
Abstract
Background
There is convincing evidence that regular physical activity reduces risk factors for cardiovascular diseases (CVD) among men. However, only a few studies have been conducted among women. Most previous studies have focused on the effects of leisure-time physical activity on cardiovascular risk factors, without considering the impact of occupational or commuting physical activity.
Design
Four independent cross-sectional surveys were carried out at 5-year intervals within the framework of the FIN MONICA studies in 1982, 1987, 1992 and 1997.
Methods
An independent random sample was drawn from the national population register for each survey. The samples were stratified by sex and 10-year age categories according to the WHO MONICA protocol. The survey consisted of a self-administered questionnaire.
Results
Not only leisure-time physical activity, but also commuting activity was directly associated with high-density lipoprotein (HDL)-cholesterol and was inversely related to body mass index (BMI) and waist circumference among both men and women. High occupational physical activity was related to high HDL-cholesterol levels and high total serum cholesterol levels in both sexes and to lower BMI, waist circumference and diastolic blood pressure (DBP) in men. High leisure-time physical activity was associated with reduced DBP among both men and women, whereas high occupational physical activity was related to lower DBP only among men.
Conclusion
Not only leisure-time physical activity but also commuting activity is associated with reduced levels of some cardiovascular risk factors. All forms of physical activity should be promoted to reduce CVD in the population.
Introduction
Cardiovascular diseases (CVD) are the primary cause of death across Europe [1]. Many epidemiological studies have shown that low physical activity is a strong and independent risk factor for CVD [2–4], and that regular physical activity reduces cardiovascular and all-cause mortality [5–9]. A sedentary lifestyle has been estimated to be responsible for approximately a third of deaths from coronary heart disease, colon cancer and diabetes [10].
Even though there is convincing evidence that regular physical activity reduces risk factors for CVD among men [6,11–15], only a few studies have been conducted among women [8,16–20]. Furthermore, most previous studies have focused on the effects of leisure-time physical activity on cardiovascular risk factors [17,21–25], without considering the impact of other forms of physical activity. The findings of studies assessing the relationship of occupational physical activity or commuting activity with cardiovascular risk factors are limited and inconsistent [8,12,14–16,20,26–31].
Recent recommendations encourage people to practice 30 min or more of moderate-intensity physical activity on most days of the week [32,33]. Whereas some individuals could increase their physical activity in leisure time, others may gain a health benefit from being more physically active on their way to work or at work. Therefore, it is important to understand the separate effects of the different forms of physical activity on cardiovascular risk factors.
The purpose of our study was to investigate separately for men and women the association between leisure-time, occupational and commuting physical activity on the most common risk factors of CVD adjusted for a number of confounding factors.
Materials and methods
Study population
Four independent cross-sectional surveys were carried out at 5-year intervals within the framework of the FINMONICA studies in 1982, 1987, 1992 and 1997. The FINMONICA study was the Finnish part of the multinational MONICA project initiated by the World Health Organization (WHO) in 1982 [34]. The first two surveys were conducted in three regions: the provinces of North Karelia and Kuopio, which are both located in eastern Finland and the region of Turku-Loimaa in south-western Finland. The survey was expanded to other regions after 1987.
An independent random sample was drawn from the national population register for each survey. The samples were stratified by sex and 10-year age categories according to the WHO MONICA protocol [35]. The common age range of the four surveys was 25–64 years and the participation rates varied between 73 and 79% in men and between 83 and 85% in women. Informed written consent was obtained from the participants of all surveys. The Institutional Review Board approved the risk factor survey in 1997.
Assessment of physical activity
Leisure-time physical activity, occupational physical activity and commuting activity were determined by a self-administered questionnaire. The time frame of the activity questionnaire was a typical week. A detailed description of the questions for physical activity is presented elsewhere [36–38]. These questions were similar to those used and validated in the ‘Seven Countries Study’ [39]. In the present study, leisure-time physical activity was defined as voluntary and purposeful physical activity, carried out in order to improve or maintain one or more components of physical fitness (exercise). Leisure-time physical activity was classified as follows: (i) high: participation in recreational sports (for example running, jogging, skiing, gymnastics, swimming, ball-games or heavy gardening) or in intense training or sports competitions for at least 3 h a week; (ii) moderate: walking, cycling or practising some other form of light exercise (fishing, gardening and hunting) for at least 4 h per week; and (iii) low: reading, watching TV or working in the household without much physical activity.
Occupational physical activity was classified as follows: (i) high: lots of walking and lifting at work, taking the stairs or walking uphill (for example industrial work, farm work, forestry); (ii) moderate: walking quite a lot at work without lifting or carrying heavy objects; and (iii) low: mostly sedentary work without much walking (for example, working in an office).
Commuting activity was classified as follows: (i) high: more than 30min physical exercise (walking, cycling) every day while getting to work and back home; (ii) moderate: exercising between 15 and 30min daily on the way to work and back home; and (iii) low: exercising less than 15min daily on the way to work and back home.
Assessment of cardiovascular risk factors
All measurements were conducted by nurses specially trained in the survey procedures. Blood pressure was measured from the right arm of the subject, who was seated for 5 min before the measurement. The fifth phase of the Korotkoff sounds was recorded as the diastolic blood pressure (DBP). Blood pressure was measured twice, recorded to the nearest 2mmHg, and the mean of these two measurements was used in the analyses.
Height was measured to the nearest 0.5 cm. Weight was measured with the subject wearing light clothing. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Waist circumference was measured in centimetres. It was measured from the midway between the inferior margin of the last rib and the crest of the ileum, as recommended by the WHO [40]. Non-fasting serum total cholesterol and high-density lipoprotein (HDL)-cholesterol concentrations after the precipitation of beta-lipoproteins with dextran sulphate and magnesium chloride were determined using an enzymatic method (CHOD-PAP; Böhringer Mannheim, Germany). A new batch of dextran sulphate sodium salt (lot no. MM 97012, Pharmacia, Sweden) for the precipitation of apolipoprotein B-containing lipoproteins was introduced into the laboratory in May 1987. However, the HDL-cholesterol values with the new precipitant were approximately 4.4% lower than those measured with the old precipitant. Therefore, the results measured before May 1987 were corrected using the following formula: HDL-cholesterol = (((HDL old − 1.2621)/0.3592) × 0.3230) + 1.1969. After this correction, the average and standard deviation of the sample results were the same as those measured using the new precipitant. The correct formula was found by measuring the HDL-cholesterol in 299 samples using both methods. The formula to correct for these two different methods was constructed based on the means of these methods. All lipoprotein determinations were made in the same central laboratory (National Public Health Institute, Department of Biochemistry) and the laboratory data were standardized against the WHO reference laboratory in Prague.
Smoking habits were classified according to three categories: never smokers, ex-smokers (those, who had smoked regularly but had stopped smoking at least 6 months before the survey) and current smokers.
Alcohol consumption was assessed with questions on the types, frequency, and amount of alcohol consumed during the previous week. An alcohol index was calculated indicating the amount of alcohol in grams per week.
Education was assessed in years and the subjects were divided into following categories: (i) low, 0-6 years of education; (ii) middle, 7-9 years of education; (iii) high, more than 9 years of education.
Statistical analyses
Statistical analyses were performed using SPSS for Windows 11.0 (SPSS Inc., Chicago, Illinois, USA). The analyses were performed separately for men and women. The models including waist circumference concerned data on surveys conducted between 1987 and 1997 only. As a result of the research design, it was not possible to exclude subjects taking lipid-lowering drugs. General linear models were used to compare mean systolic blood pressure (SBP) and DBP, BMI, HDL and total cholesterol as well as waist circumference among the three groups of different physical activity levels. The mean values and the 95% confidence intervals are presented. The differences between the groups were tested for statistical significance using the least significant difference test. A P value of less than 0.05 was chosen as the level of statistical significance. Two different models were constructed. Model one included the following covariates: area and year of survey, age, education, smoking status, alcohol intake, and two other types of physical activity. The second model included BMI in addition to the covariates mentioned above. Analyses with total cholesterol were further adjusted for HDL-cholesterol and analyses with HDL-cholesterol for total cholesterol, respectively. The correlation coefficient between leisure-time physical activity and occupational physical activity was 0.017, between leisure-time physical activity and commuting activity 0.047, and 0.124 between occupational physical activity and commuting activity, respectively.
For the logistic regression analysis, dichotomous variables for SBP (cutoff 140 mmHg) and DBP (cutoff 90mmHg), BMI (cutoff 25kg/m2), HDL (cutoff 1.0 for men and 1.2 for women) and total cholesterol (cutoff 5 mmol/l) as well as waist circumference (cutoff 94cm for men and 80cm for women) were constructed according to the newest recommendations of the Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice [33]. The odds ratios and the 95% confidence intervals are presented. The models included year of survey, age, education, smoking status, alcohol intake, total cholesterol level, BMI and the physical activity variables.
Results
The baseline characteristics of the study population are presented in Table 1. The majority of men (52%) and women (54%) reported moderate levels of leisure-time physical activity, whereas 41% of men and 46% of women had low occupational physical activity. Only 27% of men and 42% of women achieved more than 15min commuting activity daily.
Table 2 presents the risk factors for CVD among groups with different levels of leisure-time physical activity separately for men and women. When adjusted for age, area and year of survey, education, smoking, alcohol intake, total cholesterol, occupational physical activity and commuting activity, leisure-time physical activity was inversely associated with BMI and waist circumference in both men and women. The association between leisure-time physical activity and waist circumference got weaker after further adjustment for BMI; however, it remained significant (model 2). The lowest DBP level was seen in both sexes among individuals with high leisure-time physical activity. The differences in DBP between the low and the high leisure-time physical activity group decreased by 37% in men and by 61% in women, but remained statistically significant after adjustment for BMI. Leisure-time physical activity was also directly associated with HDL-cholesterol levels after adjustment for age, area and year of survey, education, smoking, alcohol intake, BMI (model 2), occupational physical activity and commuting activity.
Whereas mean waist circumference and DBP among men with high occupational physical activity was statistically significantly lower compared with those with low occupational physical activity even after adjustment for BMI, no significant difference in waist circumference or DBP between the groups was found among women after adjustment for BMI (Table 3). Men with high occupational physical activity had a significantly lower BMI (P < 0.05), but surprisingly women with high occupational physical activity had a higher BMI compared with individuals with moderate or low occupational physical activity (P < 0.05). HDL-cholesterol levels were highest among men and women with high occupational physical activity in both models. Men and women with high occupational physical activity had higher total cholesterol levels than those with moderate or low levels of occupational physical activity.
Baseline characteristics of men and women
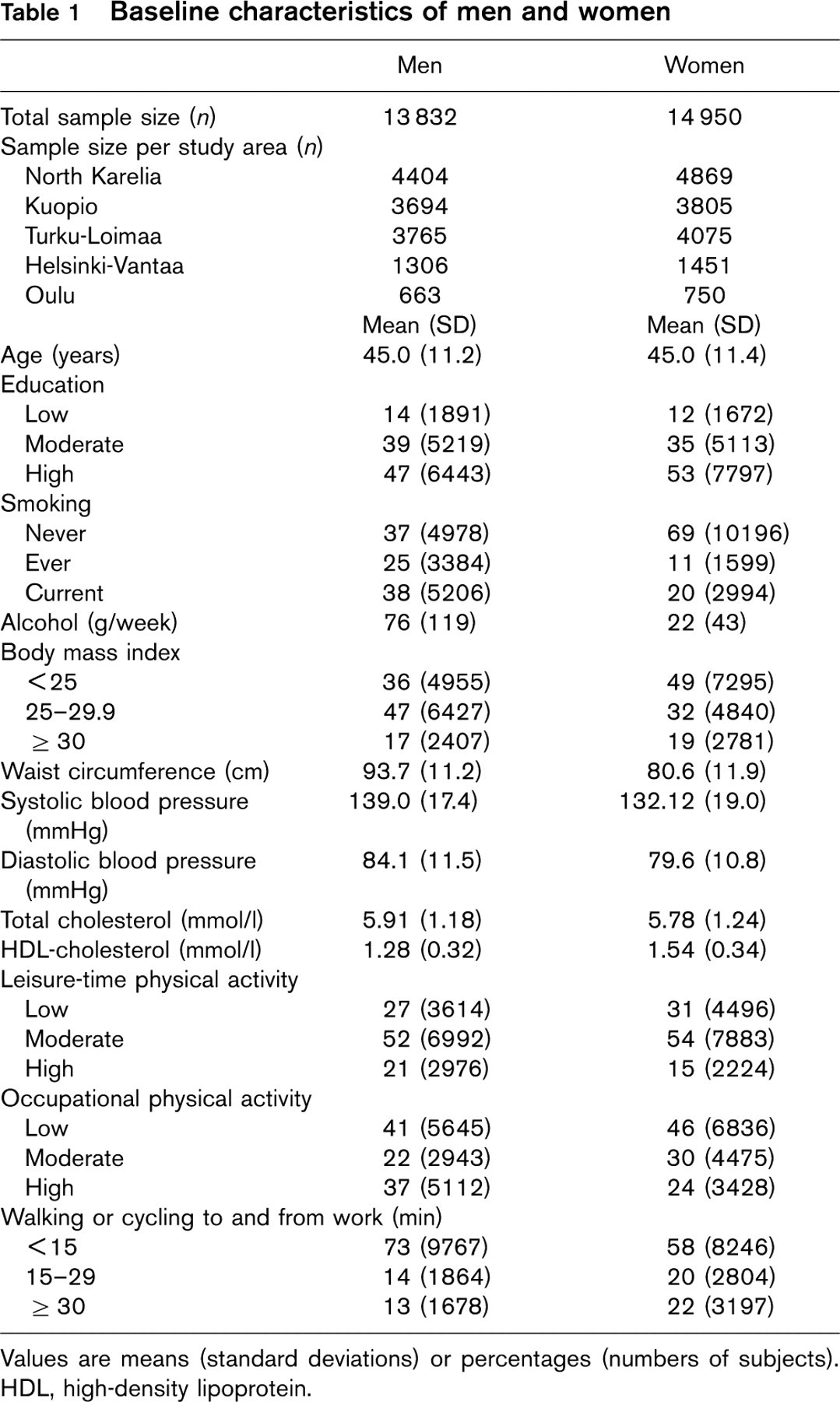
Values are means (standard deviations) or percentages (numbers of subjects). HDL, high-density lipoprotein.
Men and women with at least 30min of commuting activity daily had a significantly lower BMI, a smaller waist circumference and higher HDL-cholesterol levels than those with less than 15 min commuting activity daily after adjustment for age, area and year of survey, education, smoking, alcohol intake, BMI (model 2), leisure-time and occupational physical activity (Table 4).
Men with high leisure-time physical activity had a 34% lower probability and physically active women had a 50% smaller probability of being overweight compared with individuals with low leisure-time physical activity levels (Table 5). Compared with men and women with low leisure-time physical activity, those with high leisure-time physical activity had a significant lower probability of having enlarged waist circumference (men –67%; women –34%), having elevated DBP (men –24%; women –21%) and having increased HDL-cholesterol levels (men –34%; women –32%). Furthermore, individuals with high commuting activity showed a lower prevalence of overweight (men and women), enlarged waist circumference (women) and low HDL-cholesterol (men) (Table 5).
Discussion
This is to our knowledge the first study that has analysed separately the relationship between different forms of daily physical activity and cardiovascular risk factors in a large population sample of men and women and adjusting for a number of confounding factors. Our results show that not only leisure-time physical activity, but also commuting activity was directly associated with HDL-cholesterol and was inversely related to BMI and waist circumference among both men and women. High occupational physical activity was related to high HDL-cholesterol and high total serum cholesterol levels in both sexes and to lower BMI and waist circumference in men. High leisure-time physical activity was associated with reduced DBP among both men and women, whereas high occupational physical activity was related to lower DBP only among men.
An important finding of our study was that all separate forms of physical activity were associated with a lower BMI and a smaller waist circumference in both men and women, except occupational physical activity among women. Our findings are in accordance with a majority of studies indicating an inverse association between leisure-time physical activity and BMI [6,8,11,16,17,22,25–27] or waist circumference [11]. Only a few studies have reported no associations between leisure-time physical activity and BMI [16,21,26] or a significant inverse relationship between leisure-time physical activity and waist circumference only [28,41]. Findings about the associations between occupational physical activity and BMI have been inconsistent. Only two studies reported an inverse association between occupational physical activity and BMI [31,42]. Other studies did not find a significant relationship between occupational physical activity and BMI in men [16,27] or women [8,16]. In support of our results, the two studies assessing the effects of commuting activity and BMI or waist circumference [11,29] found an inverse association between commuting activity and BMI and waist circumference among men [11] and BMI in women [29].
Cardiovascular risk factors according to leisure-time physical activity among 25–64-year-old men and women in Finland
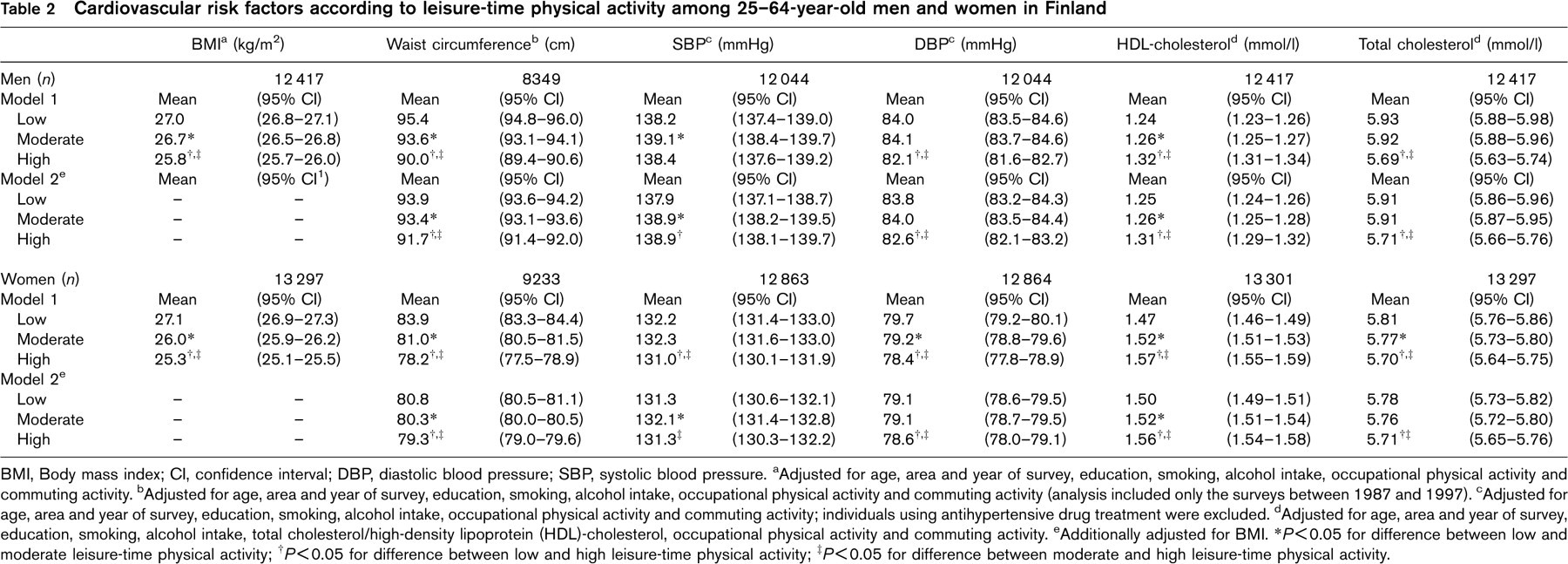
BMI, Body mass index; CI, confidence interval; DBP, diastolic blood pressure; SBP, systolic blood pressure. aAdjusted for age, area and year of survey, education, smoking, alcohol intake, occupational physical activity and commuting activity. bAdjusted for age, area and year of survey, education, smoking, alcohol intake, occupational physical activity and commuting activity (analysis included only the surveys between 1987 and 1997). cAdjusted for age, area and year of survey, education, smoking, alcohol intake, occupational physical activity and commuting activity; individuals using antihypertensive drug treatment were excluded. dAdjusted for age, area and year of survey, education, smoking, alcohol intake, total cholesterol/high-density lipoprotein (HDL)-cholesterol, occupational physical activity and commuting activity. eAdditionally adjusted for BMI. ∗P < 0.05 for difference between low and moderate leisure-time physical activity; †P < 0.05 for difference between low and high leisure-time physical activity; ‡P < 0.05 for difference between moderate and high leisure-time physical activity.
Cardiovascular risk factors according to occupational physical activity among 25–64-year-old men and women in Finland
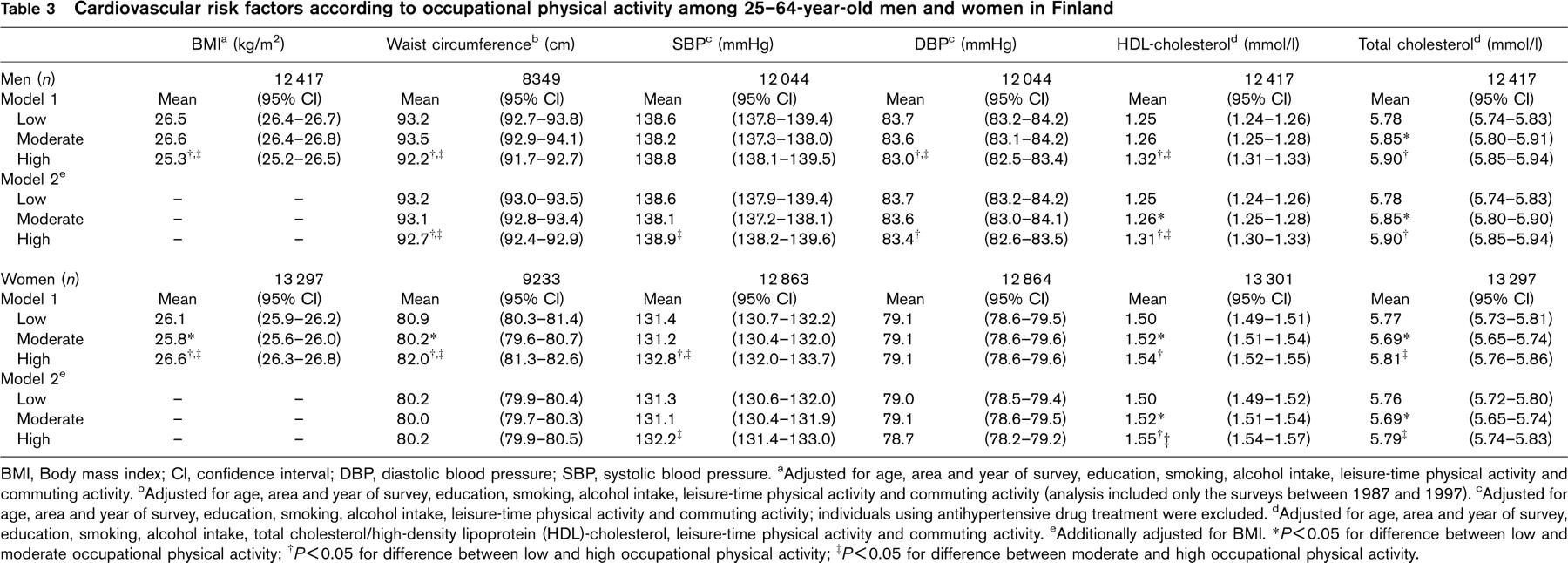
BMI, Body mass index; CI, confidence interval; DBP, diastolic blood pressure; SBP, systolic blood pressure. aAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and commuting activity. bAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and commuting activity (analysis included only the surveys between 1987 and 1997). cAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and commuting activity; individuals using antihypertensive drug treatment were excluded. dAdjusted for age, area and year of survey, education, smoking, alcohol intake, total cholesterol/high-density lipoprotein (HDL)-cholesterol, leisure-time physical activity and commuting activity. eAdditionally adjusted for BMI. ∗P < 0.05 for difference between low and moderate occupational physical activity; †P< 0.05 for difference between low and high occupational physical activity; ‡P < 0.05 for difference between moderate and high occupational physical activity.
Cardiovascular risk factors according to commuting activity among 25–64-year-old men and women in Finland
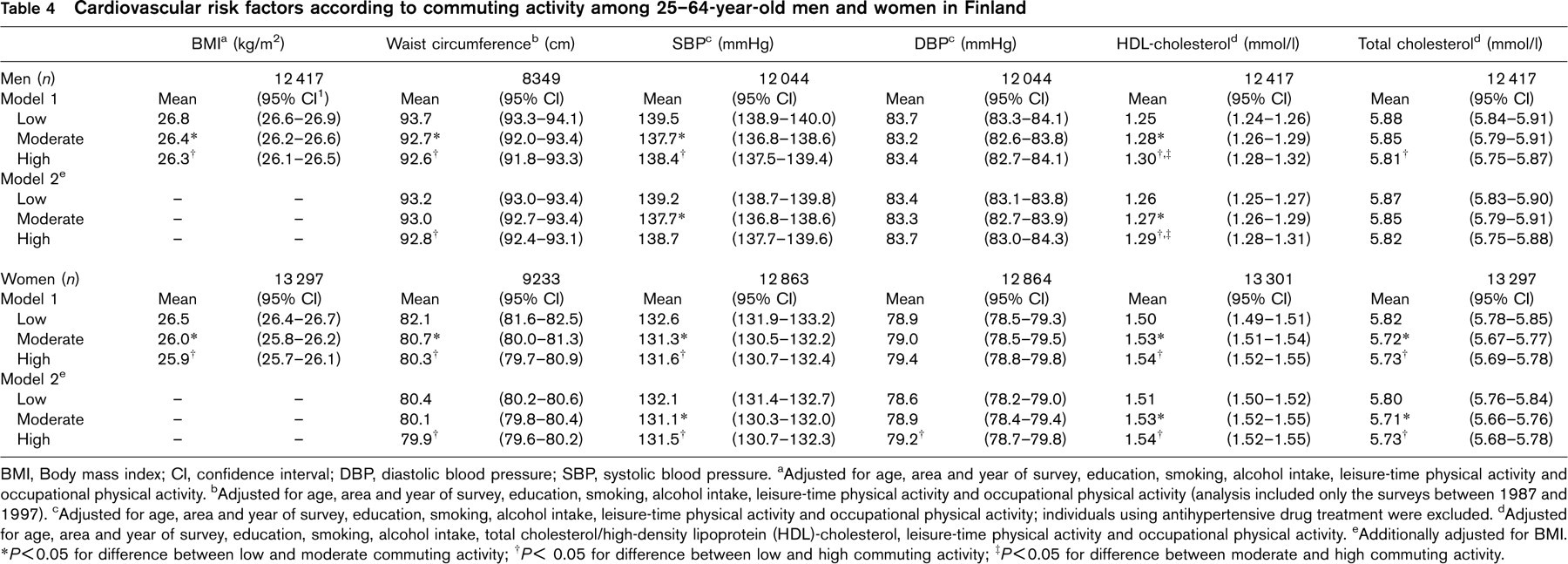
BMI, Body mass index; CI, confidence interval; DBP, diastolic blood pressure; SBP, systolic blood pressure. aAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and occupational physical activity. bAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and occupational physical activity (analysis included only the surveys between 1987 and 1997). cAdjusted for age, area and year of survey, education, smoking, alcohol intake, leisure-time physical activity and occupational physical activity; individuals using antihypertensive drug treatment were excluded. dAdjusted for age, area and year of survey, education, smoking, alcohol intake, total cholesterol/high-density lipoprotein (HDL)-cholesterol, leisure-time physical activity and occupational physical activity. eAdditionally adjusted for BMI. ∗P < 0.05 for difference between low and moderate commuting activity; †P < 0.05 for difference between low and high commuting activity; ‡P < 0.05 for difference between moderate and high commuting activity.
Physical activity has been associated with reduced blood pressure in observational studies [43,44] and clinical trials [45–47]. However, associations between physical activity and blood pressure have been inconsistent in cross-sectional studies. Even though some studies observed an inverse association between leisure-time physical activity and blood pressure among both men [5,26] and women [17,18,25,26,28], other studies could not support these findings [9,20,21,29]. Our findings are generally in line with the observations of Marti and co-workers [19], who showed a lack of association between mean arterial pressure and leisure-time physical activity. However, we found a significantly reduced DBP among men and women with high leisure-time physical activity. Their study was carried out earlier among the population in eastern Finland where a part of our study was also conducted. Studies investigating the effect of occupational physical activity or commuting activity on blood pressure are very rare. Whereas occupational physical activity seemed to be associated with a lower DBP [9,14] and SBP [14] among men, no significant association between occupational physical activity and blood pressure was observed among women [20]. Our results partly support these findings showing a lower DBP in men with high occupational physical activity. A Japanese cohort study showed that commuting activity decreased the risk of hypertension in Japanese men [42]. In Chinese men, more than 60 min commuting activity was associated with the highest mean SBP (men and women) and DBP (men). The lowest mean blood pressure values were found among those individuals with 31–60 min of commuting activity [29].
It is difficult to explain why cross-sectional studies have difficulties in showing differences in blood pressure among physical activity groups. Most likely physical activity reduces blood pressure by weight loss. However, our results remained the same even when we analysed the associations of leisure time, occupational physical activity and commuting activity with blood pressure separately in individuals with normal body weight and overweight. Differences in physical activity measurements and adjustments for confounding factors may also explain the inconsistent findings of previous studies. We conclude that other confounding factors exist that we could not control for, such as salt intake or stress.
Our results are in line with previous results indicating that leisure-time physical activity has been positively associated with HDL-cholesterol concentrations among men [6,12,13,15,23–25,48] and women [18,20,22,25,26].
Cardiovascular risk factors according to leisure-time, occupational physical activity and commuting activity levels among 25–64-year-old men and women in Finland
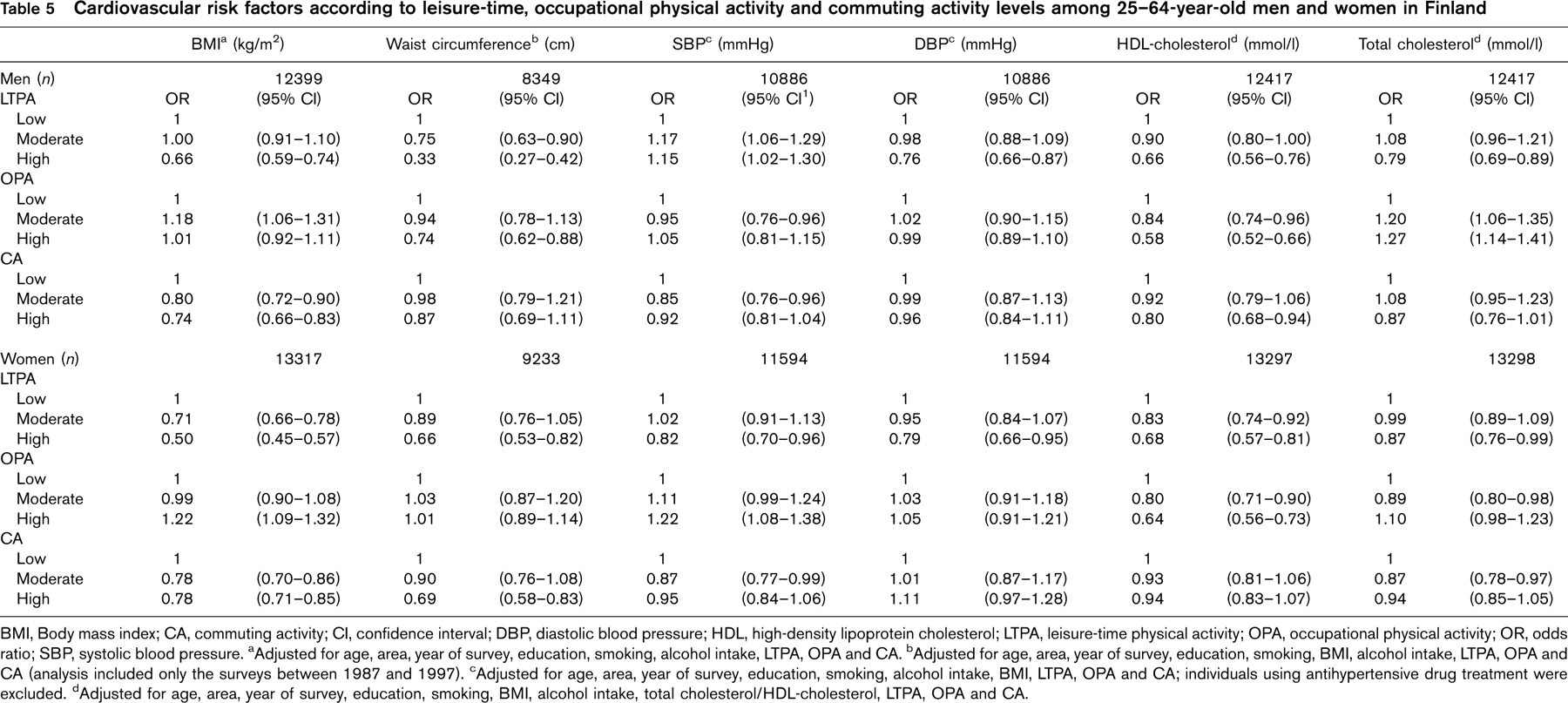
BMI, Body mass index; CA, commuting activity; CI, confidence interval; DBP, diastolic blood pressure; HDL, high-density lipoprotein cholesterol; LTPA, leisure-time physical activity; OPA, occupational physical activity; OR, odds ratio; SBP, systolic blood pressure. aAdjusted for age, area, year of survey, education, smoking, alcohol intake, LTPA, OPA and CA. bAdjusted for age, area, year of survey, education, smoking, BMI, alcohol intake, LTPA, OPA and CA (analysis included only the surveys between 1987 and 1997). cAdjusted for age, area, year of survey, education, smoking, alcohol intake, BMI, LTPA, OPA and CA; individuals using antihypertensive drug treatment were excluded. dAdjusted for age, area, year of survey, education, smoking, BMI, alcohol intake, total cholesterol/HDL-cholesterol, LTPA, OPA and CA.
In accordance with our findings, many previous studies reported an inverse association between leisure-time physical activity and total serum cholesterol among men [13,17,22,24,26,49,50]. However, in contrast to our study, they failed to show a significant association among women [25,50]. The observations of the few studies investigating the association between occupational physical activity and HDL-cholesterol levels have been less consistent. The results vary from a positive relationship [12,14] to no relationship at all [13,15]. Walking has been shown to affect serum lipid levels [51,52], and commuting activity was observed to be inversely related to total serum cholesterol among men and positively with HDL-cholesterol in a cross-sectional study among Chinese women [30].
Several reasons may explain why the cholesterol level among both men and women was highest in the groups with high occupational physical activity. Individuals with high occupational physical activity may belong to a lower socio-economic class, and using education as an indicator of socio-economic status may only partly reflect the socio-economic level. Nevertheless, it is unlikely that these results are the result of differences in socioeconomic factors alone. Another possible reason for the observations of our study may be differences in dietary habits among the group with the highest occupational physical activity compared with the group with the lowest physical activity. The correlation coefficient between cholesterol and education was – 0.308, indicating that dietary habits may differ among educational levels.
One of the main strengths of our study was that our analyses were conducted among large, representative population samples of middle-aged men and women. The participation rates were high, which makes it possible to apply the results directly to the general population. Furthermore, this is to our knowledge the first study to analyse separately the associations of different forms of physical activity with cardiovascular risk factors. In addition, we were able to adjust our results for the most important risk factors of CVD.
Naturally, our study had some limitations. Its cross-sectional design cannot prove any causal relationship between physical activity and cardiovascular risk factors. Furthermore, we could neither adjust for all potential important variables such as stress and potassium or sodium intake. The lack of information on dietary habits may also be a limitation. Dietary habits are closely related to many cardiovascular risk factors such as BMI, waist circumference, blood pressure, HDL-cholesterol and total cholesterol. We would also like to point out that we divided physical activity into categories and provided a ranking, but not information about the intensity or optimal doses of activity. Quantitative measurements of physical activities are very difficult to conduct in large population studies; however, the questionnaire used for the assessment of physical activity has been successfully used elsewhere [5,7,9,50,53], and it has been validated in the ‘Seven Countries Study’ [39].
In conclusion, not only leisure-time physical activity, but also commuting activity is associated with reduced levels of some cardiovascular risk factors (BMI, waist circumference, HDL-cholesterol). Whereas some individuals could increase their physical activity in leisure time, others may gain a health benefit from being more physically active on their way to work. Therefore, all forms of physical activity should be promoted to reduce CVD in the general population.