased risk of cardiovascular disease. Thus, preventive measures could be put in place to reduce the risk. This study has provided a baseline assessment of risk in a selected academic population from which further studies could be made. There is a need to reproduce this study among rural dwellers for the purpose of comparison with the results of this study. However, it may not be easy to use this questionnaire in the rural communities since the majority are illiterate. Based upon the outcomes of this study, the cardiovascular risk-factor analysis questionnaire appears feasible for the evaluation of risk of cardiovascular disease among the Nigerian University community.