
Abstract
Background
Patients with manifest vascular disease are at high risk of a new vascular event or death. Modification of classical risk factors is often not successful. We determined whether the extra care of a nurse practitioner could be beneficial to the cardiovascular risk profile of high-risk patients.
Design
We conducted a randomized, controlled trial based on the Zelen design.
Methods
Two hundred and thirty-six patients with manifestations of a vascular disease and who had two or more modifiable vascular risk factors were pre-randomized to receive treatment by a nurse practitioner plus usual care or usual care alone. After 1 year, risk factors were remeasured. The primary endpoint was achievement of treatment goals for blood pressure, lipid, glucose and homocysteine levels, body mass index, and smoking.
Results
Of the pre-randomized patients, 95 of 119 (80%) in the intervention group and 80 of 117 (68%) in the control group participated in the study. After a mean follow-up of 14 months, the patients in the intervention group achieved significantly more treatment goals than did the patients in the control group (systolic blood pressure 63 versus 37%, total cholesterol 79 versus 61%, low density lipoprotein-cholesterol 88 versus 67%, and body mass index 38 versus 24%). Medication use was increased in both groups and no differences were found in patients' quality of life (SF-36) at follow-up.
Conclusion
Treatment delivered by nurse practitioners, in addition to a vascular risk factor screening and prevention program, resulted in a better management of vascular risk factors than usual care alone in vascular patients after 1-year follow-up.
Introduction
Cardiovascular disease (CVD) is the most common cause of morbidity and mortality in Western countries [1]. It is the result of atherosclerosis and is influenced by multiple risk factors, such as smoking, obesity, physical inactivity, hypertension, dyslipidemia, and diabetes. Patients with manifest vascular diseases are at a considerably increased risk of fatal and non-fatal events at the same or another location in the vascular tree [2]. Modification of classical risk factors is known to reduce the risk of vascular events [3], yet despite this, vascular risk factors are often poorly managed. Secondary prevention care improved only slightly in Europe between 1996/1997 and 1999/2000 [4–6], and many patients are not treated at all or have not reached treatment goals for hypertension or dyslipidemia. Physicians adhere poorly to CVD prevention guidelines for several reasons, such as lack of time and difficulty determining which of several treatment guidelines is best [7]. Physicians have also indicated that it is the patient him or herself that forms the greatest barrier to adequate CVD prevention [8]. Lifestyle changes are an important component of vascular risk reduction strategies, and not all physicians have enough time or the appropriate training to advise about lifestyle changes (e.g. quit smoking, weight loss, increased consumption of fruit and vegetables, increased physical activity, decreased intake of salt and saturated fats) [7]. New strategies, such as organizational changes or specialist healthcare, need to be developed to achieve better risk factor management in high-risk patients. Nurse practitioners have the skills in medical and behavioral sciences needed for successful risk management [9]. A number of randomized controlled trials have shown that nurse practitioner-guided treatment for patients with coronary heart disease (CHD) results in better risk factor management than achieved with usual care [10–20]. Most of these trials, however, were conducted in a primary care setting, whereas high-risk patients are often treated in the hospital, where medical specialists are responsible for risk factor management. We investigated in the multidisciplinary Vascular Prevention by Nurses Study (VENUS) whether risk factor management in the hospital improved with nurse practitioner care plus usual care compared with usual care. Beforehand, all patients underwent an institutionalized vascular screening.
Methods
Study design
Patients were randomized before informed consent was obtained, according to the Zelen design [21], to either nurse practitioner care plus usual care (intervention group) or usual care alone (control group). Randomization was carried out by telephone with a computer-generated list. Within 24 h, a research nurse mailed patients information about the treatment they would receive. Informed consent was obtained immediately from the patients in the intervention group and after 6 months from the patients in the control group.
We aimed to detect a 20% difference between the two groups in achievement of treatment goals (hypertension, dyslipidemia) at follow-up. With a power of 80% (β = 0.2) and an α value of 0.05, 79 patients were needed in each group. To allow for dropouts, we decided to enroll 236 patients; the estimated study duration was 18 months.
Study population
Dutch-speaking patients between 18 and 79 years referred to University Medical Center Utrecht (UMC Utrecht), The Netherlands, with symptomatic manifestations of transient ischemic attack, stroke, aortic abdominal aneurysm (AAA) or peripheral artery disease (PAD) are routinely offered a vascular screening and prevention program (described below). Patients were eligible for VENUS when two or more of the following modifiable vascular risk factors were detected: smoking, hypertension, dyslipidaemia, diabetes mellitus, obesity, or hyperhomocysteinaemia. Patients with a life expectancy shorter than 2 years, those with terminal malignant disease and those dependent in daily activities (Rankin grade > 3) [22] were excluded. The Ethics Committee of our institution approved the study. Before participating in the VENUS study, patients underwent a vascular screening program. This institutionalized screening program is offered to patients with recently diagnosed vascular diseases or severe risk factors and is part of regular care. The program is supported by the departments of Internal Medicine, Nephrology, Vascular Surgery, Neurology, Radiology, Cardiology, and Epidemiology at the UMC Utrecht. Patients are screened for vascular risk factors and for asymptomatic arterial disease. Height and weight were measured without shoes and heavy clothing. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. Blood pressure was measured two times in a sitting position at the right and left upper arm with a non-random sphygmomanometer. Medical history, current use of medication, current and past smoking behavior and current and past alcohol use were derived from a standardized questionnaire described elsewhere [23]. Fasting blood was sampled to determine serum glucose, total cholesterol, high-density lipoprotein (HDL)-cholesterol, triglycerides, and homocysteine levels. Low-density lipoprotein (LDL)-cholesterol was calculated with Friedewald's formula. A multidisciplinary team of specialists formulated treatment recommendations (such as repeat measurement, start medication, adapt current medication, stop smoking, or change lifestyle) for the management of individual risk factors or vascular disorders. The results and the treatment recommendations were reported in writing to the treating vascular specialist and the general practitioner (GP) approximately 1 month before the start of VENUS. This procedure was identical in the control as in the intervention group and further action was left to the discretion of the treating physicians. The results of the vascular screening were considered as baseline measurements in the VENUS study.
The intervention group
Patients assigned to the intervention group were invited by a nurse practitioner to attend the risk-factor management clinic. At the first visit, patients were told about their vascular risk factors and individualized, realistic goals were set in co-operation with the patients. Action plans were made for lifestyle changes: smoking cessation, regular exercise, healthy diets, and medical treatment of risk factors (antiplatelet agents, blood pressure, lipid, and glucose-lowering agents, or folic acid). These action plans were created to raise awareness and motivation because the goals were attainable. A study physician prescribed or changed medication because a nurse practitioner in The Netherlands is formally not allowed to do this. At subsequent visits the nurse practitioner provided support, encouragement and reassurance in changing or maintaining the desired lifestyle and in their adherence to the prescribed medication. The nurse practitioner interventions were based on written protocols for each vascular risk factor. The length and frequency of the visits were determined by the needs of patients and nurse practitioner in order to achieve the individual treatment goals. The nurse practitioner documented for each patient the applied interventions and visit duration.
The control group
Patients assigned to the control group received care provided by the GP and the treating vascular specialist (in this study a vascular surgeon or neurologist).
Treatment goals
The formulated treatment recommendation and the nurse intervention of the VENUS study are based on international guidelines for the treatment of vascular risk factors. According to guidelines at the time of the start of the study, the following goals were set: total cholesterol < 5.0 mmol/l, LDL-cholesterol ≤ 3.1 mmol/l, triglycerides < 1.7 mmol/l, HDL-cholesterol for men > 1.0 mmol/l and women > 1.3 mmol/l [24], blood pressure < 140/90 mmHg [25], fasting glucose < 6.1 mmol/l [26], homocysteine for men < 11.3 μmol/l and women < 9.4 μmol/l [27, 28], BMI < 25kg/m2 [29], and complete smoking cessation [30, 31].
Follow-up
Follow-up visits were at 6 months and 1 year after randomization. In this article, we provide data of the 1-year follow-up only. At both follow-up evaluations, data were collected on current medication use and smoking behavior. The vascular risk factor levels were again determined by physical examination and a fasting blood sample. Quality of life was assessed by the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) [32].
Outcome assessment
The primary outcome was the cardiovascular risk profile at 1 year after randomization. We measured change in risk factors and medication usage. The proportion of achieved treatment goals for each risk factor before and after the intervention was compared for the intervention and the control group.
Data analysis
All comparisons between groups were performed according to the intention-to-treat principle. The data for patients who withdrew their consent before the beginning of the randomized controlled trial (n = 61) or who were lost to follow-up (n = 10) were not analyzed. Continuous variables are presented as means with standard deviation and categorical variables as percentages. Differences between the groups were tested by the independent sample t-test for continuous variables and the χ2 test for categorical variables; the corresponding 95% confidence intervals (CIs) are reported. Changes within each group were assessed by paired sample t-test. The association between the proportion of treatment goals achieved and treatment arm was determined with logistic regression and adjusted for the baseline values of the vascular risk factors. Analyses were performed in SPSS version 12.0.1 (SPSS, Chicago, Illinois, USA).
Results
Patient flow and follow-up
Two hundred and thirty-six consecutive patients were recruited and randomized in the study between May 2002 and October 2003 (Fig. 1). During this time, 61 patients refused to participate, eight died (four in each group), one moved abroad and one developed severe pulmonary disease and was not able to continue the study. One patient was crossed over from the control to the intervention group. Hence, the main analyses were based, without those lost to follow-up, on data from 90 (76%) of the 119 patients in the intervention group and 75 (64%) of the 117 control patients. Follow-up ended on 27 December 2004. The mean follow-up was 14 months (range, 10–22 months); 14 months (range, 10–22 months) for the intervention group and 14 months (range, 12–23 months) for the control group.
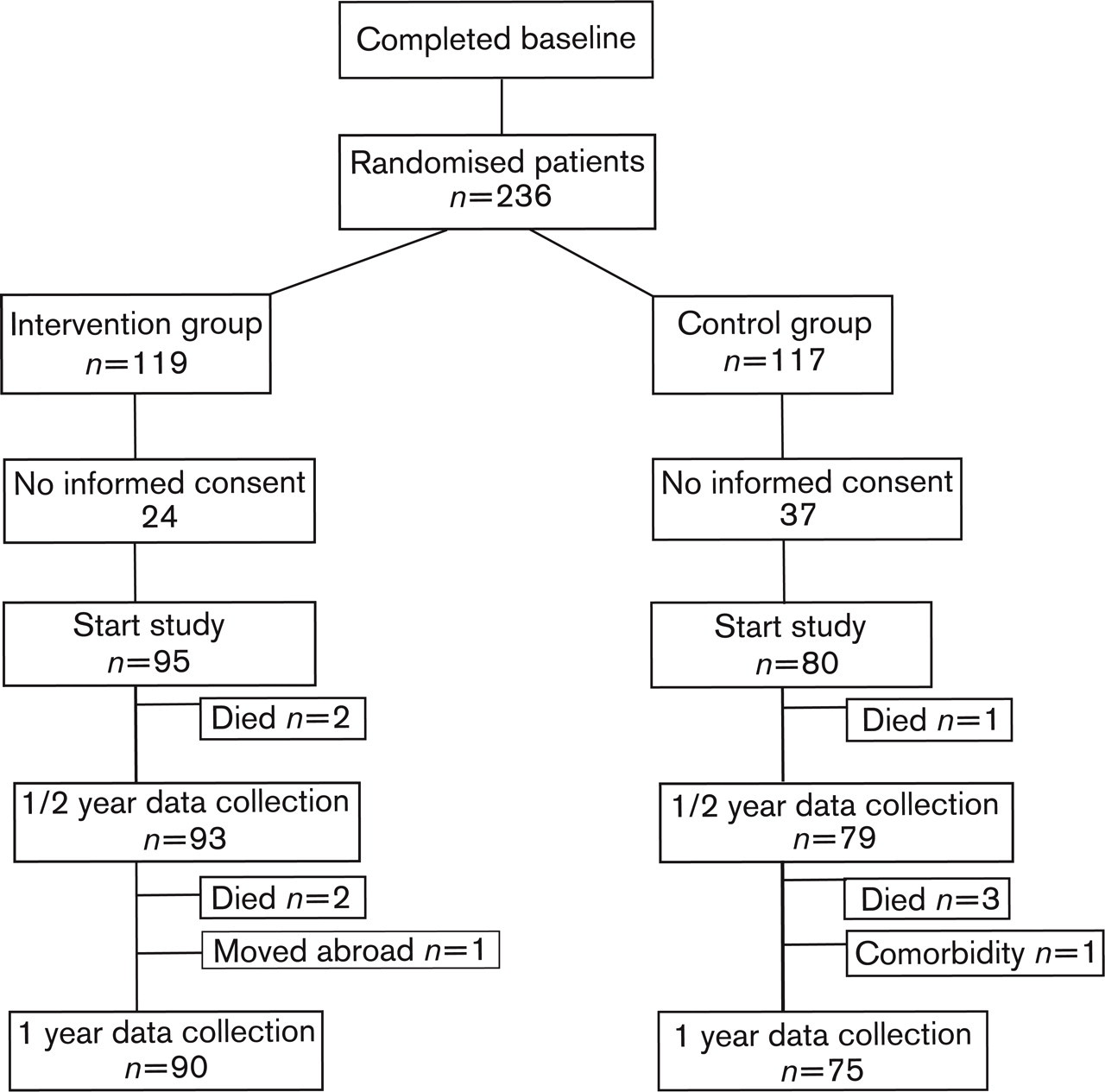
Flow of patients through the trial.
Randomization was considered successful because the two groups were not different with respect to important risk factors (Table 1). Of the total study population, 77% was male, with a mean age of 60.1 ± 10.3 years. Patients assigned to the intervention group more often had PAD, CHD, and cerebrovascular disease in history than those in the control group. Medication use was similar in the two groups at baseline, with most patients using antiplatelet therapy, blood pressure and lipid-lowering agents. There were no conspicuous differences between the baseline characteristics of the patients who did or did not participate in the study (Table 2).
The mean values for the different vascular risk factors at baseline and at 1 year are shown in Table 3. The intervention group achieved a mean reduction in total cholesterol of 0.9 mmol/l (95% CI 0.7–1.1) compared to 0.5 mmol/l (95% CI 0.3–0.7) in the control group. For systolic blood pressure, the intervention group achieved a mean reduction of 8 mmHg (95% CI 5–13) compared to 6 mmHg (95% CI 2–11) in the control group. Diastolic blood pressure, LDL-cholesterol, and glucose levels improved (P < 0.001) from baseline to 1 year in each group. The levels of triglycerides decreased 0.4 mmol/l (95% CI 0.2–0.5) and homocysteine decreased 2.4 μmol/l (95% CI 1.4–3.1) in the intervention group but not in the control group. The mean BMI increased 0.7 kg/m2 (95% CI 0.4–1.0) in the control group after 1 year. The prevalence of smoking increased in both groups.
Baseline characteristics of the randomized patients
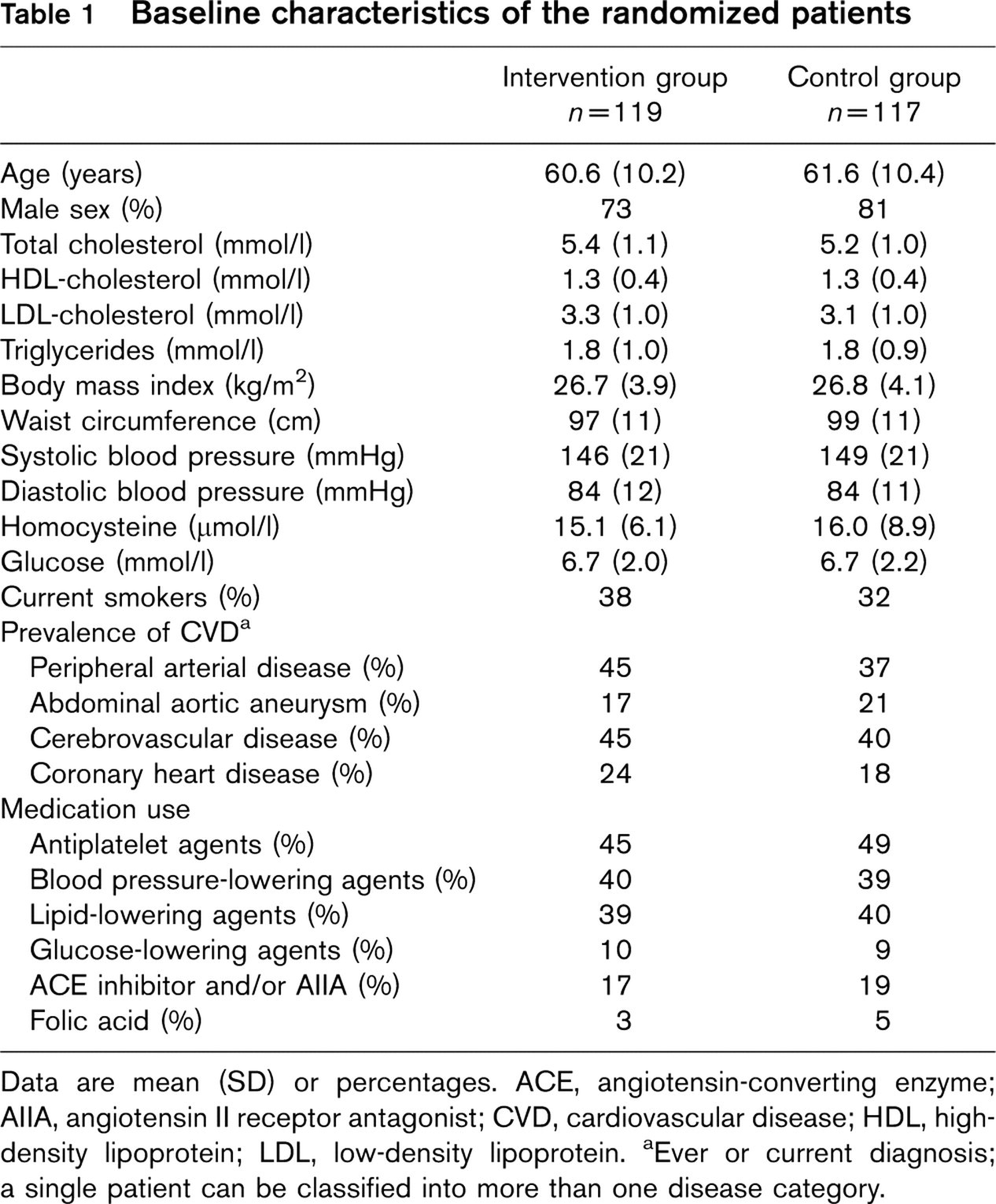
Data are mean (SD) or percentages. ACE, angiotensin-converting enzyme; AIIA, angiotensin II receptor antagonist; CVD, cardiovascular disease; HDL, highdensity lipoprotein; LDL, low-density lipoprotein.
aEver or current diagnosis; a single patient can be classified into more than one disease category.
Baseline characteristics of participants versus non-participants
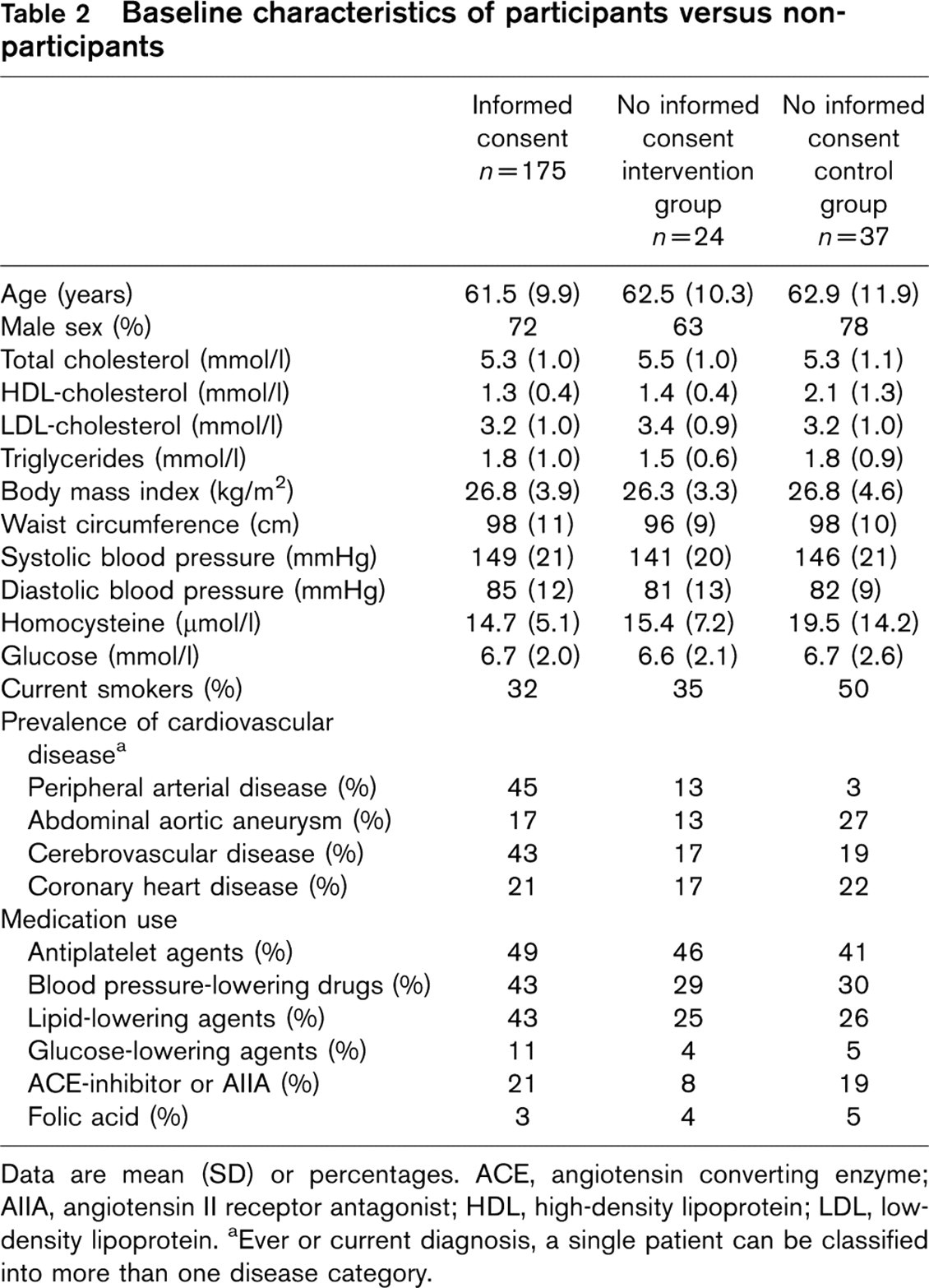
Data are mean (SD) or percentages. ACE, angiotensin converting enzyme; AIIA, angiotensin II receptor antagonist; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
aEver or current diagnosis, a single patient can be classified into more than one disease category.
The levels of total cholesterol decreased 0.4 mmol/l (95% CI 0.1–0.7), LDL-cholesterol 0.4 mmol/l (95% CI 0.1–0.7), triglycerides 0.3 mmol/l (95% CI 0.1–0.5) and homocysteine 1.9μmol/l (95% CI 0.6–3.3) more in the intervention group and HDL-cholesterol increased −0.1 mmol/l (95% CI −0.2 to −0.0) more in the intervention group.
The proportion of patients who had already reached their target for individual risk factors at baseline or who achieved treatment goals after 1 year, separated per group, is shown in Table 4. More patients in the intervention group than in the control group achieved their treatment goals at follow-up. After adjustment for the baseline values, the proportion of patients who achieved treatment goals for systolic blood pressure (odds ratio (OR) 2.7; 1.3–5.4), total cholesterol (OR 3.3; 1.5–7.3), LDL-cholesterol (OR 3.5; 1.5–8.6) and BMI (OR 4.0; 1.2–13.1) was significantly higher in the intervention group than in the control group. Indicating that patients in the intervention group more often achieved treatment goals for systolic blood pressure than patients in the control group, taking the baseline blood pressure into account.
Changes in risk factors and differences between the change in the intervention and the control group (n = 165)
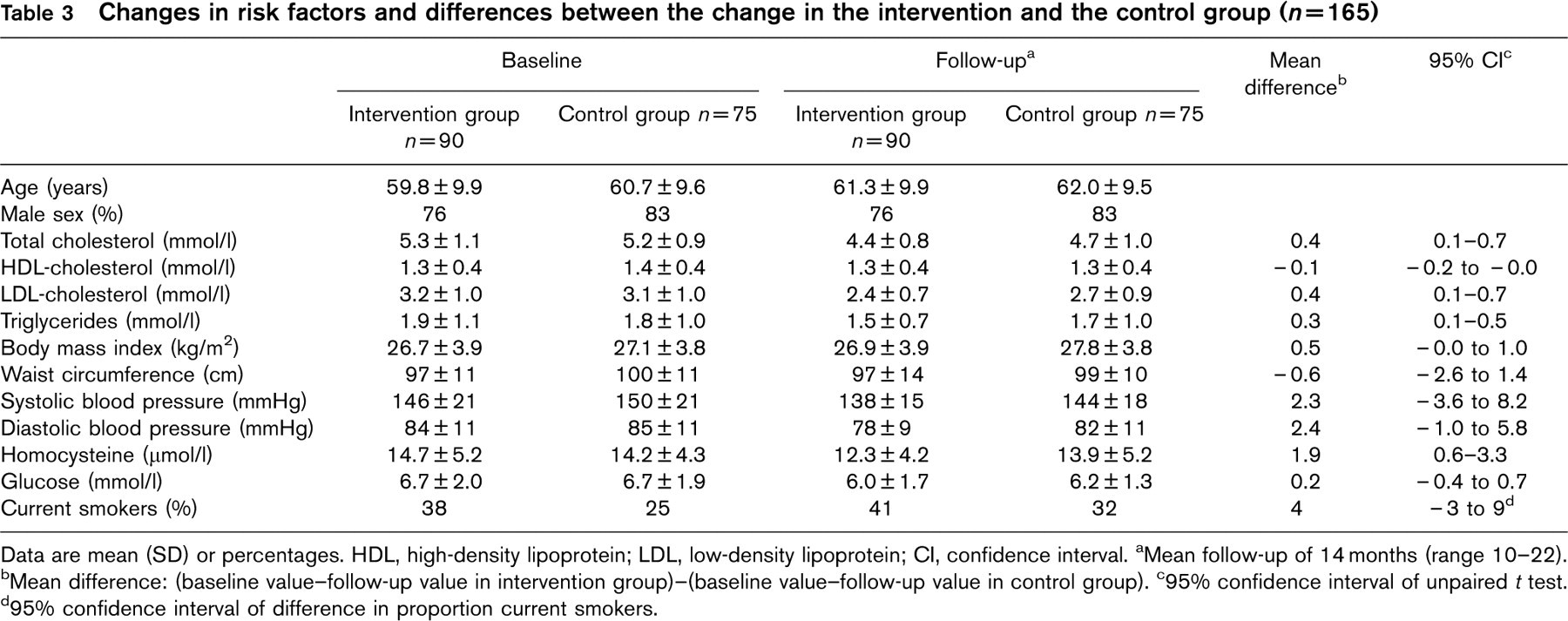
Data are mean (SD) or percentages. HDL, high-density lipoprotein; LDL, low-density lipoprotein; CI, confidence interval.
aMean follow-up of 14 months (range 10–22).
bMean difference: (baseline value-follow-up value in intervention group)-(baseline value-follow-up value in control group).
c95% confidence interval of unpaired t test.
d95% confidence interval of difference in proportion current smokers.
Treatment goals at baseline and at follow-up and odds ratios for achieving treatment goals (n = 165)
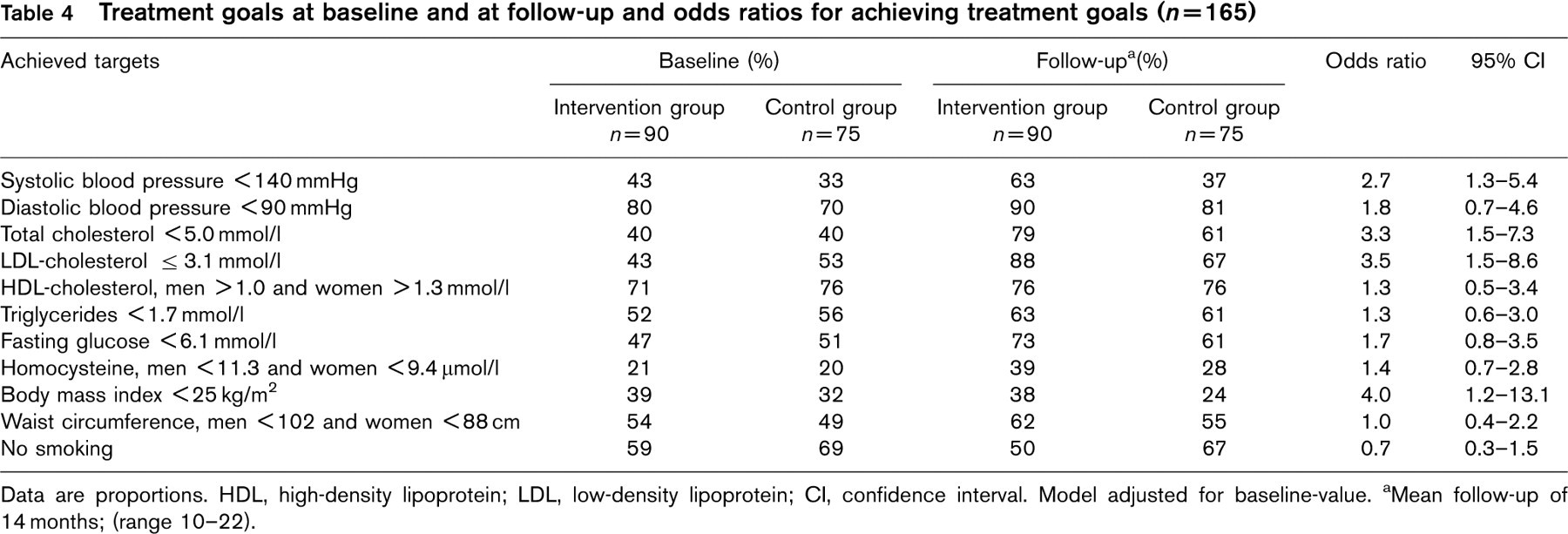
Data are proportions. HDL, high-density lipoprotein; LDL, low-density lipoprotein; CI, confidence interval. Model adjusted for baseline-value. aMean follow-up of 14 months; (range 10–22).
Medication usage in the intervention group and in the control group
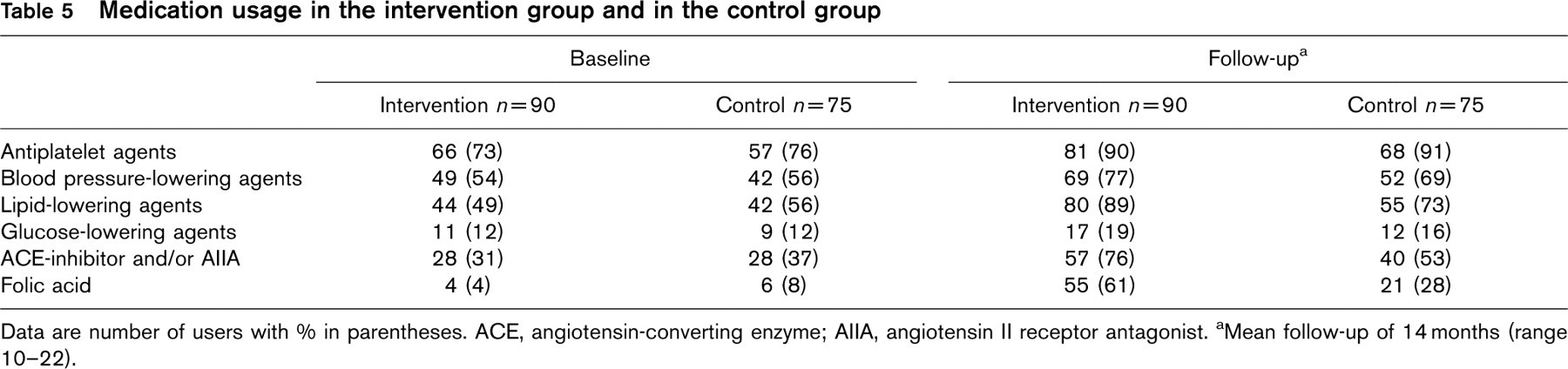
Data are number of users with % in parentheses. ACE, angiotensin-converting enzyme; AIIA, angiotensin II receptor antagonist.
aMean follow-up of 14 months (range 10–22).
Change in medication use
Regardless of group, more patients used medication at follow-up than at baseline (Table 5). At follow-up, more patients in the intervention group than in the control group used lipid-lowering drugs (89 versus 73%), angiotensin-converting enzyme inhibitor or angiotensin II receptor antagonist (76 versus 53%) and folic acid (61 versus 28%).
Quality of life
Quality of life was not significantly different between the groups at baseline or at follow-up on any scale or overall scores (data not shown).
Nurse intervention
Eighty-three of the 90 (92%) patients in the intervention group visited the nurse practitioner risk factor management clinic, making a mean of four visits (range, 1–15 times) during the follow-up period. One person died and six patients only participated in the follow-up visits. The first visit was longest, with a mean duration of 48 min (range, 15–105 min): 10 min were spent on hypertension, 5 min on hyperglycemia, 9 min on hyperhomocysteinemia, 11 min on dyslipidemia, 6 min on smoking, and 7 min on overweight. The second and third visits lasted 27 min (range, 10–60 min). In these visits less attention was paid to risk factors than during the first visit: 6 min on hypertension, 2 min on hyperglycemia, 3 min on hyper-homocysteinemia, 6 min on dyslipidemia, 4 min on smoking, and 6 min on overweight.
Discussion
In this randomized, controlled trial, we investigated whether nurse practitioner care plus usual care instead of usual care alone improved the cardiovascular risk profile of high-risk patients who underwent a vascular screening and prevention program beforehand. We found that nurse practitioner-assisted risk factor management resulted in more frequent achievement of treatment goals for systolic blood pressure (OR 2.7; 95% CI 1.3–5.4), total cholesterol (OR 3.3; 95% CI 1.5–7.3), LDL-cholesterol (OR 3.5; 95% CI 1.5–8.6) and BMI (OR 4.0; 95% CI 1.2–13.1). All patients used more medication than at baseline, and the quality of life was not different in the two groups. The prevalence of smoking was higher in both groups at follow-up than at baseline. This was partly unexpected, because of the no-smoking policies in governmental buildings, in the working environment and the strong anti-smoking messages from healthcare providers. At the start of the study smokers had quitted smoking but a considerable number of them started smoking again. Our findings confirm that in patients with recent clinical manifestations of a vascular disease, a relapse to start smoking again is a serious threat that needs continuous attention from healthcare professionals.
Earlier randomized, controlled trials of nurse practitioner care for patients with established CHD reported contradictory findings (Table 6). These studies differed from our study in sample size, study population, and some focused on a single risk factor (e.g. plasma lipids). Two longer studies showed that differences in improvements in medical and lifestyle components between intervention and control groups diminished over a 4-year period [14, 17]. For example, the OR for blood pressure diminished from 5.3 (95% CI 3.0–9.4) at 1 year to OR 1.5 (95% CI 0.9–2.4) at 4 years follow-up, but nurse-led secondary prevention clinics led to fewer total deaths and probably fewer coronary events. A systematic review of 12 different randomized, controlled trials involving 9803 patients with CHD concluded that in five of seven trials nurse practitioner intervention improved the risk factor profile, reduced hospital admissions and enhanced quality of life [33].
In contrast to many other studies, we chose a tailored and individualized intervention for vascular risk factor management in patients with PAD and cerebrovascular disease. Although, their manifestation of atherosclerosis is different, they share many common risk factors. Patients were screened for vascular risk factors, and a multidisciplinary team formulated treatment advice, which formed the basis of the nurse practitioner intervention. Thereafter, this study was conducted in the hospital instead of primary care. We think that a setting of an outpatient clinic attached to a hospital, integrating treatment of the (acute) clinical manifestation of the vascular disease and initiating risk factor treatment, is an optimal environment for successful risk management in these high-risk patients. For long-term follow-up, patients can then be seen by their GP. Communication between the GP and the vascular specialist in the hospital who is expected to take action in vascular risk management, is often sub-optimal [34].
Randomized, controlled trials among patients with coronary heart disease
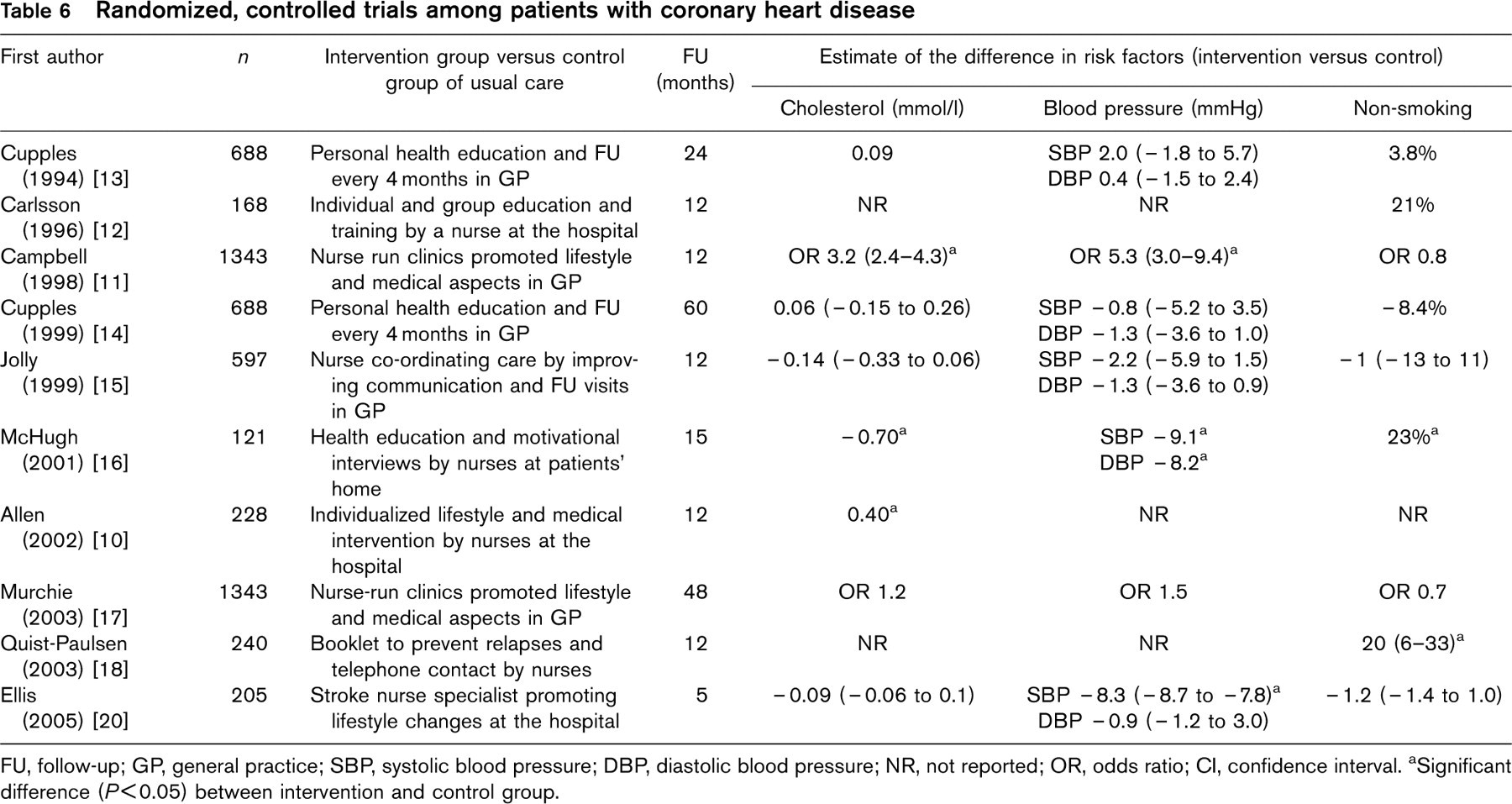
FU, follow-up; GP, general practice; SBP, systolic blood pressure; DBP, diastolic blood pressure; NR, not reported; OR, odds ratio; CI, confidence interval.
aSignificant difference (P < 0.05) between intervention and control group.
An integrated approach to vascular risk reduction in which a doctor treats the vascular problems and a nurse practitioner treats risk factors, initiates behavioral change and helps patients to cope with illness and vascular risks should be effective on vascular risk reduction in all patients with manifestations of CVD [9].
Other investigators suggest that a community approach to the prevention of CVD may be worthwhile [35]. In our opinion, risk management can only be successful if patients are given feedback on their progress by trained healthcare professionals. On average, the patients of our study visited the nurse practitioner clinic four times over a 14-month period. While such an approach is time consuming, nurse-led clinics for the secondary prevention of CHD in primary care are cost effective [36].
Our study has some potential limitations. It was conducted in a single academic medical center, and thus the results may reflect not only the effects of the nurse practitioner intervention but also the hospital setting. Moreover, VENUS was carried out in addition to a vascular screening and prevention program. Before the start of the study, the treating physicians and the GPs of all patients received letters detailing the cardiovascular risk profile of their patients, which may have motivated them to make an extra effort to alter their patients' cardiovascular risk profiles. We did not attempt to control for the type of treatment the patients received from usual care during the study. Nevertheless, we found a statistically significant improvement in risk factor management in the intervention group compared with the control group. It should be noted that the sample size in both groups was rather small to detect differences between dichotomous outcome variables. As a consequence differences may be missed due to lack of power.
We used the Zelen design instead of a conventional design because detailed knowledge of the trial and its exact purposes would have been likely to bias or influence the results of both groups of patients [37]. The Zelen design probably reduces non-compliance and drop-out considerably, thus increasing validity [38]. Furthermore, Schellings et al. [38] suggest that the design has a wider applicability, particularly when potential participants would find being in the experimental group more attractive rather than being in the control group, which receives standard treatment. The number of people who refused participation, however, was not lower (n = 61) than in other studies, although we had fewer dropouts (n = 10). Those who refused to participate can introduce a difference in prognostic factors but in VENUS hardly any differences between the baseline characteristics of the patients who did or did not participate was observed.
Lastly, medication use and smoking behavior were self-reported. It was not possible to confirm this by checking pharmacy records and by assessing a salivary sample for cotinine levels. Klungel et al. [39] found that neither a questionnaire nor pharmacy records can be considered as the ‘gold standard’ with regard to true pharmacotherapy.
In conclusion, our findings show that care provided by a nurse practitioner, in addition to usual care and on top of a vascular screening and prevention program, improved the management of important risk factors in patients with a recent clinical manifestation of a vascular disease. Adequately managed risk factors will contribute to a reduction in vascular morbidity and mortality in this group of high-risk patients.
Footnotes
Acknowledgements
We gratefully acknowledge the contribution of T. Westra (nurse practitioner), A. Sonsma (VENUS research nurse), J.M. Dijk (coordination), B. Slotboom and M. Edlinger (data managers), J. Sykes (native speaker of English), and the SMART study group, the members of which are listed in the appendix.