
Abstract
Background
Information on trends in healthy and unhealthy habits among children are important for the development of programmes intended to foster and consolidate a healthy lifestyle. This report studied the importance of time and age on the health behaviour of Swedish school children.
Methods
A comparison between health behaviours derived from repeated evaluations of Swedish school children aged 11–13 years was performed.
Results
Significant positive time trends were found in the form of increased physical activity and decreased sedentary behaviours, whereas negative time trends were observed in dietary habits and smoking. An analysis of the impact of increasing age demonstrated a negative influence including less physical activity and deteriorating dietary habits and increased smoking at the young age groups in this study.
Conclusion
Time trends and age are both important determinants of health behaviour in preteen children. Even the small age increase from 11 to 13 years had an important negative influence. The results of the present study underline that the window of opportunities to promote a healthy lifestyle in children is narrow. It is evident that a successful health intervention programme must be initiated at an early age, continued and repeated over time, and structured to counteract trends in age as well as time.
Introduction
An early introduction of a healthy lifestyle is essential in the prevention of cardiovascular and several other diseases. Poor dietary habits and a sedentary lifestyle are often founded at a young age, underlining the importance of an early initiation of health-promoting habits [1]. Daily physical activity is a cornerstone in a healthy lifestyle. Children who spend less time in moderate vigorously physical activity are more often obese than those who do [2]. The eating patterns of children and adolescents have changed considerably over time. Not the least an increasing exposure to free carbohydrates has become more common, contributing to excess calorie intake and overweight. Food rich in fat and low in fruit and vegetable content is another concern [3, 4]. Unlimited access to television and computer games introduces sedentary leisure habits, which, combined with exposure to sugar and fat-rich snacks, counteract the introduction of a healthy lifestyle [5]. Smoking causes multiple health problems throughout life, and an important public health objective is to convince children to abstain from trying tobacco products [6]. An early start of tobacco use increases the likelihood for addiction and a high consumption, thereby introducing a greater risk of tobacco-related illness [7].
Knowledge about the impact of time trends and increasing age in lifestyle-oriented risk factors among children should constitute an important source of information on the demands for and type of health-fostering activities needed to reinforce and preserve healthy habits. The aim of this investigation was to study the importance of these factors on the health behaviour of Swedish school children by comparing the outcome of a recent [8] with previous surveys [9].
Methods
The Adventure with Pelle Pump cohort
One cohort of 12-year-old children was derived from the evaluation of the Swedish health education programme ‘An Adventure with Pelle Pump’ (APP), conducted in May 2003 as presented in detail elsewhere [8]. In brief a random selection of 1369 schoolchildren (mean age 12.5 years) from 86 sixth grade classes in 78 schools representing different socio-economic and living areas across the country participated in a questionnaire-based survey on healthy habits and the knowledge of healthy behaviour.
The Health Behaviours in School Children cohorts
The WHO-based ‘Health Behaviours in School Children’ (HBSC) studies were performed in November/December 1993, 1997 and 2001 [9], targeted at children in the 5th and 7th grades (mean ages 11.5, 13.5 years). Inclusion was performed according to a two-step cluster design. First, schools were chosen to be representative of Swedish children. Second, all selected schools comprised the cluster, and one class from each school was randomly selected for the purpose of the investigation. The cohort from 1993, 1997 and 2001 consisted of 1225, 1294 and 1499 children in the 5th grade and 1208, 1357 and 1201 children in the 7th grade, respectively.
The characteristics of the APP and the HBSC cohorts are presented in Table 1.
The questionnaires
The questionnaires were distributed to the teachers with an explanatory letter. They were asked to let the children answer the questionnaires during an ordinary lesson without any instructions besides those given in the letter.
The APP questionnaire included 16 questions on health knowledge and 39 on health behaviour, including physical activity, nutrition and the use of tobacco. To facilitate comparisons, 16 of the APP questions on health behaviours were the same as those used in the HBSC studies [9]. The HBSC questionnaire consisted of 80 items in 1993, 83 in 1997 and 74 in 2001.
Descriptions of questions on health behaviours
Physical activity
After a definition and examples of common physical activity (i.e. any activity that increases your heart rate and makes you get out of breath some of the time), the children were asked how many days a week they were physically active (cumulative activity including sports, school activities, playing with friends, and walking to school) for 60 min or more.
Sedentary behaviours
Sedentary behaviours was how many hours they watched television (including video or DVD films) and used a computer (for playing games, e-mailing, chatting, or Internet surfing) in their free time during a typical weekday and weekend. The possible responses were none, less than 1 h, approximately 1–3, 4–6 or 6 or more hours per day.
Dietary variables
Dietary variables covered how many times during a typical week they had breakfast and how often they consumed fruits, vegetables, soft drinks and candy/sweets. The possible responses were never, less than once a week, 1–2, 3–4, and 5–6 days a week, once a day, and more than once a day.
Smoking
They were asked if they had ever tried smoking, and, in case of a positive reply, how often they smoked.
Statistical analysis
The time trend analysis was performed analysing trends in health behaviours of children including cohorts from 1993, 1997, 2001 and 2003. The analysis was performed using logistic regression, with time as a continuous variable. The age analysis was performed analysing trends in health behaviours of children from the 5th (age 11.5) and the 7th (age 13.5) grade in the 2001 HBSC study and 6th grade children (age 12.5) from the APP study in 2003. The analysis was performed using logistic regression with age as a continuous variable.
Characteristics of study populations of the four cohorts comprised in the time trend and age analysis

APP, An Adventure with Pelle Pump; HBSC, Health Behaviours in School Children.
A comparison of chi-squared values was further performed, in which a large value indicated greater importance. The significance level was set to P ≤ 0.05, two-sided.
The APP study was approved by the ethics committee of the Karolinska Institutet.
Results
Physical activity and sedentary behaviours
The time and age trends for physical activity and sedentary behaviours for boys and girls are shown in Fig. 1.
The proportion of children that were physically active at least 1 h every weekday increased significantly from 2001 to 2003 (P < 0.001). The age trend analysis revealed that the proportion of physically active children decreased with increasing age (P < 0.001). Time trends had a more pronounced influence on physical activity than increased age (Table 2).
The proportion of children watching television more than 1 h per day on weekdays decreased from 2001 to 2003 (P < 0.001). Increasing age resulted in decreased time watching television (girls P < 0.05). In this respect time trends was of greater importance than increased age (Table 2).
Computer use on weekdays was not affected by time among boys (NS) whereas it increased among girls from 2001 to 2003 (P < 0.01). The age trend analysis revealed a decrease in time spent using the computer with increased age (P < 0.0001), and was found to be of greater importance than changes seen over time (Table 2).
Dietary variables
As depicted in Fig. 2 regular breakfast habits declined among both boys (P < 0.001) and girls (P < 0.001) from 2001 to 2003. This decrease also related to increasing age (P < 0.001) with age more important than time trends (Table 2).
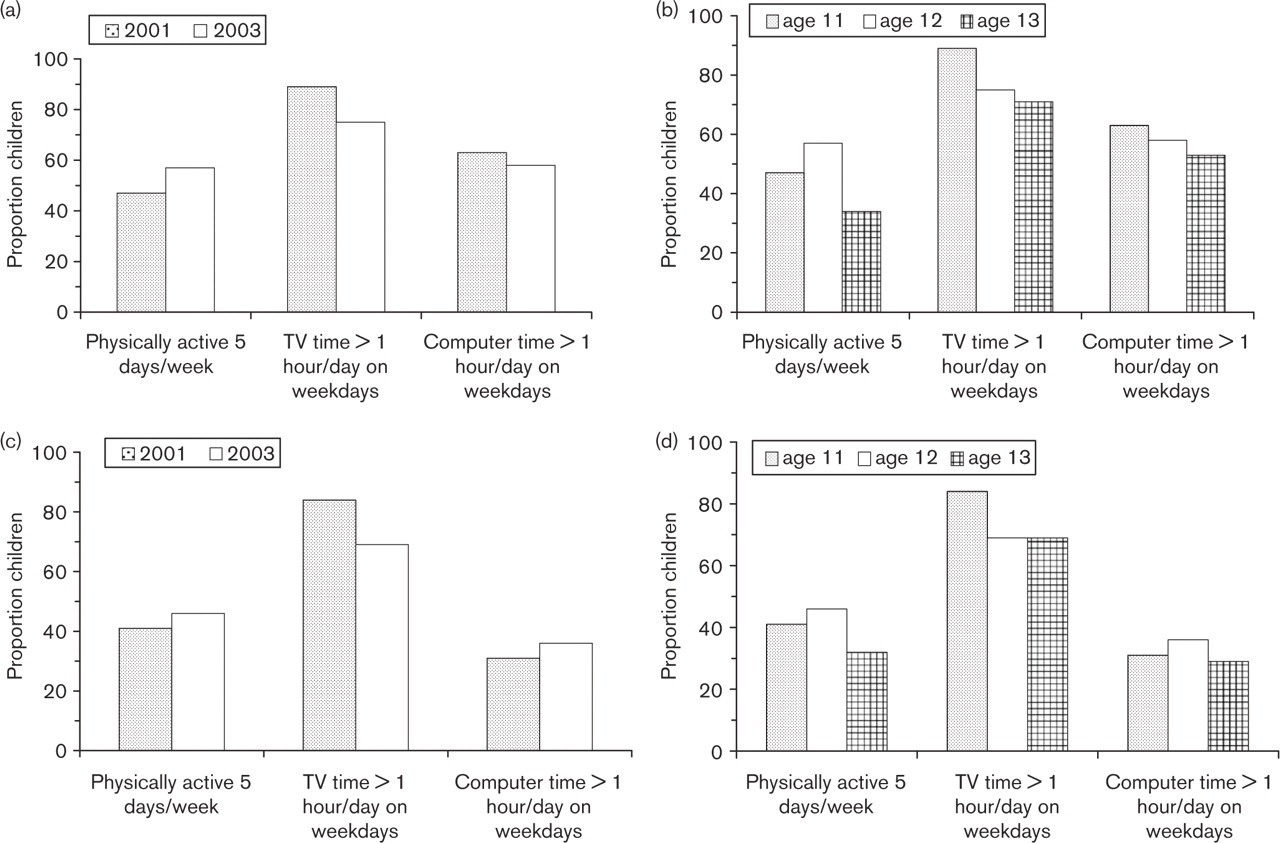
Time and age trends in physical activity and sedentary behaviours. Proportion of children with high frequencies of physical activity, watching television and computer use, described in: (a) time trends on physical activity and sedentary behaviours of boys; (b) age trends on physical activity and sedentary behaviours of boys; (c) time trends on physical activity and sedentary behaviours of girls; (d) age trends on physical activity and sedentary behaviours of girls.
Results from the chi-squared analysis of age and time trends
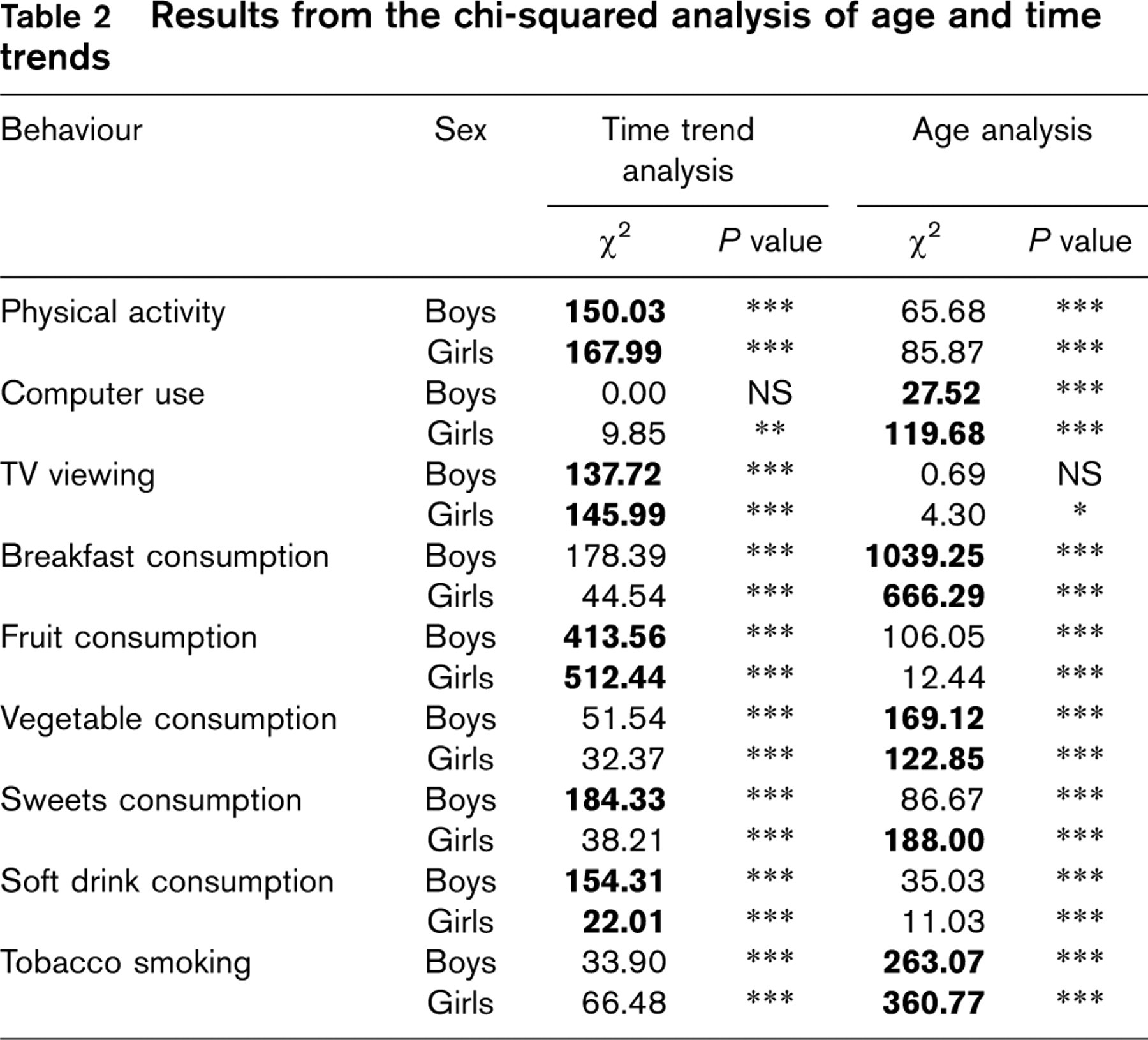
Bold indicates the highest chi-squared value for each behaviour and thus the strongest trend. P values:
∗ P ≤ 0.05;
∗∗ P<0.01;
∗∗∗ P<0.001.
NS, not significant.
A decline in fruit intake (P < 0.001) was seen from 1993 to 2003. Although there was an age dependency with decreased fruit intake by increasing age (P < 0.001), time was of greater importance (Table 2).
An overall increase in vegetable intake (P < 0.001) was seen from 1993 to 2003, with a decline from 2001 in boys and 1997 in girls. An increase in age resulted in a decrease in vegetable intake with age (P < 0.001) of greater importance than time trends (Table 2).
Daily sweet consumption was low during the whole period of time, but there was a decrease from 1993 to 2003 (P < 0.001). An age dependency, increased consumption with increased age (P < 0.001), was seen in the consumption of sweets among both boys and girls. For boys a time trend was of greater importance than age, in contrast to girls in whom age was more important (Table 2).
A similar decrease in the proportion of children consuming soft drinks daily (P < 0.001) was seen from 1993 to 2003. The age trend analysis revealed an age dependency of increased consumption by age for boys and decreased consumption for girls (P < 0.0001), but time trend was, despite low changes and low consumption, of greater importance than age (Table 2).
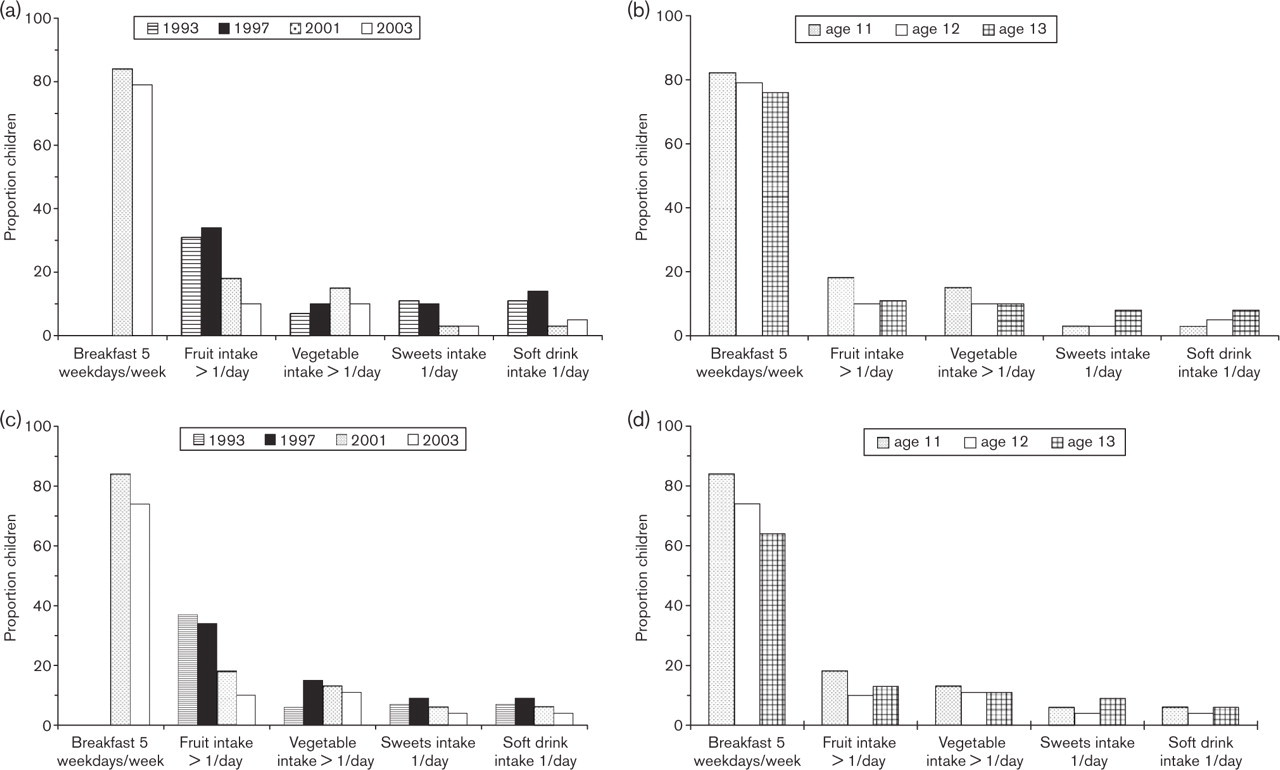
Time and age trends in dietary patterns. Proportion of children with a high consumption of breakfast, fruit, vegetables, sweets and soft drink described in: (a) time trends on dietary patterns of boys; (b) age trends on dietary patterns of boys; (c) time trends on dietary patterns of girls; (d) age trends on dietary patterns of girls.
Smoking
Time and age trends in smoking behaviours for both boys and girls are illustrated in Fig. 3. More children (P < 0.001) had tried smoking at least once in 2003 than in 2001. The proportion of children having tried smoking at least once increased with increased age. Age was of greater importance for the development of tobacco habits than time trends (P < 0.001; Table 2).
Discussion
This analysis of the impact of time trends and increasing age on lifestyle-oriented habits of importance for future health demonstrated a favourable time trend as regards physical activity, whereas essential eating habits deteriorated. Lifestyle habits were clearly influenced both by time trends and increasing age. Importantly, the small increase from 11 to 13 years of age had a strong negative influence on breakfast and vegetable consumption as well as the use of tobacco.
In the present study, physical activity and inactivity was analysed by two variables, one as time spent being physically active and the other as time spent engaged in sedentary behaviours, such as television viewing and computer use. The current recommendation on physical activity for school-age children is that they should participate in at least 60 min of ‘daily, moderate to vigorous physical activity that is developmentally appropriate, enjoyable, and involves a variety of activities’ [10]. Only 57% of the boys and 46% of the girls in the 2003 APP cohort reached this goal, supporting previous findings that at least 50% of children and adolescents are insufficiently physically active [11–13]. However, the increased proportion of physically active children in 2003 compared with 2001 must be seen as encouraging, further reinforced by the observation that sedentary behaviour as regards television viewing and time spent using the computer decreased during the same period of time. This may be the result of seasonal variations in physical activity and sedentary behaviours. However, this encouraging development may also relate to extensive health promotion strategies, such as the ‘Bunkeflo project’ and ‘Put Sweden on the Move’ [14], aimed at increasing physical activity among Swedish school children during the last decade. Promotion strategies thus have the potential to influence the health behaviour of children when implemented in the right context.
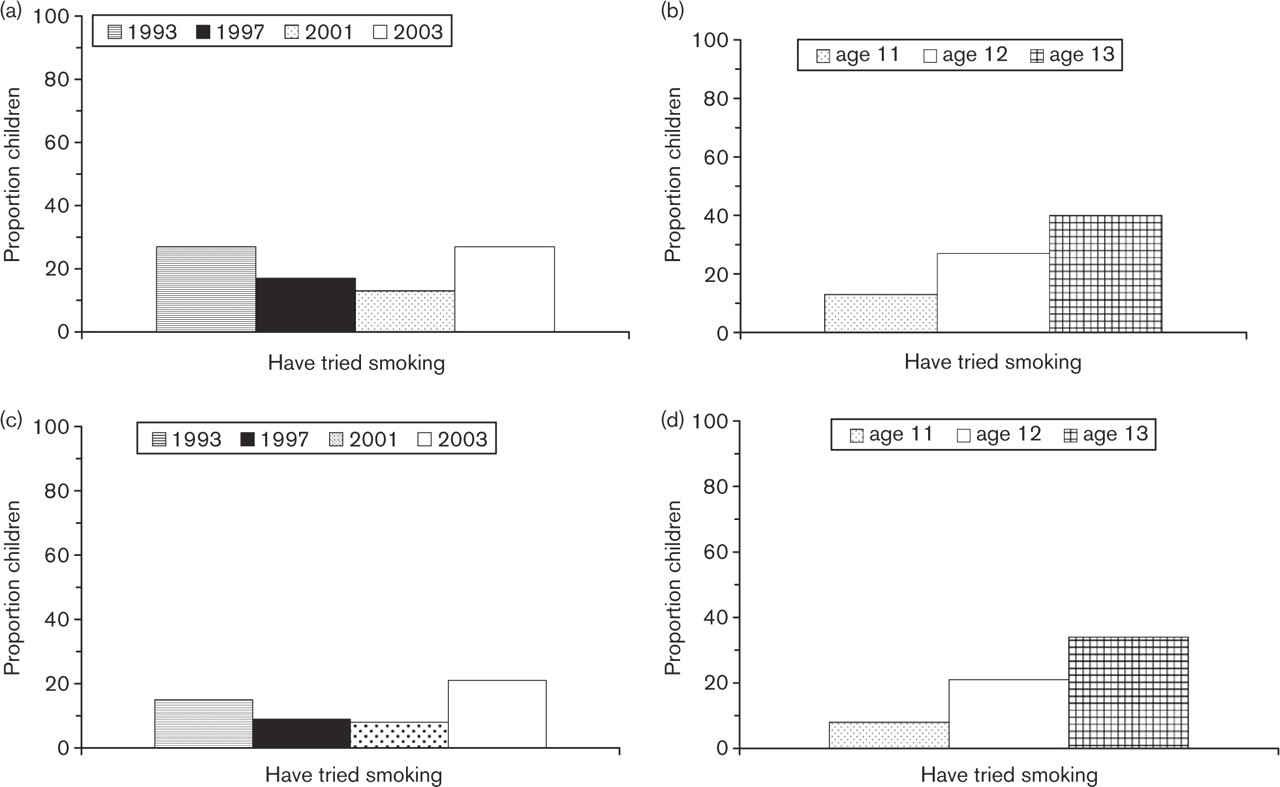
Time and age trends on smoking habits. Proportion of children having tried smoking at least once, described in: (a) time trends on smoking of boys; (b) age trends on smoking of boys; (c) time trends on smoking of girls; (d) age trends on smoking of girls.
Breakfast intake deteriorated by time. This change was even stronger in the age-dependent analysis, highlighting the importance of early initiation and continued effort to create healthy habits. Breakfast consumption is a predictor for the whole-diet nutrient adequacy, and skipping breakfast is a common behaviour in overweight or obese children [15]. Another key factor in the preservation of health is the consumption of fruit and vegetables [16]. Nutritional surveys show that children and adults in most regions of the world are not meeting the minimum suggested consumption goals of 400 g per day of fruit and vegetables [17, 18]. In the present study, fruit and vegetable consumption decreased by age, which has also been described elsewhere [19]. Fruit and vegetables may replace other, less favourable, products, and a low fruit and vegetable intake has been related to frequent television viewing among adolescents [20], demonstrating that lifestyle factors interact, and has to be looked at in a comprehensive manner.
The time analysis showed a decrease in the consumption of soft drinks and sweets, which contrasts with contemporary media reports on unhealthy food habits among children and adolescents. However, the age analysis pointed in another direction, with the increased consumption of these products by increasing age. Once more and taking both time trends and increasing age into consideration, the implication is that food habits need more attention early in life.
That the previously noted decrease in the proportion of children who had tried smoking reverted to an increasing proportion was disappointing, in particular considering the very young age in the most recent cohort of children. This negative trend was somewhat more apparent among girls, who are now approaching the smoking levels of boys. Tobacco use in pre-adolescence has been found to differ between the sexes, with an earlier initiation among boys but a more rapid transition to regular smoking among girls [21]. Although both time trends and increasing age had a highly significant impact on tobacco use, the interpretation of these data are somewhat difficult, as part of the time trend may be explained by the difference in age between the cohorts. However, these data have to be taken seriously and both time and age trends demonstrate that a non-smoking programme must be initiated early and continued long term to be effective.
Study limitations
The character of this study using different cohorts of children did not allow a formal interaction analysis to isolate the impact of time from that of age on behaviour. As described, the analyses for time and age were adjusted in an attempt, at least to some extent, to circumvent these shortcomings. As age differences in the population studied were rather small, it is evident that changes appear quickly in these rather young children.
The study was based on self-reported information. Limitations, such as the potential for self-report bias and errors in recall, have to be recognized. Information on dietary patterns, physical activity variables, and smoking habits were available only in a frequency domain but not as the total volume of these variables. Self-reports on tobacco behaviours in particular among preteens and adolescents may be regarded as even less reliable. However, a validity study on the concordance between self-reported tobacco use and saliva cotinine (a metabolite of nicotine) concentration in Swedish adolescents (age 15 years) concluded that adolescents give reports of tobacco use that are both high in reliability and validity [22].
The lack of an analysis of the non-responders in the different cohorts may be considered as a limitation. This was impossible for ethical reasons but a high response rate, 85–90%, enhanced the general applicability of the results.
Conclusion
Although it might be difficult to control time trends, the influence of age may be counteracted by the early initiation of promotion programmes and strategies. The finding that an increase of approximately 2 years of age has a definite negative impact on health behaviours in children must therefore be taken seriously. The results of the present study underline that the window of opportunities to promote a healthy lifestyle in children is indeed narrow. It is evident that a successful health intervention programme must be initiated at an early age, continued and repeated over time and structured to counteract trends in age as well as time.
Footnotes
Acknowledgements
The authors would like to extend their sincere gratitude to Mia Danielsson and Ulla Marklund, PhD, principal investigators for the Swedish national research team for HBSC at the National Institute of Public Health, Stockholm, Sweden, for access to data from the HBSC studies. They would also like to extend their gratitude to all the children who participated in this study and to their teachers for helping with the distribution of the questionnaires.